(UroToday.com) The 2026 American Society of Clinical Oncology (ASCO) Annual Meeting was host to a prostate, testicular, and penile cancers rapid oral abstracts session. Dr. Fred Saad presented the results of subgroup analyses by disease volume and timing (de novo versus recurrent) from the PSMAddition study of [177Lu]Lu-PSMA-617] in the metastatic hormone-sensitive prostate cancer (mHSPC) setting.
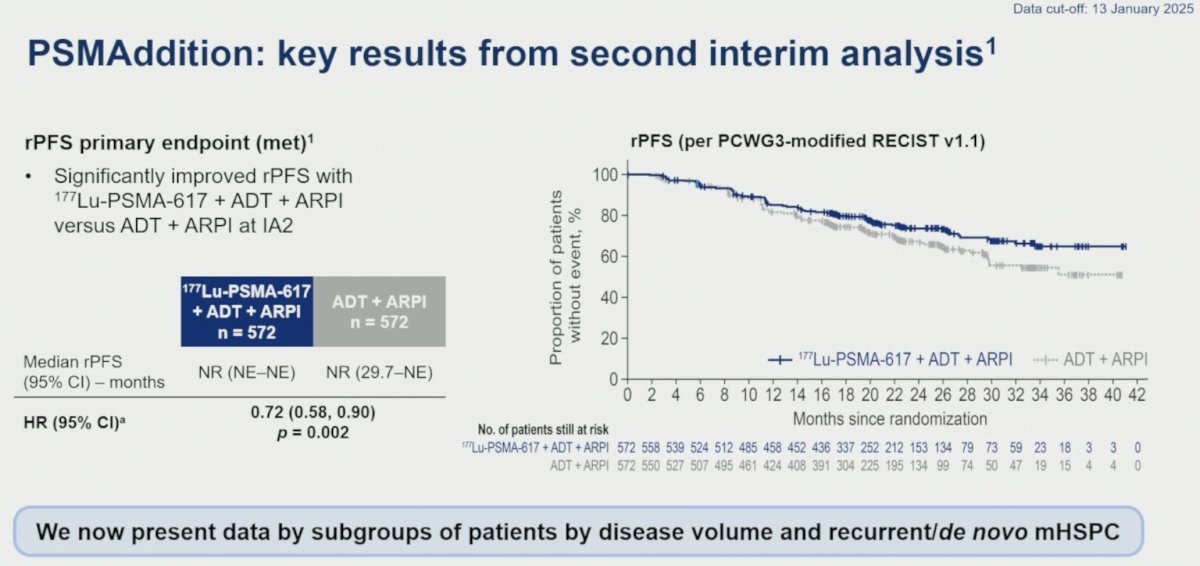
As previously reported at ESMO 2025, PSMAddition met its primary endpoint, demonstrating a significant improvement in radiographic progression-free survival (rPFS) with [¹⁷⁷Lu]Lu-PSMA-617 + ADT + ARPI versus ADT + ARPI alone (HR: 0.72, 95% CI: 0.58–0.90; p=0.002).1
PSMAddition is a phase III trial that enrolled patients with PSMA-positive mHSPC diagnosed by conventional imaging and ≥1 PSMA-positive metastatic lesion on ⁶⁸Ga-PSMA-11 PET/CT. Eligible patients were untreated or minimally treated, had an ECOG performance status of 0–2, and were candidates for ADT + ARPI. Patients were randomized 1:1 to:
- [¹⁷⁷Lu]Lu-PSMA-617 (7.4 GBq ±10%) every 6 weeks for 6 cycles plus ADT + ARPI
- ADT + ARPI alone
The primary endpoint was rPFS, with overall survival (OS) as a key secondary endpoint. Crossover to [¹⁷⁷Lu]Lu-PSMA-617 was permitted following blinded independent central review (BICR)-confirmed radiographic progression. At the second interim analysis, the median follow-up was 23.6 months (range: 17.7–42.8).![The primary endpoint was rPFS, with overall survival (OS) as a key secondary endpoint. Crossover to [¹⁷⁷Lu]Lu-PSMA-617 was permitted following blinded independent central review (BICR)-confirmed radiographic progression. At the second interim analysis, the median follow-up was 23.6 months (range: 17.7–42.8).](/images/com-doc-importer/271-asco-2026/asco-2026-subgroup-analyses-by-disease-volume-and-de-novo-recurrent-mhspc-in-the-psmaddition-study-of-177lu-lu-psma-617/image-1.jpg)
Disease volume was defined according to CHAARTED criteria (high-volume: visceral metastases and/or ≥4 bone lesions with ≥1 lesion beyond the vertebral bodies and pelvis). mHSPC timing was classified by status at presentation (de novo: stage IVB disease at initial diagnosis).
Baseline characteristics were generally balanced across treatment arms within each subgroup. High-volume disease was present in approximately 68% of patients (389/572 and 390/572 in the experimental and control arms, respectively), while 52% of patients had de novo disease.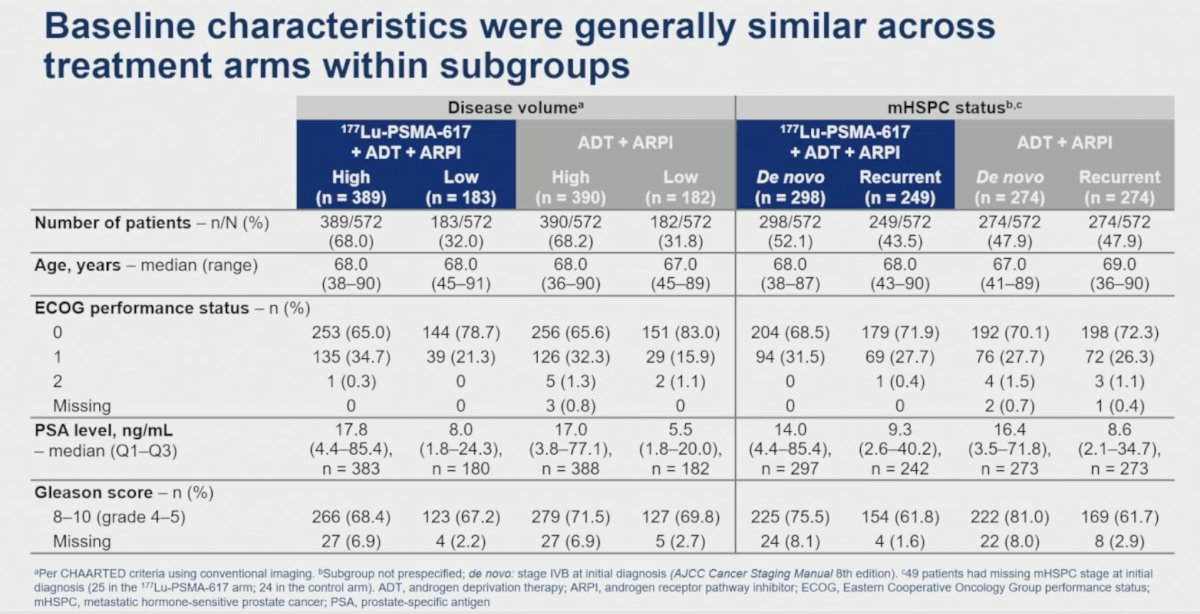
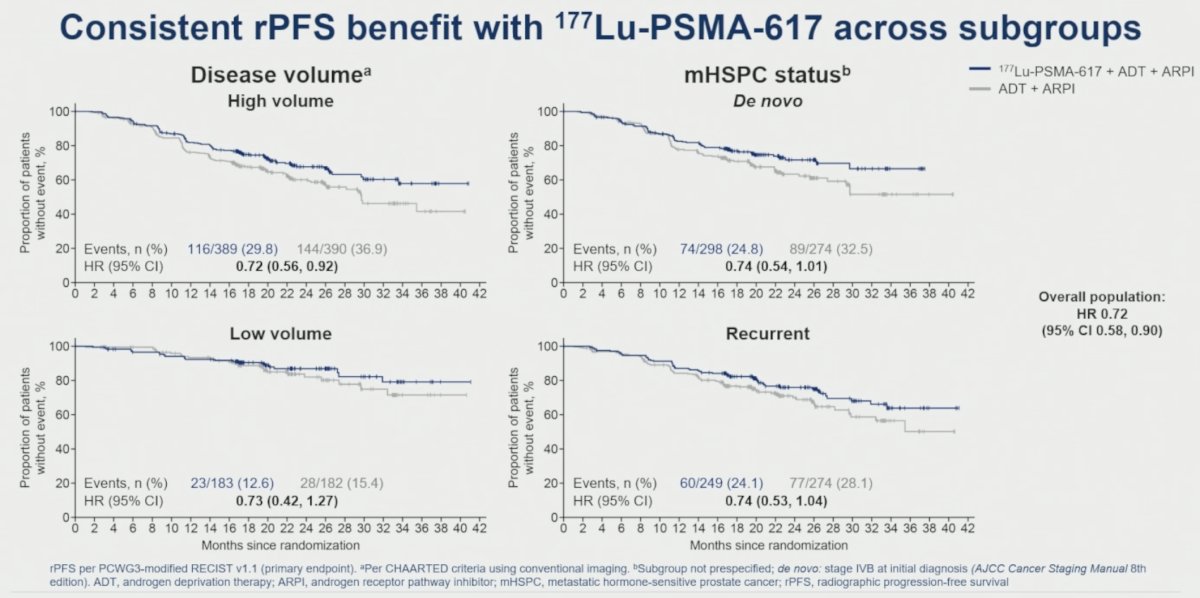
The rPFS benefit observed in the overall study population was maintained across all disease volume and disease status subgroups, as follows:
- Disease volume:
- High-volume: HR= 0.72 (95% CI: 0.56–0.92)
- Low-volume: HR= 0.73 (95% CI: 0.42–1.27)
- mHSPC status:
- De novo disease: HR= 0.74 (95% CI: 0.54–1.01)
- Recurrent: HR= 0.74 (95% CI: 0.53–1.04)
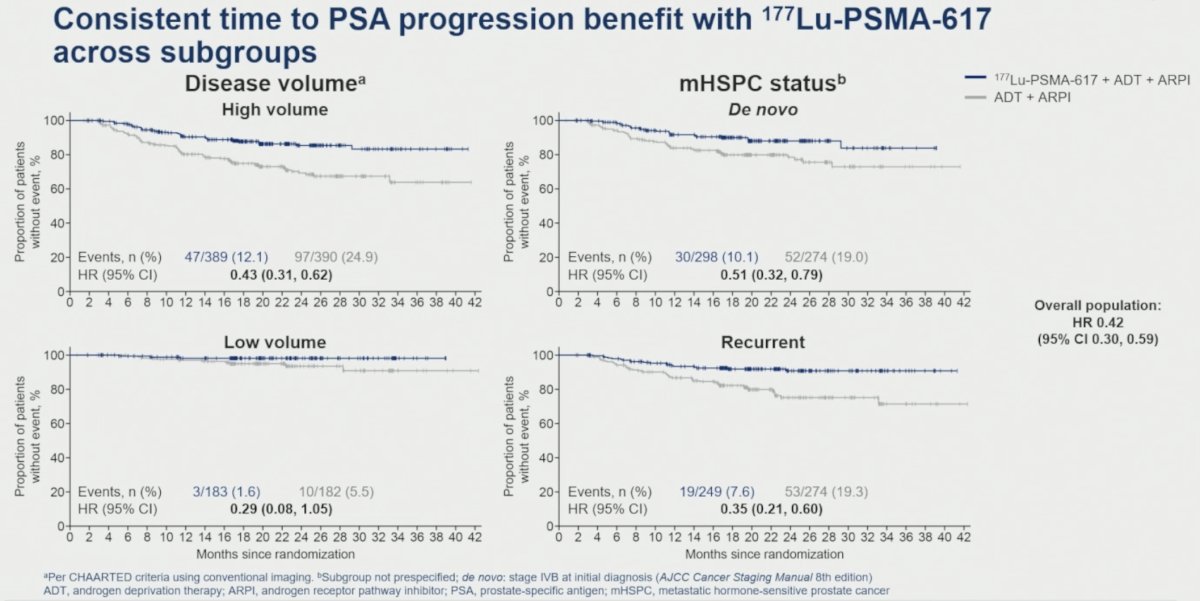
A consistent benefit was also observed for time to PSA progression:
- Disease volume:
- High-volume: HR= 0.43 (95% CI: 0.31–0.62)
- Low-volume: HR= 0.29 (95% CI: 0.08–1.05)
- mHSPC status:
- De novo: HR= 0.51 (95% CI: 0.32–0.79)
- Recurrent: HR= 0.35 (95% CI: 0.21–0.60)
The time to development of metastatic castration-resistant prostate cancer (mCRPC) similarly favored the [¹⁷⁷Lu]Lu-PSMA-617 arm across all subgroups:
- Disease volume:
- High-volume: HR= 0.67 (95% CI: 0.54–0.82)
- Low-volume: HR= 0.87 (95% CI: 0.55–1.37)
- mHSPC status:
- De novo: HR= 0.61 (95% CI: 0.47–0.80)
- Recurrent: HR= 0.75 (95% CI: 0.56–1.00)
![The time to development of metastatic castration-resistant prostate cancer (mCRPC) similarly favored the [¹⁷⁷Lu]Lu-PSMA-617 arm across all subgroups:](/images/com-doc-importer/271-asco-2026/asco-2026-subgroup-analyses-by-disease-volume-and-de-novo-recurrent-mhspc-in-the-psmaddition-study-of-177lu-lu-psma-617/image-5.jpg)
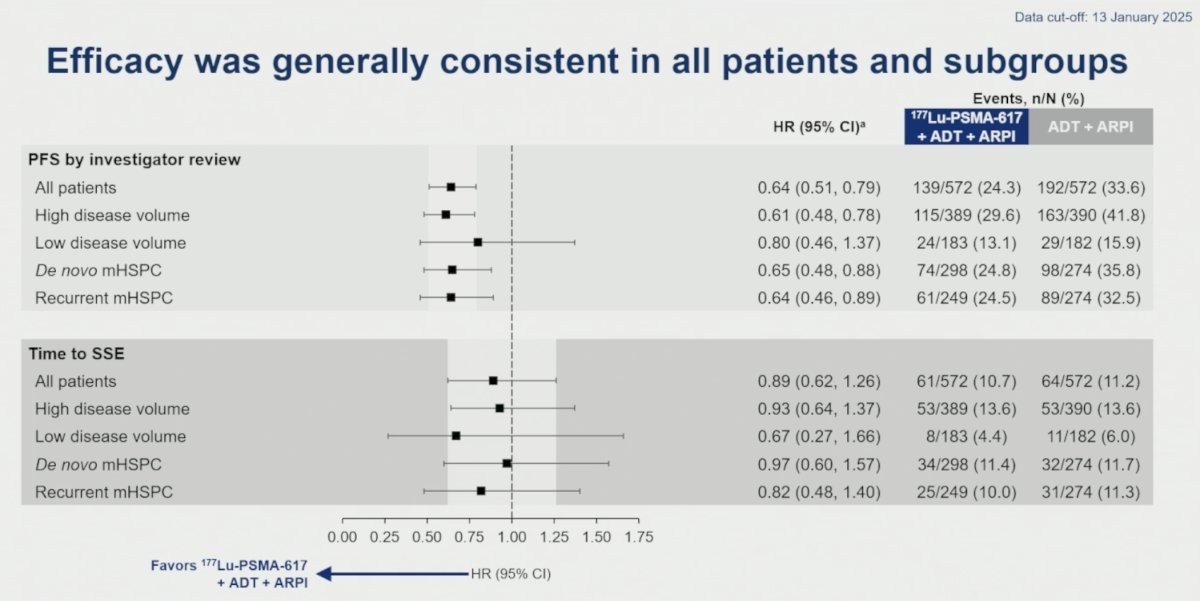
PFS by investigator review demonstrated results consistent with the primary analysis:
- Overall population: HR 0.64 (95% CI: 0.51–0.79)
- High-volume disease: HR 0.61 (95% CI: 0.48–0.78)
- Low-volume disease: HR 0.80 (95% CI: 0.46–1.37)
- De novo disease: HR 0.65 (95% CI: 0.48–0.88)
- Recurrent disease: HR 0.64 (95% CI: 0.46–0.89)
Time to symptomatic skeletal events (SSEs) was generally similar across subgroups and consistent with the overall population:
- Overall population: HR 0.89 (95% CI: 0.62–1.26)
- High-volume disease: HR 0.93 (95% CI: 0.64–1.37)
- Low-volume disease: HR 0.67 (95% CI: 0.27–1.66)
- De novo disease: HR 0.97 (95% CI: 0.60–1.57)
- Recurrent disease: HR 0.82 (95% CI: 0.48–1.40)
Patient-Reported Outcomes
Patient-reported outcomes (PRO) analyses demonstrated similar treatment effects across disease volume and disease status subgroups.
For the time to FACT-P total score worsening:
- Overall population: HR 1.14 (95% CI: 0.98–1.33)
- High-volume disease: HR 1.13 (95% CI: 0.94–1.37)
- Low-volume disease: HR 1.16 (95% CI: 0.88–1.53)
- De novo disease: HR 1.13 (95% CI: 0.90–1.41)
- Recurrent disease: HR 1.16 (95% CI: 0.92–1.46)
For the time to EQ-5D-5L utility score worsening:
- Overall population: HR 1.13 (95% CI: 0.97–1.31)
- High-volume disease: HR 1.04 (95% CI: 0.87–1.25)
- Low-volume disease: HR 1.34 (95% CI: 1.01–1.77)
- De novo disease: HR 1.17 (95% CI: 0.93–1.45)
- Recurrent disease: HR 1.09 (95% CI: 0.87–1.37)
For the time to Brief Pain Inventory–Short Form (BPI-SF) pain intensity worsening:
- Overall population: HR 1.02 (95% CI: 0.87–1.18)
- High-volume disease: HR 0.98 (95% CI: 0.82–1.18)
- Low-volume disease: HR 1.09 (95% CI: 0.83–1.44)
- De novo disease: HR 1.06 (95% CI: 0.85–1.31)
- Recurrent disease: HR 0.97 (95% CI: 0.78–1.22)

Longitudinal analyses of PROs in the overall population showed generally similar trajectories between treatment arms for FACT-P total score, EQ-5D-5L utility score, and BPI-SF pain intensity throughout follow-up.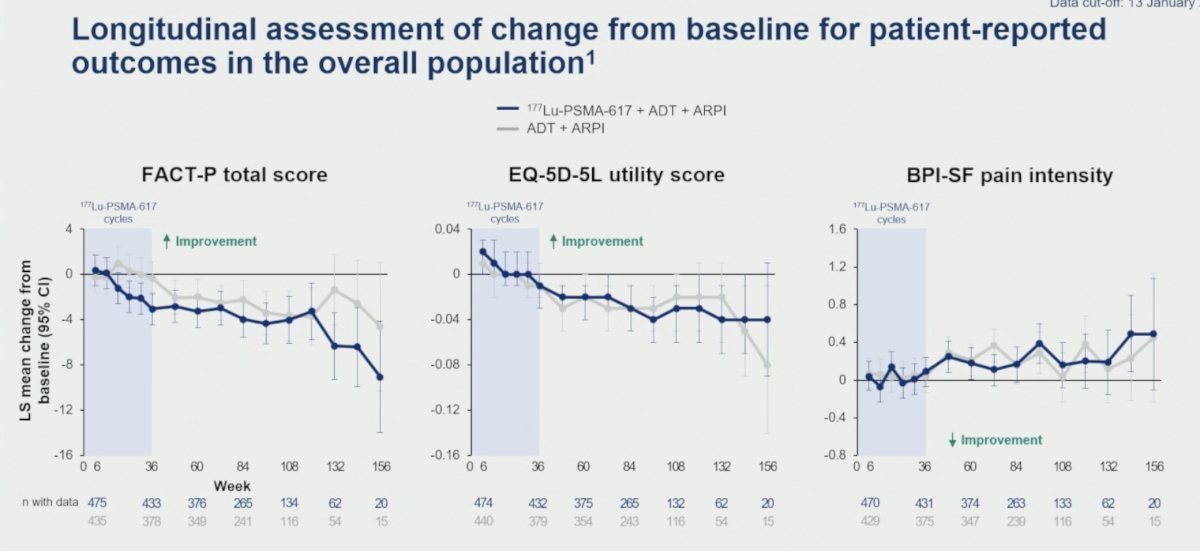
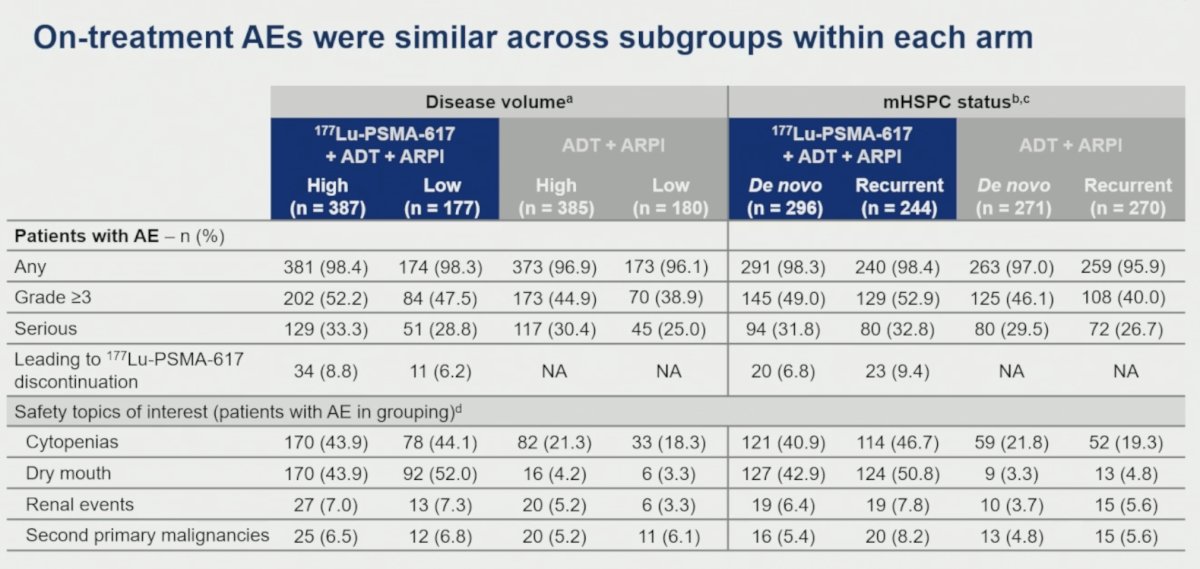
With regards to safety, on-treatment adverse events (AEs), including those of special interest (cytopenias, dry mouth, renal events, second primary malignancies) were generally similar across disease volume and mHSPC status subgroups within each treatment arm.
Dr. Saad concluded his presentation of the PSMAddition subgroup analyses as follows:
- Combining ¹⁷⁷Lu-PSMA-617 with ADT + ARPI provided a similar magnitude of rPFS benefit versus ADT + ARPI across high and low disease volume and de novo and recurrent mHSPC subgroups.
- Other efficacy and patient-reported outcome HRs for the ¹⁷⁷Lu-PSMA-617 vs control arm for each disease volume and mHSPC status subgroup were generally similar across subgroups and to the overall population.
- The safety profile was generally consistent across subgroups within each treatment arm, with similar incidences of AEs, grade ≥3 AEs, and selected safety topics of interest (cytopenias, dry mouth).
- In patients with PSMA+ mHSPC, the efficacy, patient-reported outcomes, and safety profile of ¹⁷⁷Lu-PSMA-617 combined with ADT + ARPI were consistent across clinically relevant disease volume and mHSPC status subgroups.
Presented by: Fred Saad, CQ, MD, FRCS, FCAHS, Professor, Department of Surgery, Raymond Garneau Chair in Prostate Cancer, Director of Prostate Cancer Research, Director of GU Oncology, Université de Montréal, University of Montreal Hospital Centers, CRCHUM, Montréal, QC
Written by: Rashid K. Sayyid, MD, MSc, Assistant Professor, Urologic Oncologist, Department of Urology at The University of Arizona and Banner University Medical Center, Tucson, AZ – @rksayyid on X during the American Society of Clinical Oncology Genitourinary (ASCO) Annual Meeting held in Chicago, IL between May 29th and June 1st, 2026
References:
- Tagawa ST, Sartor O, Piulats JM, Saad F, Fizazi K, Reid AHM, et al. Phase III trial of [177Lu]Lu-PSMA-617 combined with ADT plus ARPI in patients with PSMA-positive metastatic hormone-sensitive prostate cancer (PSMAddition). Ann Oncol. 2025;36(Suppl 2):S1627-S1628.