(UroToday.com) The 2026 ASCO annual meeting featured a prostate cancer session and a presentation by Dr. Georges Gebrael discussing results from Rad2Nivo, a phase Ib study of radium-223 with nivolumab in patients with metastatic castration resistant prostate cancer (mCRPC). Radium-223 is an α-emitting calcium-mimetic radiopharmaceutical that is FDA approved for patients with mCRPC with symptomatic bone metastasis and no visceral metastasis.1
Preclinical data suggest that radiation might enhance the anticancer effect from PD-1 therapy.2-3 Few patients experience PSA reduction with radium-223, and objective responses in bone metastasis cannot be assessed. Thus, Dr. Gebrael and colleagues hypothesized that radium-223 + nivolumab would be safe and result in decreased ctDNA variant allele frequency as a marker of clinical efficacy.
In this phase IB, prospective, open-label, single-center, single-arm study, patients with symptomatic bone metastatic mCRPC without visceral metastasis were eligible. Participants received intravenous radium-223 (55 kBq/kg IV) monotherapy for 6 cycles. Nivolumab (480 mg IV) was introduced starting with cycle 3 and continued for up to 2 years:
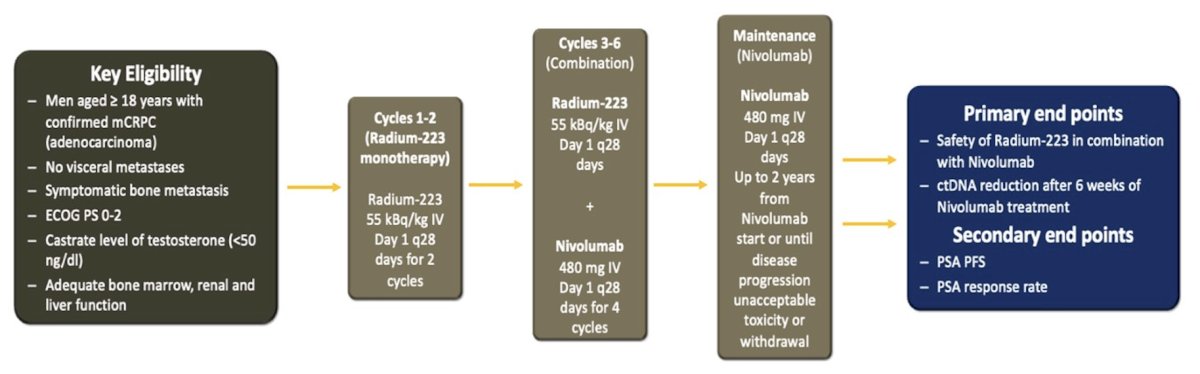
ctDNA was collected at baseline, cycle 3, and 6 weeks after. The primary endpoints were (i) frequency of grade ≥3 non-hematologic treatment-emergent adverse events and (ii) change in ctDNA variant allele frequency from baseline compared to after 6 weeks of nivolumab therapy. Mean variant allele frequency was defined as the average variant allele frequency of all somatic mutations present at baseline at a variant allele frequency 1%. The null hypothesis was that the proportion of patients with a non-zero ctDNA reduction is ≤ 20%. A one-sided exact binomial test was used to evaluate whether the proportion of patients demonstrating a decrease in mean variant allele frequency on-treatment exceeded 20%. With 36 patients, there will be 83% power at one-sided α = 0.05 to detect an alternative proportion of subjects with ctDNA reduction = 40%.
Overall, 39 patients were enrolled in the trial between September 2020 and January 2025, and 35 patients were treated with both radium-223 + nivolumab (4 patients did not receive nivolumab due to clinical progression prior to cycle 3). The median age was 71 years (range: 54-84), the median PSA at study entry was 13.9 ng/dL (range: 0-3245), and 30 patients (77%) had a Gleason score ≥8 (unavailable for 3 patients). The median number of prior lines of therapy was 3 (range: 1-7), and 53.9% (n = 21) of patients had received prior chemotherapy:
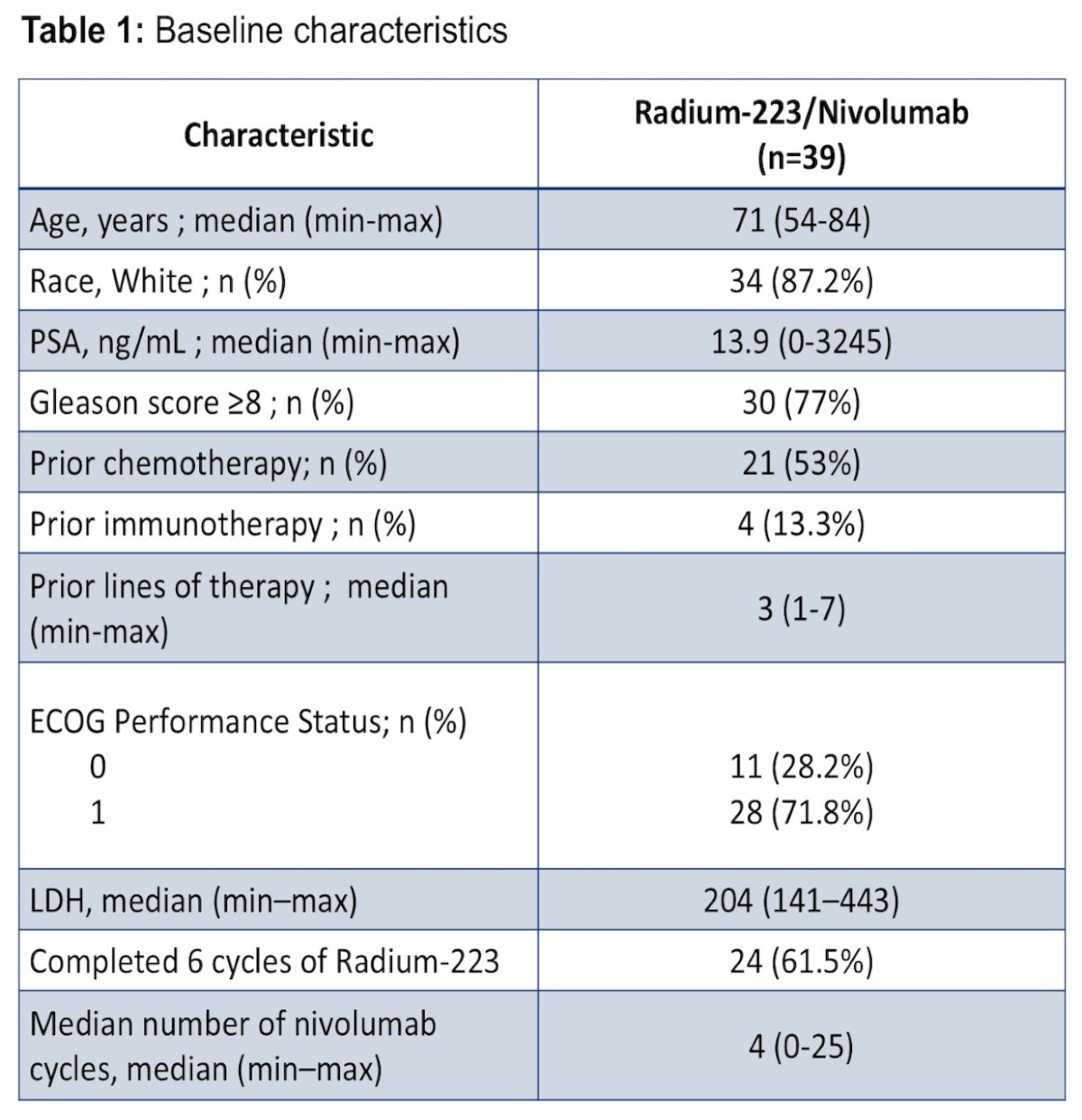
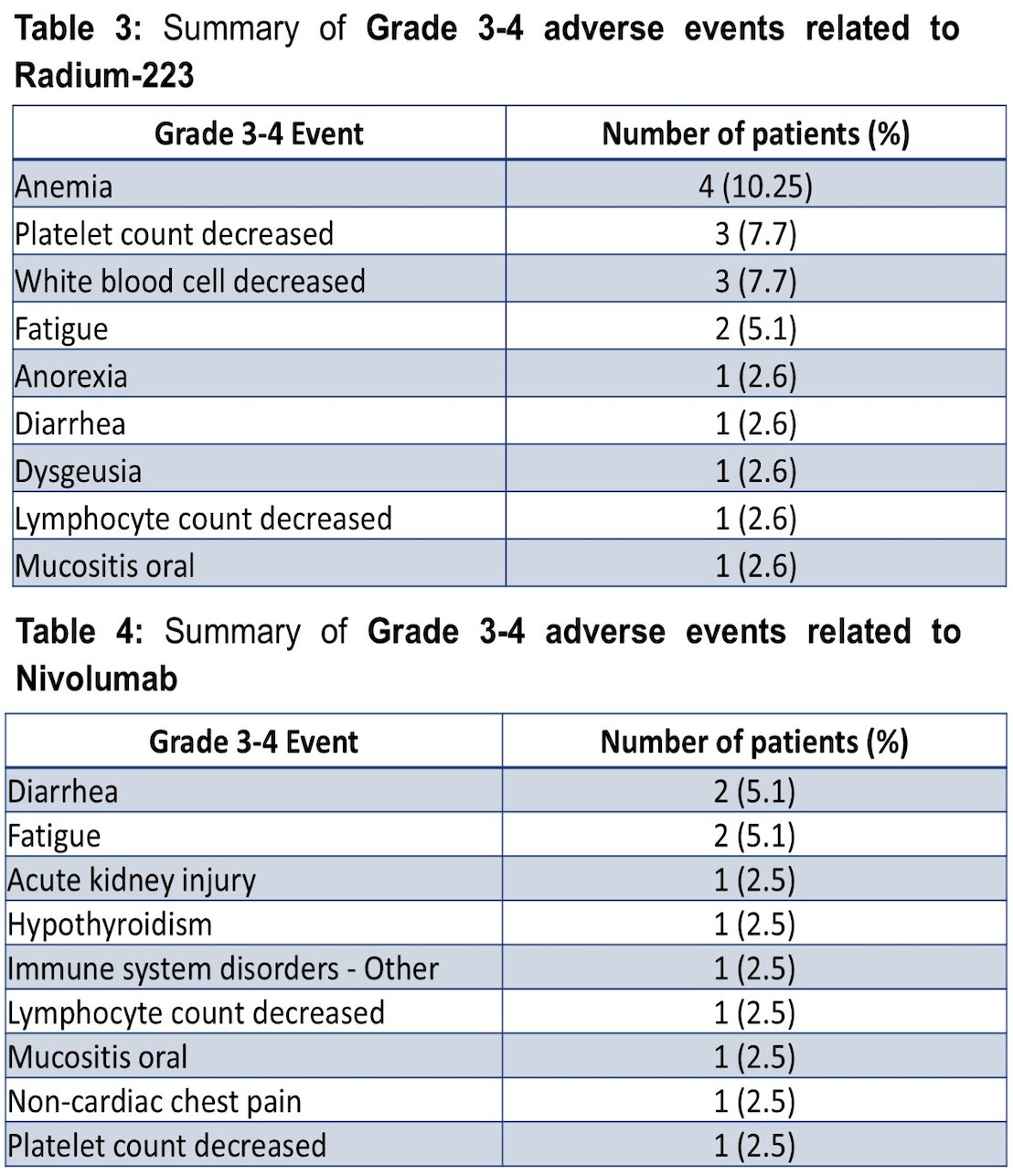
Overall, 61% (n = 24) of patients completed 6 doses of radium-223 (range: 2-6), and the median number of nivolumab cycles was 4 (range: 0-25). Dose holds or delays occurred in 26% (n = 10) and 31% (n = 12) of patients receiving radium-223 and nivolumab, respectively. There were 38% (n = 15) of patients who experienced at least one grade 3-5 treatment-emergent adverse event regardless of attribution. There were no dose-limiting toxicities observed. Serious adverse events related to radium-223 and nivolumab occurred in 5% (n = 2) and 2.6% (n = 1) of patients, respectively. A summary of grade 3-4 adverse events related to radium-223 and to nivolumab is noted in the following tables:
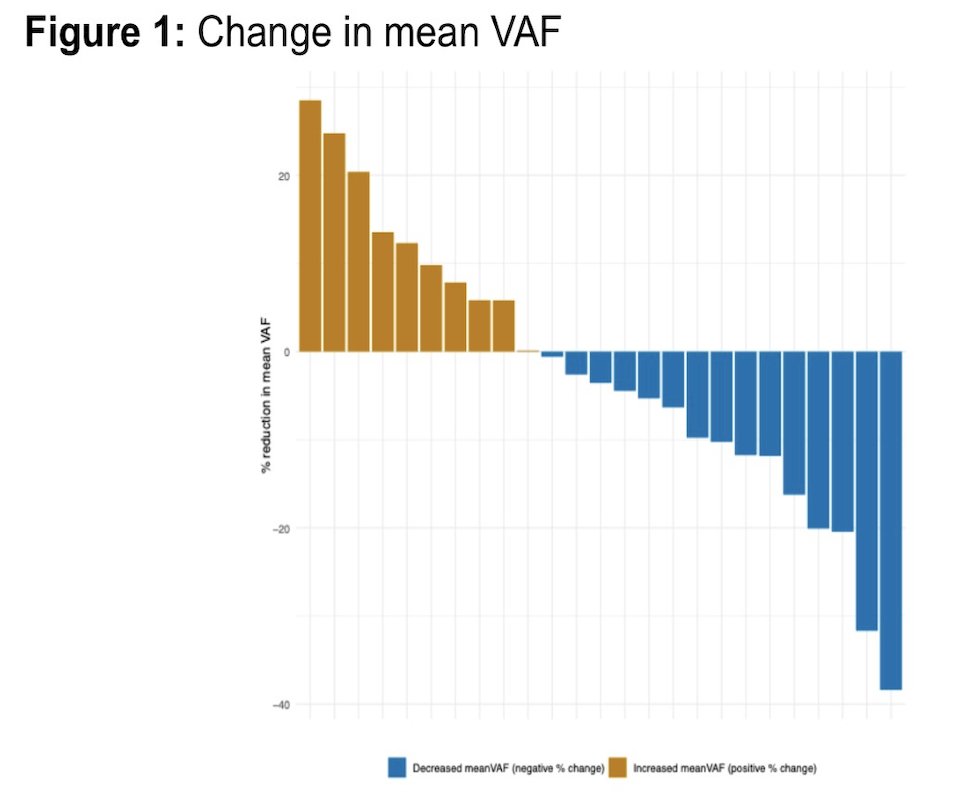
Paired molecular data were available for 25 patients. Variant allele frequency was measurable in all patients who had samples collected and reduction was observed in 15 of 25 patients (60%, one-sided 95% CI, 41.7%-100%; p < 0.01):
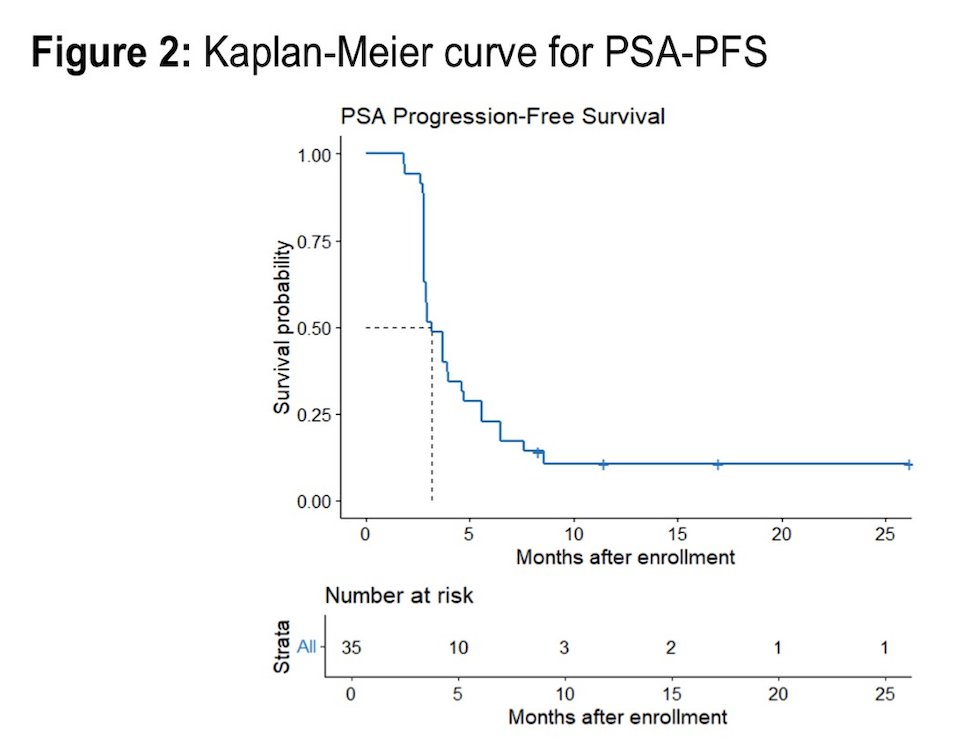
The median PSA progression-free survival was 3.15 months (95% CI 2.79-4.70):
Dr. Gebrael concluded his presentation discussing results from Rad2Nivo, a phase Ib study of radium-223 with nivolumab in patients with mCRPC, with the following take-home points:
- This investigator-initiated trial met its primary endpoints
- The combination of radium-223 and nivolumab appears to be safe, with a toxicity profile consistent with the known adverse effects of each agent and no new safety signals identified
- The mean variant allele frequency was decreased in 60% of the evaluable patients
Presented by: Georges Gebrael, MD, Huntsman Cancer Institute, University of Utah, Salt Lake City, UT
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Associate Professor of Urology, Georgia Cancer Center, Wellstar MCG Health, @zklaassen_md on Twitter during the American Society of Clinical Oncology Genitourinary (ASCO) Annual Meeting held in Chicago, IL between May 29th and June 1st, 2026
References:
- Parker C, Nilsson S, Heinrich D, et al. Alpha emitter radium-223 and survival in metastatic prostate cancer. N Engl J Med 2013;369(3):213-223.
- Dovedi SJ, Adlard AL, Lipowska-Bhalla G, et al. Acquired resistance to fractionated radiotherapy can be overcome by concurrent PD-L1 blockade. Cancer Res. 2014 Oct 1;74(19):5458-5468.
- Kim JW, Shin MS, Kang Y, et al. Immune analysis of radium-223 in patients with metastatic prostate cancer. Clin Genitourin Cancer. 2018 Apr;16(2):e469-e476.