(UroToday.com) The 2026 American Society of Clinical Oncology (ASCO) Annual Meeting was host to a prostate, testicular, and penile cancers rapid oral abstracts session. Dr. Susan Halabi presented an analysis from Alliance A031201 evaluating a circulating tumor DNA (ctDNA)-based clinical-genetic prognostic model for radiographic progression-free survival (rPFS) in patients with metastatic castration-resistant prostate cancer (mCRPC).
Dr. Halabi noted that rPFS is a routinely utilized and clinically meaningful endpoint in mCRPC clinical trials. Importantly, rPFS often informs clinical management decisions and treatment changes, which can impact patient morbidity. While existing prognostic models incorporate clinical variables, they do not account for tumor genomic characteristics, limiting predictive accuracy. Given that ctDNA provides a non-invasive and readily available measure of tumor burden and genomic alterations, Dr. Halabi and colleagues sought to develop and validate a clinical-genetic model integrating ctDNA-derived genomic features with clinical variables to improve the prediction of rPFS in men with mCRPC.
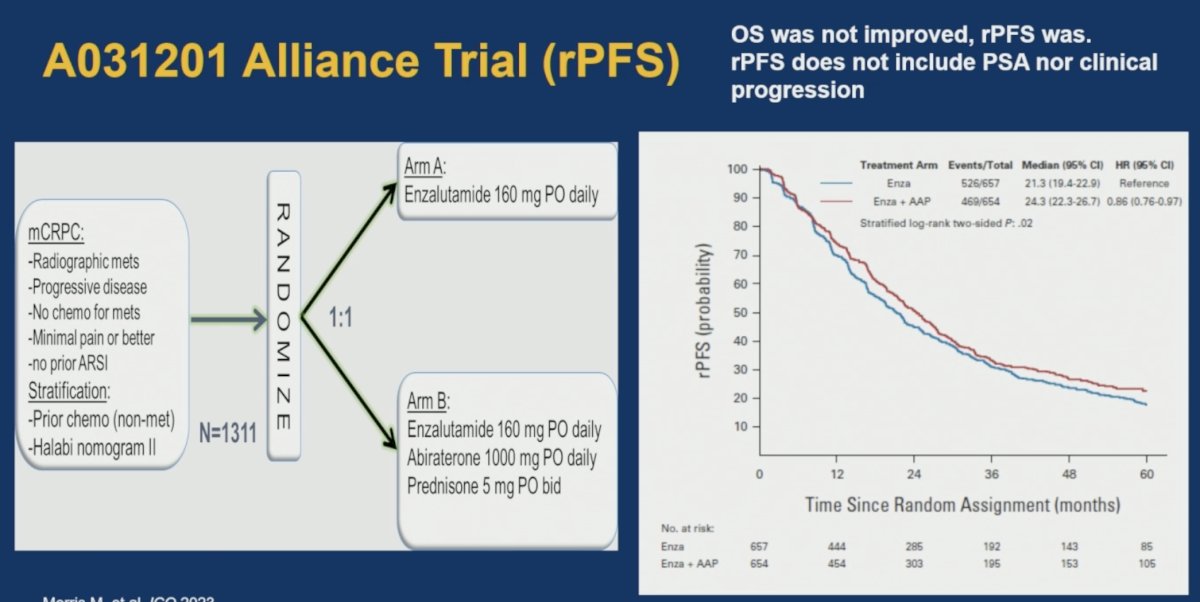
The analysis was based on the Alliance A031201 phase III trial, which enrolled 1,311 men with mCRPC and randomized them 1:1 to:
- Enzalutamide alone
- Enzalutamide plus abiraterone acetate and prednisone
Although the combination arm improved rPFS compared with enzalutamide alone, it did not improve overall survival,1 highlighting the need for better tools to identify patients at the highest risk of progression.
Plasma samples were analyzed using the AR ctDETECT assay. Cell-free DNA isolated from 1–3 mL of plasma underwent a customized bioinformatics pipeline designed to identify:
- ctDNA burden (aneuploidy fraction)
- Copy number alterations across 74 target genes
- Pathogenic single-nucleotide variants
- AR structural rearrangements
These genomic features were integrated with established clinical variables to develop a machine learning-based clinical-genetic model for rPFS.
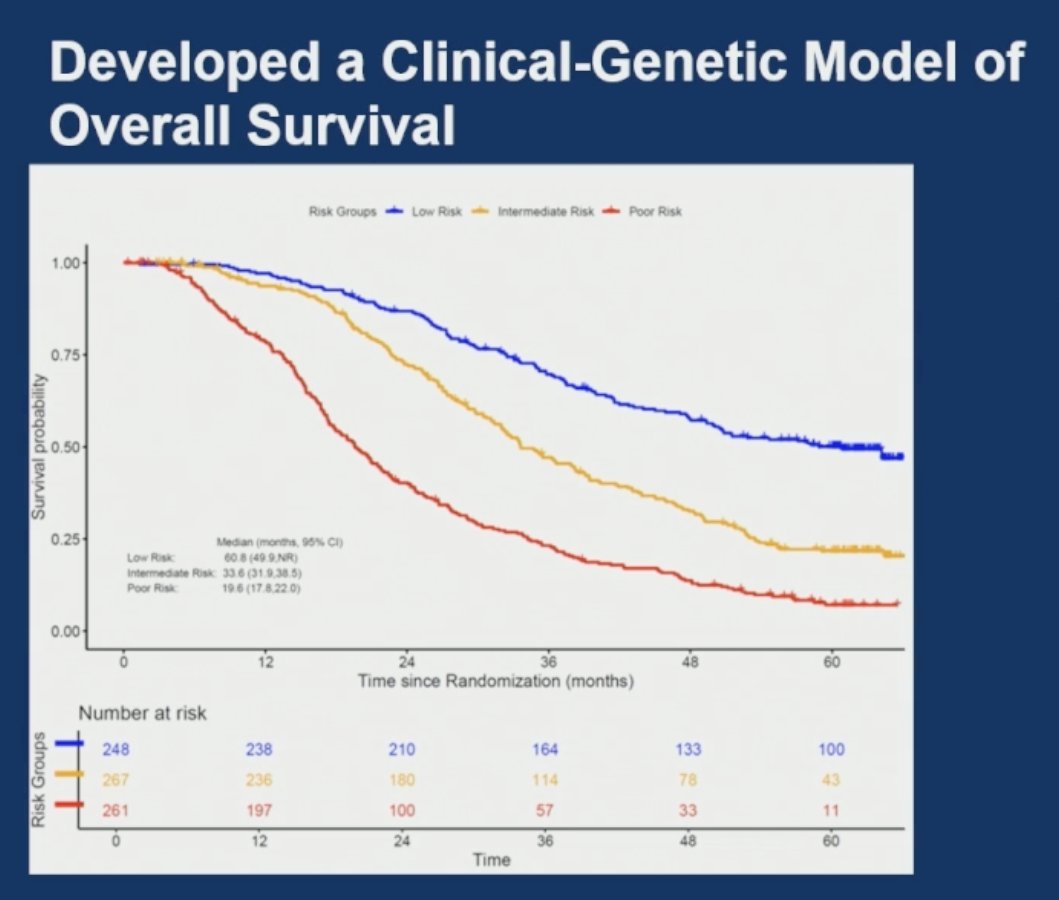
The investigators first demonstrated the prognostic value of ctDNA profiling. Using ctDNA-derived genomic information, they previously developed a clinical-genetic model of overall survival capable of stratifying patients into low-, intermediate-, and poor-risk groups with markedly different outcomes. This work served as the foundation for the development of the current rPFS-specific model.
Notably, the genomic determinants of rPFS differed from those previously identified for overall survival, emphasizing that progression and survival are biologically distinct clinical endpoints.
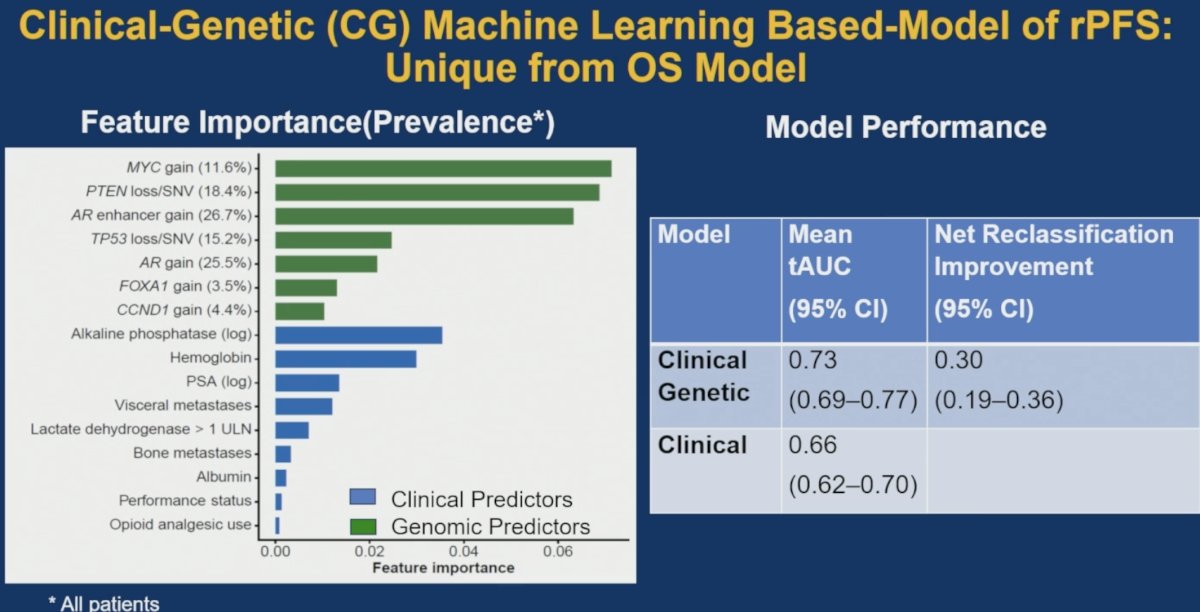
The final machine learning-based clinical-genetic model incorporated both clinical and genomic variables. Among the most influential genomic predictors were:
- MYC gain (11.6%)
- PTEN loss or pathogenic variants (18.4%)
- AR enhancer gain (26.7%)
- TP53 loss or pathogenic variants (15.2%)
- AR gain (25.5%)
- FOXA1 gain (3.5%)
- CCND1 gain (4.4%)
Important clinical contributors included:
- Alkaline phosphatase
- Hemoglobin
- PSA
- Presence of visceral metastases
- Elevated lactate dehydrogenase
- Bone metastases
- Albumin
- Performance status
- Opioid analgesic use
The addition of ctDNA-derived genomic information significantly improved predictive performance compared with a clinical-only model. The clinical-genetic model achieved a mean time-dependent area under the curve (tAUC) of 0.73 (95% CI: 0.69–0.77), compared with 0.66 (95% CI: 0.62–0.70) for the clinical model alone. Furthermore, incorporation of genomic information resulted in a net reclassification improvement of 30% (95% CI: 19–36%).
The model successfully stratified patients into distinct prognostic groups with markedly different rPFS outcomes.
Using a two-group classification system:
- Low-risk patients (n=396) had a median rPFS of 35.2 months (95% CI: 30.5–40.0)
- Poor-risk patients (n=380) had a median rPFS of 14.8 months (95% CI: 13.7–17.0)
Using a three-group classification system:
- Low-risk patients (n=253): median rPFS 40.0 months (95% CI: 34.3–53.5)
- Intermediate-risk patients (n=261): median rPFS 25.2 months (95% CI: 22.3–28.4)
- Poor-risk patients (n=263): median rPFS 12.8 months (95% CI: 11.2–14.6)
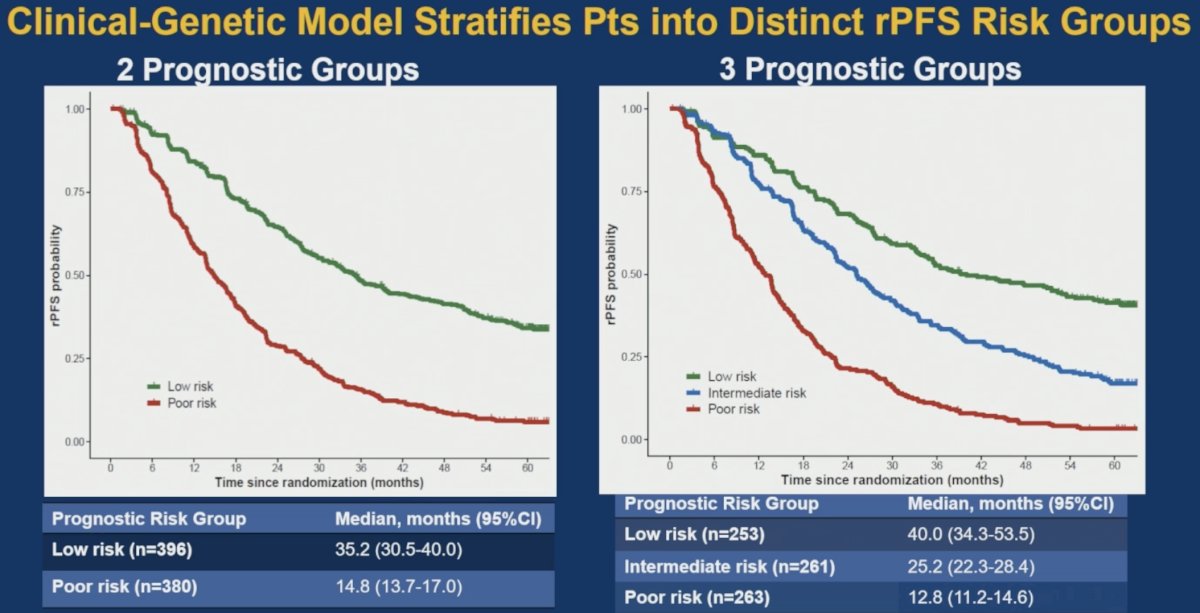
These findings demonstrate substantial separation between prognostic groups and suggest that integration of ctDNA profiling meaningfully refines risk assessment beyond standard clinical variables alone.
Dr. Halabi concluded her presentation as follows:
- Using data from the Alliance A031201 trial, Dr. Halabi and colleagues developed and validated a clinical and ctDNA-based genetic prognostic model of rPFS in the 1st line mCRPC setting with ARPI (enzalutamide ± abiraterone)
- ctDNA profiling added to the clinical model with a statistically significantly higher predictive accuracy than the clinical-only model and a 30% net improvement in correct risk classification
- Key clinical and genetic drivers of rPFS in the new clinical-genetic model include:
- Alk phos, hemoglobin, PSA, pattern of spread, and LDH
- Gains in AR and the AR enhancer, MYC, FOXA1, and CCND1
- Losses or pathogenic mutations of PTEN and TP53
Presented by: Susan Halabi, PhD, Chief of the Division of Biostatistics and Bioinformatics, Duke Cancer Institute, Durham, North Carolina, United States
Written by: Rashid K. Sayyid, MD, MSc, Assistant Professor, Urologic Oncologist, Department of Urology at The University of Arizona and Banner University Medical Center, Tucson, AZ – @rksayyid on X during the American Society of Clinical Oncology Genitourinary (ASCO) Annual Meeting held in Chicago, IL between May 29th and June 1st, 2026
Reference: