(UroToday.com) The 2026 American Society of Clinical Oncology (ASCO) Annual Meeting was host to a prostate, testicular, and penile cancers rapid oral abstracts session. Dr. Corinne Maurice-Dror presented PROTRACT, a randomized phase II trial comparing ctDNA-guided biomarker-directed therapy versus patient/clinician's choice for metastatic castrate-resistant prostate cancer progressing after abiraterone acetate + prednisone.
Sequential use of androgen receptor pathway inhibitors (ARPIs) remains common in clinical practice despite recognized cross-resistance, underscoring patients’ preference to delay or avoid chemotherapy. Prior studies have demonstrated that the circulating tumor DNA (ctDNA) fraction is an independent prognostic biomarker in prostate cancer, with lower ctDNA fractions associated with improved outcomes among patients receiving enzalutamide following a prior ARPI, but not with docetaxel after 1st line ARPI. The PROTRACT trial aimed to evaluate whether ctDNA-guided treatment selection could improve outcomes compared with standard physician/patient-directed treatment selection in chemotherapy-naïve patients with metastatic castration-resistant prostate cancer (mCRPC) progressing after abiraterone acetate plus prednisone (AAP).
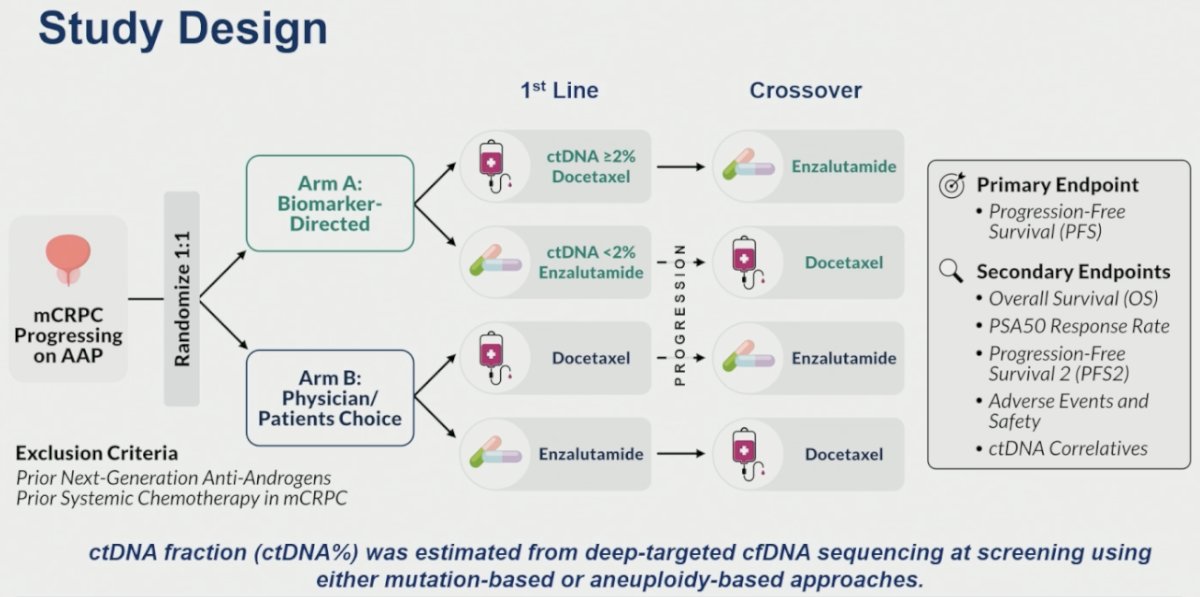
PROTRACT was a randomized phase II trial enrolling mCRPC patients progressing on AAP, who had not received systemic chemotherapy in the castrate-resistant state nor prior next-generation anti-androgens. Eligible patients were randomized 1:1 to:
- Arm A (biomarker-directed therapy): treatment assignment based on baseline ctDNA fraction
- ctDNA ≥2%: docetaxel
- ctDNA <2%: enzalutamide
- Arm B (physician/patient preference): treatment selected according to routine clinical decision-making
Importantly, at progression, crossover to the alternate treatment was permitted.
The primary endpoint was progression-free survival (PFS). The secondary endpoints were:
- Overall survival (OS)
- PSA50 response rate
- Progression-free survival 2 (PFS2)
- Adverse events and safety
- ctDNA correlatives.
ctDNA fraction was estimated from deep-targeted cfDNA sequencing using mutation-based or aneuploidy-based approaches.
Between October 2020 and June 2025, 56 patients were screened, and 42 were randomized. Among randomized patients:
- Biomarker-directed arm (n=17)
- Docetaxel: n=11 (ctDNA ≥2%)
- Enzalutamide: n=6 (ctDNA <2%)
- Patient preference arm (n=25)
- Docetaxel: n=4
- ctDNA ≥2%: n=3
- ctDNA <2%: n=1
- Enzalutamide: n=21
- ctDNA ≥2%: n=14
- ctDNA <2%: n=7
- Docetaxel: n=4
The study was terminated early because of slow accrual prior to reaching the planned enrollment of 100 patients.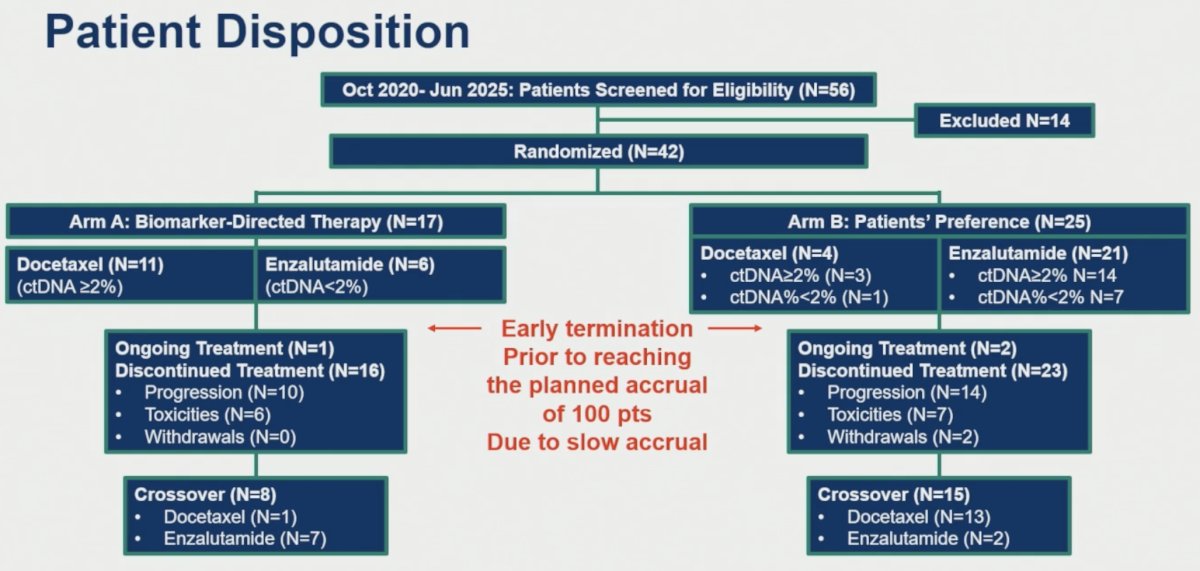
At data cutoff (January 2026), treatment remained ongoing in 1 patient in Arm A and 2 patients in Arm B. Treatment discontinuation occurred in 16 and 23 patients, respectively, primarily because of disease progression and toxicity. Crossover occurred in 8 patients in Arm A and 15 patients in Arm B.
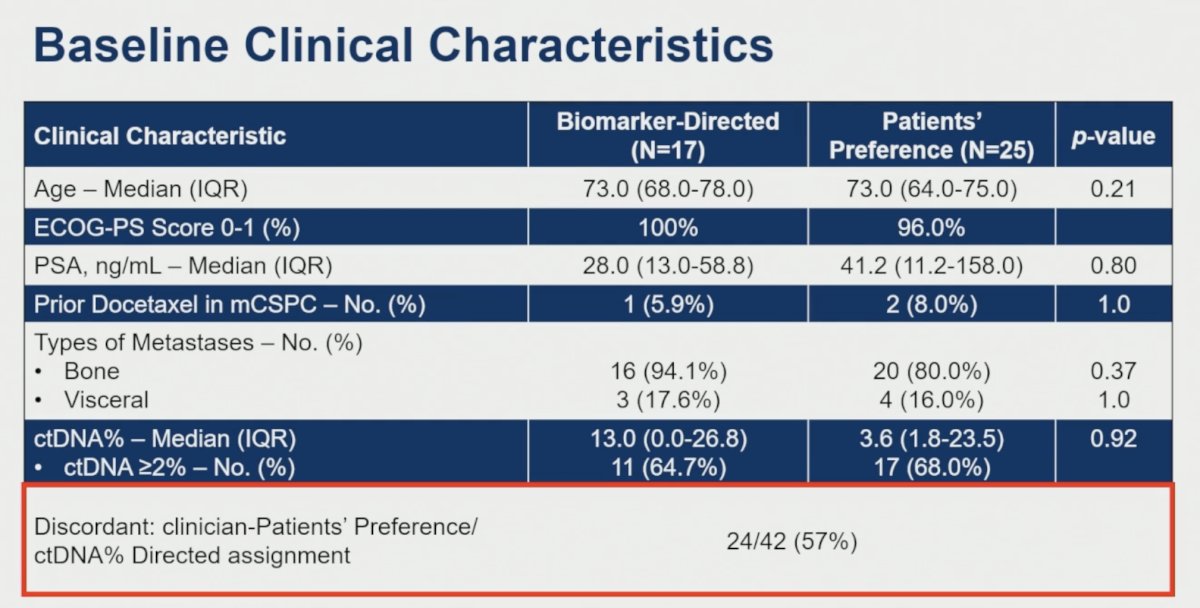
The baseline characteristics were balanced between groups. The median age was 73 years in both arms. The median PSA was comparatively lower in the biomarker-directed arm (28 vs 41.2 ng/ml). Six to eight percent of patients had received prior docetaxel in the mCSPC setting. Bone metastases were present in 80–94% of patients, and visceral metastases in 16–17.6%. The median ctDNA% was 13 in the biomarker-directed arm and 3.6 in the patients’ preference arm. The percentages of patients with ctDNA fraction ≥2% were 65% and 68%, respectively (p=0.92). Importantly, treatment assignment according to ctDNA-guided selection was discordant with physician/patient preference in 24 of 42 patients (57%), highlighting the potential clinical impact of biomarker-informed treatment selection.
The primary endpoint of PFS was significantly improved with ctDNA-guided treatment selection, with median PFS, as follows:
- Biomarker-directed arm: 5.6 months (95% CI 3.2–8.2)
- Patient preference arm: 2.5 months (95% CI 1.5–3.7)
- HR 0.38 (95% CI 0.19–0.76), p=0.01
Swimmer plot analyses demonstrated longer durations of response among patients treated according to ctDNA-guided assignment.
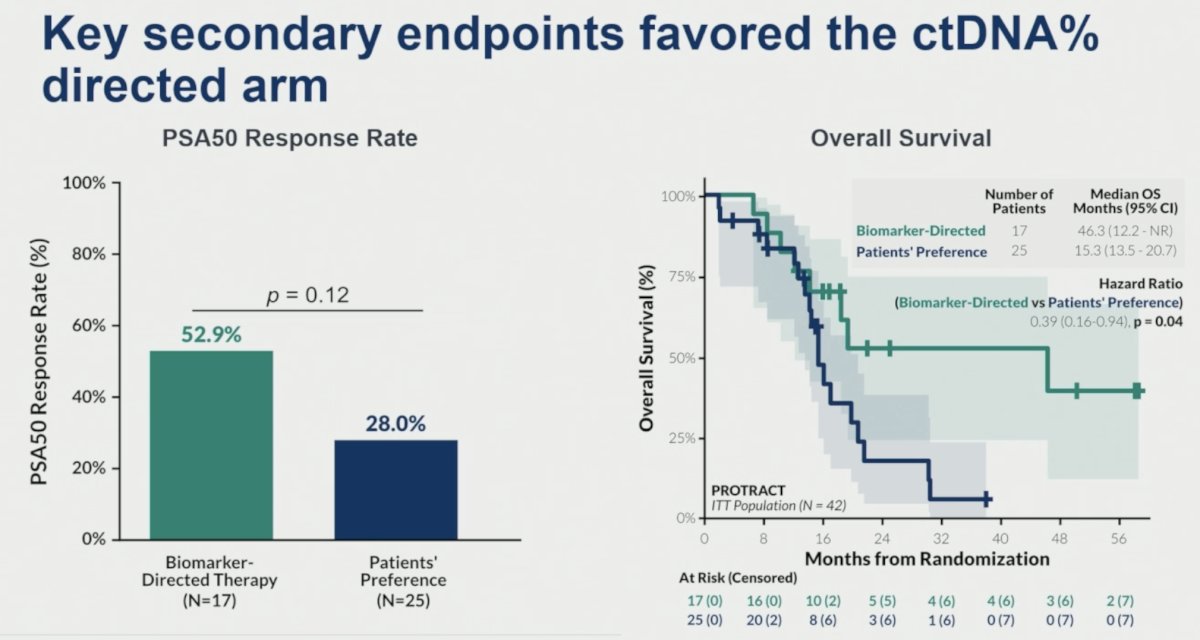
The key secondary endpoints favored the ctDNA%-directed arm:
- PSA50 response
- Biomarker-directed arm: 52.9%
- Patient preference arm: 28%
- p=0.12
- Overall survival (medians)
- Biomarker-directed arm: 46.3 months (95% CI 12.2–NR)
- Patient preference arm: 15.3 months (95% CI 13.5–20.7)
- HR 0.39 (95% CI 0.16–0.94), p=0.04
The safety profile was consistent with the expected toxicities of docetaxel and enzalutamide, with no new safety signals identified. Adverse events were more common and more severe among patients receiving docetaxel compared to those receiving enzalutamide. In the biomarker-directed arm, grade ≥3 adverse events occurred in 63.6% of docetaxel-treated patients compared with none of the enzalutamide-treated patients. Treatment discontinuation due to adverse events was also more frequent with docetaxel (54.5% versus 0%).
Similarly, in the patient-preference arm, adverse events leading to treatment discontinuation were observed in 50% of docetaxel-treated patients and 23.8% of enzalutamide-treated patients. Serious adverse events were uncommon across treatment groups.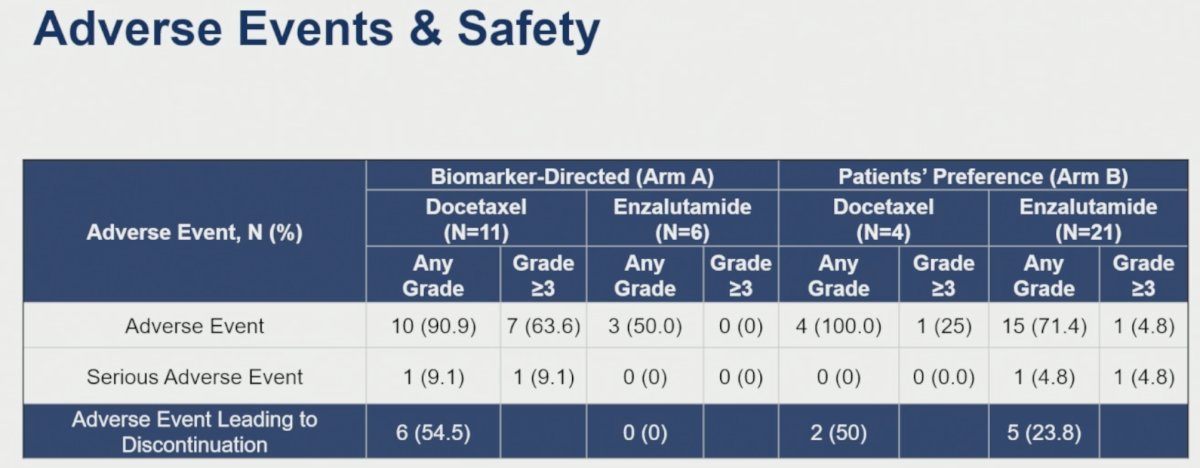
Overall, these findings suggest that the improved efficacy observed with ctDNA-guided treatment selection was achieved without unexpected safety concerns, and the observed toxicities were consistent with the known safety profiles of the individual therapies.
Dr. Corinne Maurice-Dror concluded her presentation of the PROTRACT trial as follows:
- The PROTRACT results highlight the potential clinical utility of ctDNA% as a predictive biomarker to guide treatment selection in patients with mCRPC, resulting in improved outcomes compared with clinician/patient-directed treatment choice.
- The data support the inclusion of ctDNA% as an integrated and integral biomarker in clinical trials for patients with advanced prostate cancer.
Presented by: Corinne Maurice-Dror, MD, Clinical Assistant Professor, Division of Medical Oncology, University of British Columbia, Vancouver, BC, Canada
Written by: Rashid K. Sayyid, MD, MSc, Assistant Professor, Urologic Oncologist, Department of Urology at The University of Arizona and Banner University Medical Center, Tucson, AZ – @rksayyid on X during the American Society of Clinical Oncology Genitourinary (ASCO) Annual Meeting held in Chicago, IL between May 29th and June 1st, 2026