(UroToday.com) The 2026 American Society of Clinical Oncology (ASCO) Annual Meeting was host to a prostate, testicular, and penile cancers rapid oral abstracts session. Dr. Kim Chi presented an analysis of the Canadian Cancer Trials Group (CCTG) study PR21 (PLUDO) evaluating the impact of treatment crossover in metastatic castrate-resistant prostate cancer (mCRPC) patients randomized to 177Lu-PSMA-617 versus docetaxel.
The PLUDO trial was designed to address an increasingly relevant clinical question in mCRPC management: how best to sequence 177Lu-PSMA-617 and docetaxel in patients progressing following androgen receptor pathway inhibitor (ARPI) therapy. In the primary analysis previously presented at ESMO 2025, patients with ARPI pre-treated mCRPC were randomized to receive either 177Lu-PSMA-617 or docetaxel. While no significant difference was observed in the primary endpoint of radiographic progression-free survival (rPFS1; HR 1.01, 90% CI 0.77–1.31), overall survival favored patients randomized to docetaxel first (HR 1.64, 95% CI 1.14–2.35). However, this result was potentially confounded by an imbalance in crossover, prompting the current preplanned analysis evaluating outcomes among patients who received both therapies.
This trial included PSMA PET-positive mCRPC patients with disease progression following prior ARPI therapy. Prior docetaxel for mHSPC was permitted if administered ≥12 months earlier.
Patients were randomized 1:1 to:
- 177Lu-PSMA-617 7.4 GBq IV every 6 weeks for 6 cycles
- Docetaxel 75 mg/m2 IV every 3 weeks for 12 cycles
Following radiographic progression (rPFS1), patients were permitted to crossover to the alternate therapy. Additional study objectives included overall survival, rPFS2, PSA decline, adverse events, patient-reported quality of life, and correlative studies.
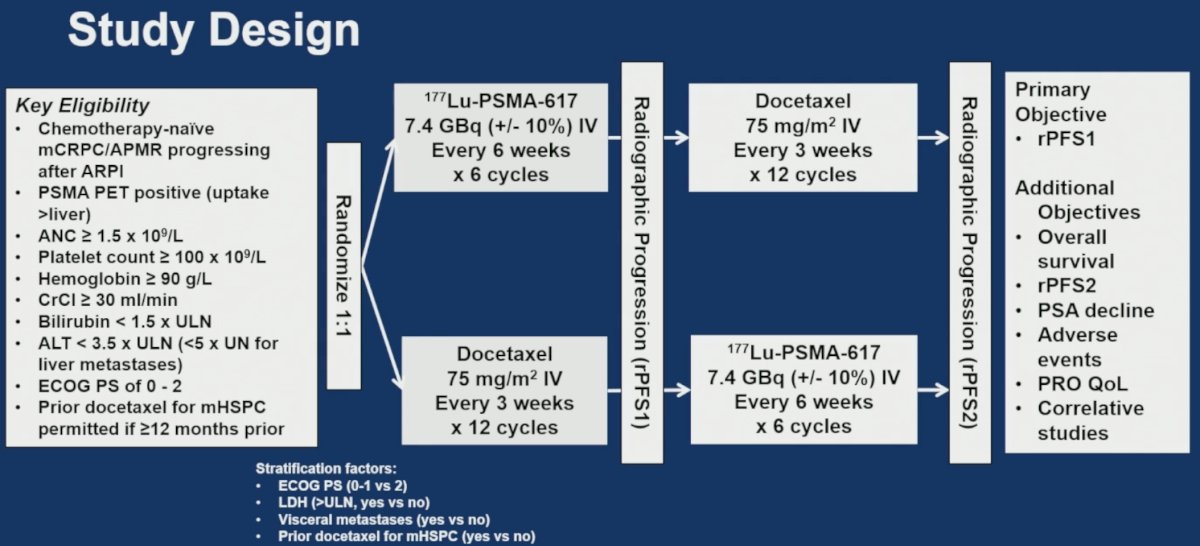
The study flow chart is illustrated below. A total of 199 patients were randomized to 177Lu-PSMA-617 (n=100) and docetaxel (n=99). At radiographic progression, 42/79 (53.2%) patients in the 177Lu-PSMA-617 arm crossed over to docetaxel, and 62/99 (62.6%) patients in the docetaxel arm crossed over to 177Lu-PSMA-617.
To better understand this imbalance, the investigators examined quality-of-life and adverse event outcomes at the time of first radiographic progression. The mean FACT-P total scores at rPFS1 favored LuPSMA-treated patients:
- LuPSMA: 114 (SD 20.7)
- DOC: 103 (SD 21.6)
The investigators concluded that the lower crossover rate from LuPSMA to docetaxel was unlikely to be explained by worse quality of life or treatment-related toxicity.
The baseline characteristics at crossover were generally similar between treatment sequences:
- Median age: 69 years (LuPSMA→DOC) versus 71 years (DOC→LuPSMA)
- Liver metastases: 10% versus 3%
- Median hemoglobin: 116 versus 118 g/L
- Median alkaline phosphatase: 179 versus 175 U/L
- Median LDH: 289 versus 268 U/L
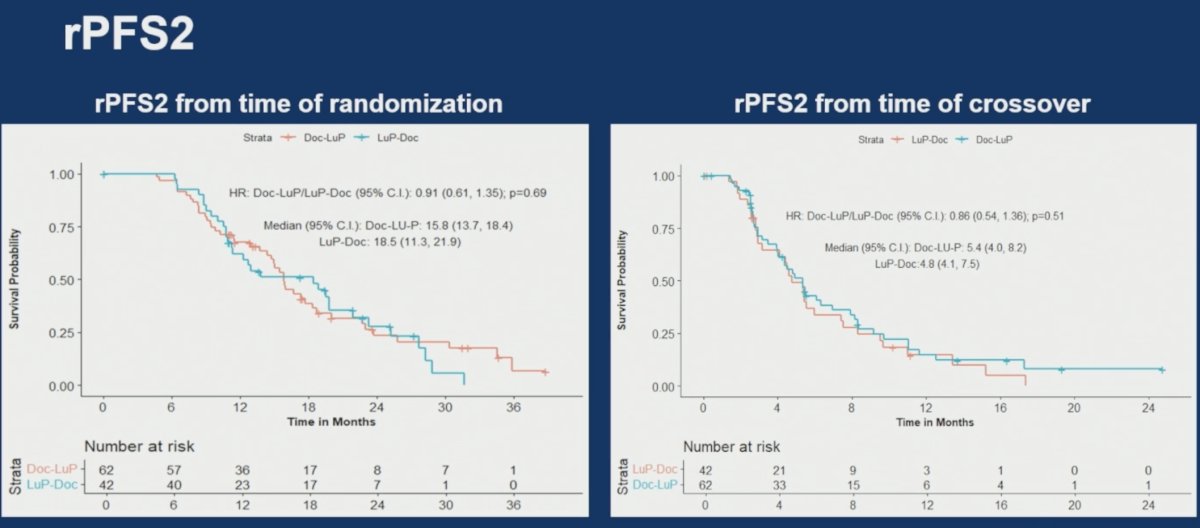
The key efficacy endpoint of this analysis was rPFS2. From the time of randomization:
- LuPSMA→DOC: 18.5 months (95% CI 11.3–21.9)
- DOC→LuPSMA: 15.8 months (95% CI 13.7–18.4)
- HR 0.91 (95% CI 0.61–1.35), p=0.69
From the time of crossover:
- LuPSMA→DOC: 4.8 months
- DOC→ LuPSMA: 5.4 months
- HR 0.86 (95% CI 0.54–1.36), p=0.51
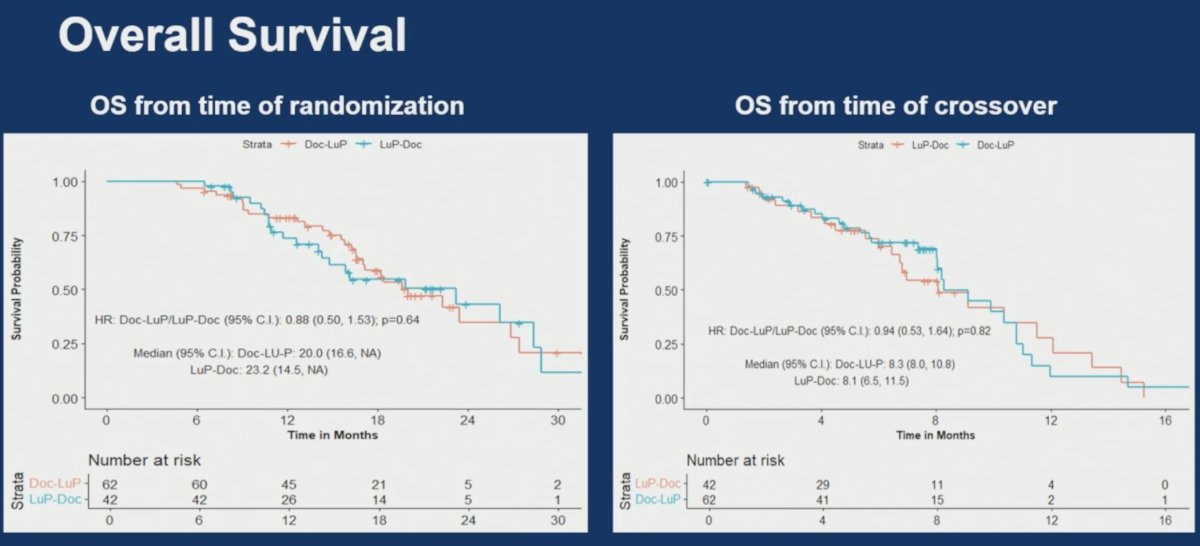
Overall survival analyses likewise demonstrated no significant differences between treatment sequences. From the time of randomization:
- LuPSMA →DOC : 23.2 months (95% CI 14.5–not estimable)
- DOC→ LuPSMA: 20 months (95% CI 16.6–not estimable)
- HR 0.88 (95% CI 0.50–1.53), p=0.64
From the time of crossover:
- LuPSMA →DOC: 8.1 months (95% CI 6.5–11.5)
- DOC→ LuPSMA: 8.3 months (95% CI 8.0–10.8)
- HR 0.94 (95% CI 0.53–1.64), p=0.82
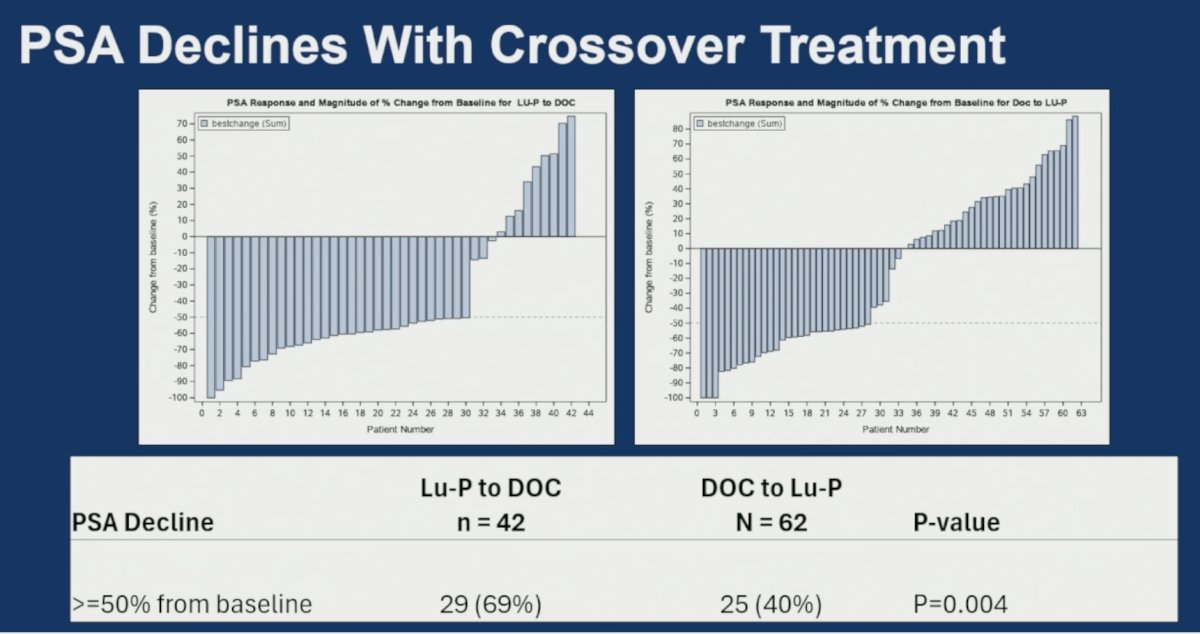
PSA responses were observed with both crossover strategies. A PSA decline ≥50% from baseline occurred in:
- LuPSMA DOC: 29/42 patients (69%)
- DOC LuPSMA: • 25/62 patients (40%)
- p=0.004
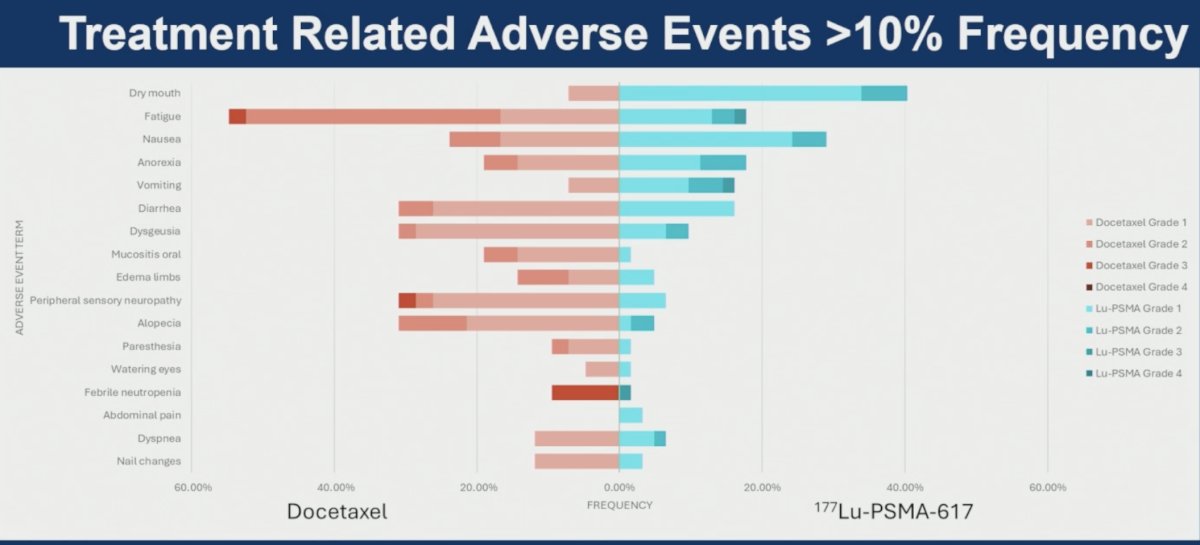
Treatment-related adverse events in the crossover setting were consistent with previously reported safety profiles for both therapies. Among adverse events occurring in >10% of patients:
- LuPSMA was associated more frequently with dry mouth, nausea, anorexia, and vomiting
- Docetaxel was associated more frequently with fatigue, diarrhea, dysgeusia, alopecia, peripheral sensory neuropathy, paresthesia, and febrile neutropenia
Laboratory treatment-emergent adverse events were also consistent with known toxicity profiles of each treatment.
Dr. Chi concluded his presentation with the following key messages:
- The imbalance in crossover, with fewer patients crossing from LuPSMA→DOC than DOC→LuPSMA, does not appear to be related to worse quality of life or adverse events at the time of first progression
- Among patients who received both treatments, there were no significant differences in rPFS or overall survival between the sequencing strategies of LuPSMA followed by docetaxel versus docetaxel followed by LuPSMA
- In the crossover setting, PSA declines and adverse events were consistent with those previously reported for both LuPSMA and docetaxel
- Collectively, the PR21/PLUDO study supports the use of both 177Lu-PSMA-617 and docetaxel in patients with mCRPC/APMR progressing after ARPI therapy
Presented by: Kim N. Chi, MD, Vice President & Chief Medical Officer, British Columbia Cancer Agency, Vancouver Cancer Centre, Vancouver, Canada
Written by: Rashid K. Sayyid, MD, MSc, Assistant Professor, Urologic Oncologist, Department of Urology at The University of Arizona and Banner University Medical Center, Tucson, AZ – @rksayyid on X during the American Society of Clinical Oncology Genitourinary (ASCO) Annual Meeting held in Chicago, IL between May 29th and June 1st, 2026
References:- Chi KN, Saad F, Ding K, Bauman G, Emmenegger U, Hotte SJ, et al. A randomized phase II study of 177Lu-PSMA-617 vs docetaxel in patients with metastatic castration-resistant prostate cancer (mCRPC) and PSMA-positive disease: Canadian Cancer Trials Group (CCTG) study PR.21. Ann Oncol. 2025;36(Suppl 2):LBA89.