(UroToday.com) The 2026 ASCO annual meeting featured a plenary session and a discussant presentation by Dr. Declan Murphy discussing “Perioperative (neoadjuvant and adjuvant) apalutamide + ADT versus placebo + ADT with radical prostatectomy in high-risk localized or locally advanced prostate cancer: Final analysis of the PROTEUS Phase 3 study” by Dr. Mary-Ellen Taplin.
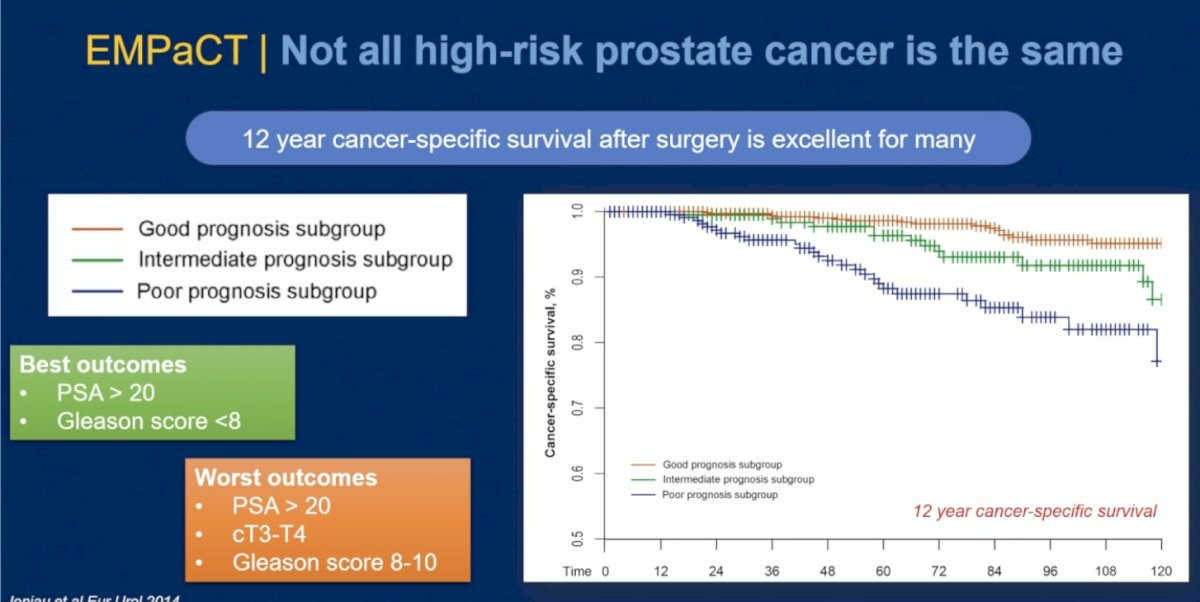
Dr. Murphy began his presentation by emphasizing that not all high-risk prostate cancer behaves the same biologically or clinically. He highlighted long-term data from the EMPaCT study demonstrating that 12-year cancer-specific survival after surgery remains excellent for many patients, underscoring that radical prostatectomy can provide durable disease control in appropriately selected individuals.1
At the same time, he noted the marked heterogeneity within high-risk localized disease. Patients with PSA >20 ng/mL but Gleason score <8 demonstrated more favorable outcomes, whereas those with PSA >20 ng/mL, clinical stage T3–T4 disease, and Gleason score 8–10 experienced the poorest oncologic outcomes. Dr. Murphy stressed that this biologic variability reinforces the need for improved risk stratification and treatment intensification strategies tailored to individual patient risk profiles.1
The first point Dr. Murphy raised when analyzing PROTEUS was that the control arm was not truly reflective of the contemporary standard of care. He emphasized that ADT alone is not currently recommended as standard perioperative therapy for high-risk localized prostate cancer, although he acknowledged the challenges investigators faced when the study was designed. In particular, he noted that this was a large global study conducted across many countries, and maintaining blinding, regulatory alignment, and trial feasibility in the neoadjuvant setting likely influenced the selection of the placebo plus ADT control arm. Dr. Murphy also highlighted the importance of the ongoing PROTEUS substudy directly comparing the PROTEUS regimen against radical prostatectomy alone without ADT, which may ultimately provide additional clarity regarding the true incremental benefit of perioperative systemic intensification.

Dr. Murphy specifically addressed the criticism surrounding the ADT-containing control arm in PROTEUS. He emphasized that although ADT is not standard-of-care perioperative therapy, he does not believe its inclusion invalidates the study results because ADT alone has not been shown to worsen long-term oncologic outcomes. He noted that while ADT does not improve metastasis-free survival or overall survival, it can improve pathologic features such as surgical margins and nodal status.
He summarized this concept succinctly by stating that ADT is “not SOC, but it doesn’t make things worse,” adding that some pathology parameters may actually improve with ADT exposure. Therefore, in his view, the PROTEUS experimental arm can still reasonably be compared against current standards of care while awaiting results from the substudy directly comparing radical prostatectomy alone versus the intensified perioperative PROTEUS regimen.
Dr. Murphy next highlighted the fascinating pathologic opportunities emerging from PROTEUS, particularly surrounding pCR, MRD, and residual cancer burden assessments. He emphasized that the nearly 9-fold improvement in pCR/MRD observed with apalutamide plus ADT represents a highly meaningful biologic signal; however, he cautioned that systemic therapy alone is not sufficient in high-risk localized prostate cancer and stressed that local control continues to matter significantly in this disease setting.

He further noted that the MRD findings were strongly corroborated by residual cancer burden analyses, with favorable residual cancer burden responses observed in 30.6% of patients receiving apalutamide plus ADT compared with 11.7% in the placebo plus ADT arm (OR 3.36; 95% CI 2.67–4.23; p<0.0001). Dr. Murphy suggested that residual cancer burden may ultimately represent a superior measure of tissue response, given its correlation with metastasis-free survival and its potential role as a future surrogate endpoint in perioperative prostate cancer trials.
Dr. Murphy noted that Dr. Taplin had already clearly demonstrated that MRD findings were corroborated by residual cancer burden analyses, reinforcing the biologic consistency of the PROTEUS results.2 He emphasized that residual cancer burden may ultimately represent a better measure of tissue response than traditional binary pCR endpoints, particularly because increasing residual cancer burden classes appeared to correlate closely with worse metastasis-free survival outcomes over time

Dr. Murphy noted that the PROTEUS pathology findings raise an important clinical question: Does every patient truly require prolonged adjuvant therapy after surgery? He emphasized that the marked improvements in pCR, MRD, and residual cancer burden achieved with perioperative apalutamide plus ADT suggest that pathologic response may eventually help guide treatment personalization and de-escalation strategies in selected patients.
At the same time, he reiterated that local control remains paramount in high-risk localized prostate cancer. In his view, the PROTEUS data demonstrate that intensified systemic therapy with ADT plus apalutamide meaningfully improves pCR, MRD, and residual cancer burden outcomes, and that these pathologic improvements ultimately translate into better metastasis-free survival.
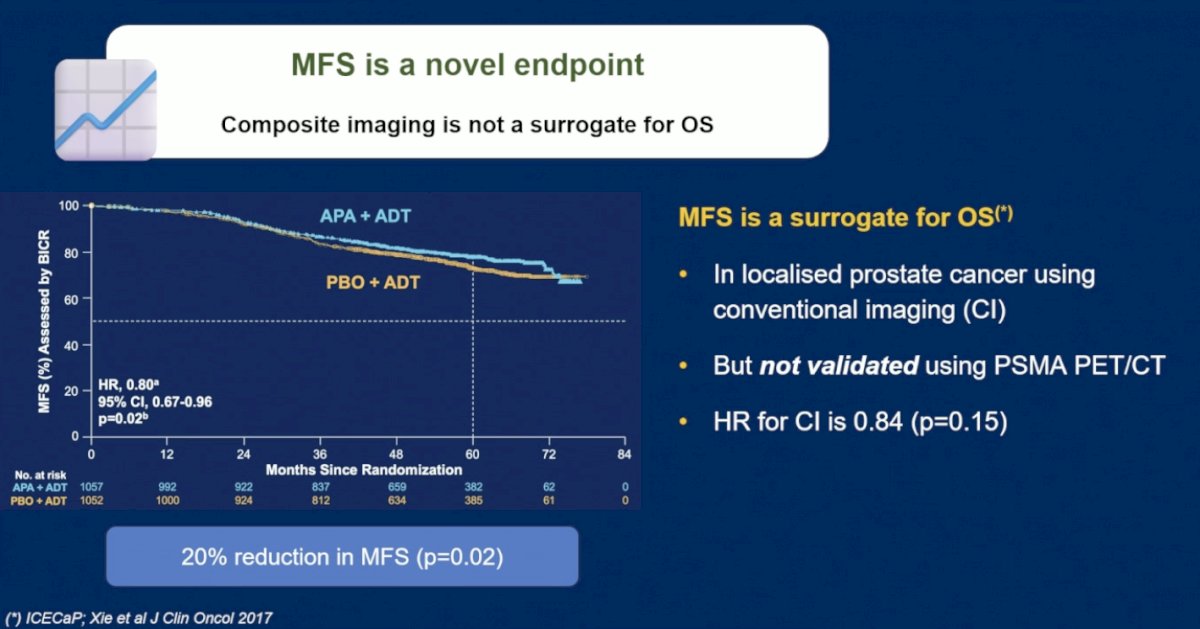
The third point Dr. Murphy raised focused on the interpretation of metastasis-free survival in the PSMA PET era. He emphasized that while metastasis-free survival has been validated as a surrogate for overall survival in localized prostate cancer using conventional imaging, this relationship has not yet been validated when PSMA PET/CT is incorporated into endpoint assessment.
He noted that PROTEUS demonstrated a 20% reduction in the risk of metastasis or death using the composite imaging endpoint; however, the conventional imaging-only analysis was not statistically significant (HR 0.84; p=0.15). Dr. Murphy cautioned that PSMA PET may detect metastatic disease substantially earlier than conventional imaging, potentially altering the interpretation of metastasis-free survival endpoints.
Dr. Murphy acknowledged that the metastasis-free survival benefit observed in PROTEUS is clinically meaningful, emphasizing that metastases unquestionably matter in high-risk prostate cancer because they ultimately impact long-term patient outcomes and subsequent treatment burden. However, he reiterated that metastasis-free survival defined using PSMA PET imaging should not yet be considered a validated surrogate for overall survival. He further stressed that PSMA PET/CT is now standard of care for staging and restaging high-risk localized prostate cancer, making its incorporation into modern trials appropriate and clinically relevant.
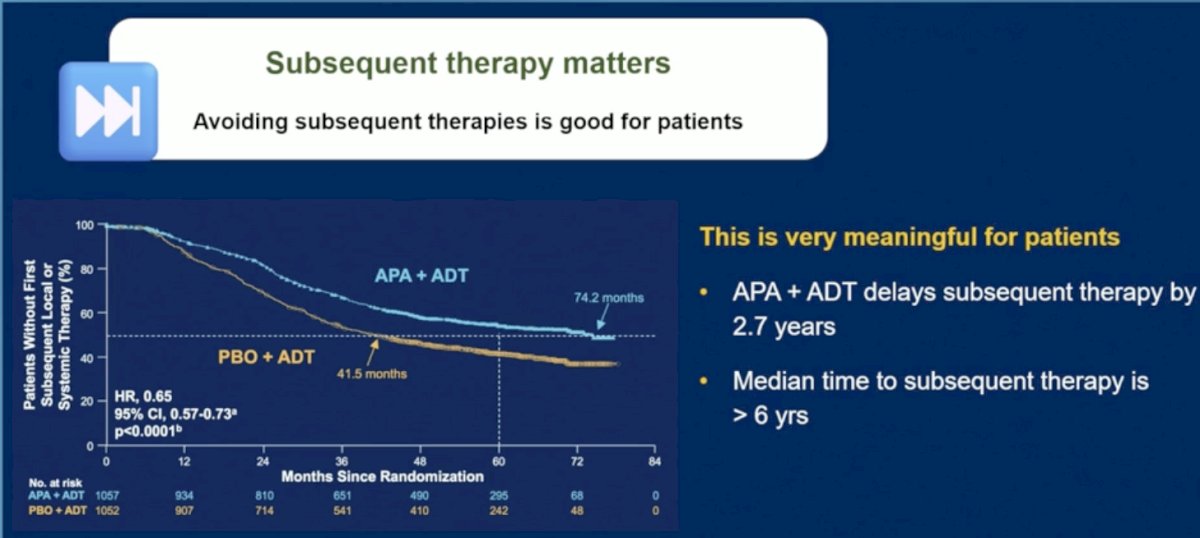
The fourth endpoint Dr. Murphy discussed was time to subsequent therapy, which he considered highly meaningful from a patient perspective. He emphasized that avoiding or substantially delaying additional therapy is critically important in high-risk localized prostate cancer, particularly given that these patients may otherwise face years of additional treatment burden, toxicity, and quality-of-life implications.
He highlighted that perioperative apalutamide plus ADT delayed the need for subsequent therapy by approximately 2.7 years, with median time to subsequent therapy extending beyond 6 years. Dr. Murphy stressed that for patients who may live another 10–15 years after diagnosis, delaying or potentially avoiding subsequent local or systemic therapies represents a clinically and personally meaningful outcome, and the quality of the patient journey should be considered.
Furthermore, Dr. Murphy highlighted the work of Dr. Christopher Sweeney, who previously helped validate metastasis-free survival as a surrogate endpoint for overall survival in localized prostate cancer. He noted that Dr. Sweeney has now proposed a new composite endpoint termed “Freedom from Clinical Detriment” (FFCD), which is currently being discussed with regulatory agencies, including the FDA. Dr. Murphy explained that FFCD is intended to serve as a more patient-centered endpoint, capturing not only PSA relapse and metastatic progression, but also the broader clinical consequences patients experience, including anxiety, additional scans, subsequent therapies, and sustained deterioration in quality of life.
The underlying hypothesis is that intensification of primary therapy in high-risk localized prostate cancer may ultimately be justified not solely by traditional oncologic endpoints, but also by reducing clinically meaningful detrimental events associated with disease recurrence.
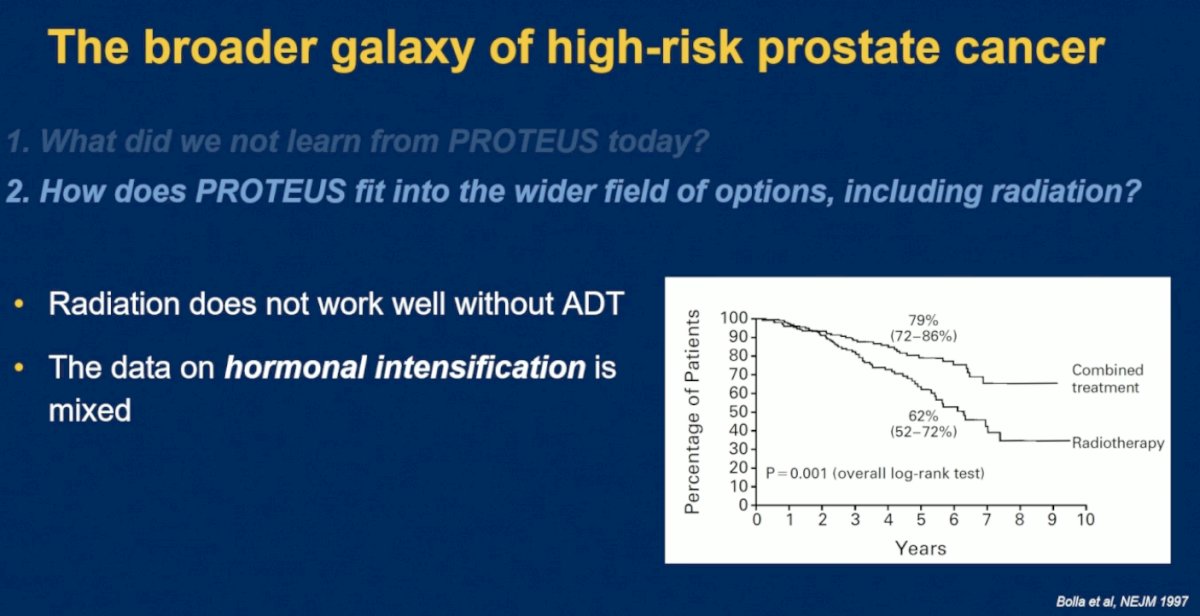
Dr. Murphy continued by placing PROTEUS within the broader landscape of high-risk localized prostate cancer management and emphasizing several important unanswered questions that remain following this landmark trial. He noted that although PROTEUS demonstrated compelling improvements in pCR/MRD, metastasis-free survival, event-free survival, and time to subsequent therapy, mature cancer-specific survival and overall survival data are still awaited. He also emphasized the importance of understanding which patient subgroups derive the greatest benefit from perioperative intensification, as well as identifying patients who may potentially avoid overtreatment.
In addition, Dr. Murphy highlighted the need for more detailed analyses regarding patient-reported outcomes, quality of life, and surgical outcomes following intensified perioperative systemic therapy. Finally, he stated that further characterization of adverse events and long-term tolerability will be essential as the field determines how PROTEUS should ultimately integrate into the wider treatment landscape for high-risk prostate cancer, including alongside radiation-based treatment strategies.
Radiation therapy historically has not performed optimally without ADT intensification, highlighting prior data demonstrating improved outcomes with combined treatment strategies compared with radiation alone.3 However, he emphasized that the data surrounding additional hormonal intensification beyond conventional ADT remain somewhat mixed across radiation-based studies. In this context, Dr. Murphy suggested that PROTEUS provides compelling evidence supporting intensified perioperative systemic therapy in surgically managed patients with high-risk disease.
Dr. Murphy noted that radiation oncologists have already been exploring treatment intensification strategies in high-risk localized prostate cancer through landmark trials such as STAMPEDE and ENZARAD.4,5 He highlighted that the STAMPEDE radiation cohort evaluated the addition of abiraterone to ADT and radiation therapy in a particularly high-risk population, with a median PSA of 35 ng/mL, 92% of patients harboring clinical T3–T4 disease, and 39% presenting with cN1 disease. In that study, treatment intensification significantly improved metastasis-free survival (HR 0.53; p<0.0001). In contrast, ENZARAD, which evaluated enzalutamide intensification alongside radiation and ADT, did not demonstrate a significant metastasis-free survival benefit in the overall study population (HR 0.88; p=0.34), although subgroup outcomes among cN1 patients appeared more favorable.
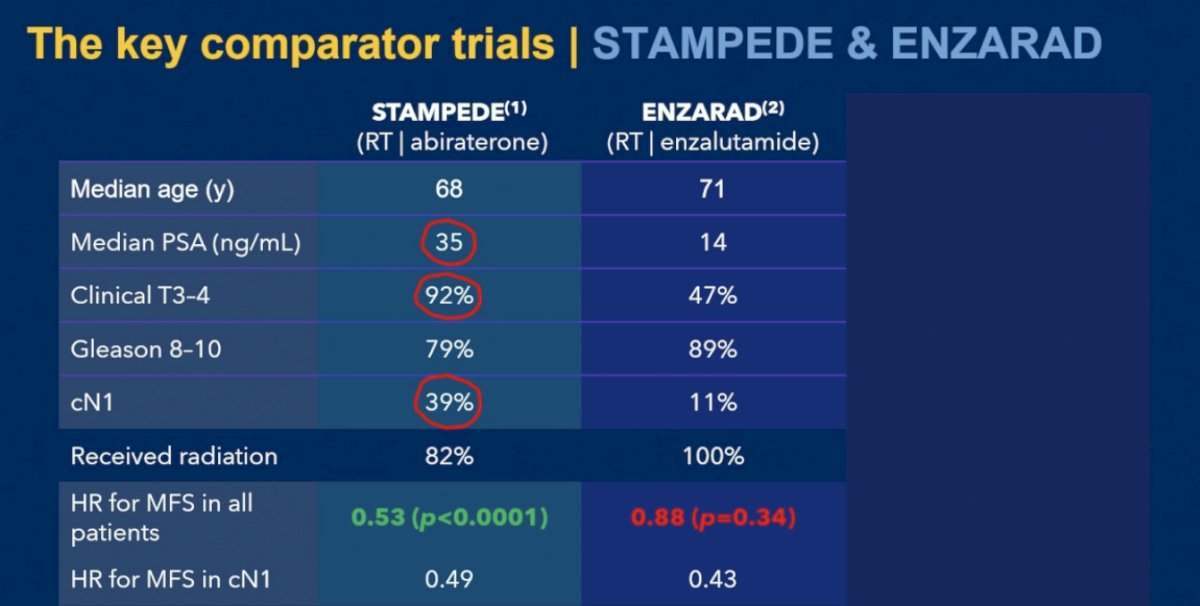
Dr. Murphy then directly compared PROTEUS with ENZARAD, highlighting the intriguing differences between these two intensification strategies despite seemingly similar patient populations. He noted that ENZARAD and PROTEUS enrolled patients with relatively comparable baseline characteristics, including similar median PSA levels (14 ng/mL), high proportions of Gleason 8–10 disease (89% vs 95%), and nodal involvement rates (11% vs 12%). However, while ENZARAD failed to demonstrate a metastasis-free survival benefit (HR 0.88; p=0.34), PROTEUS met its metastasis-free survival endpoint with a significant benefit favoring perioperative apalutamide intensification (HR 0.80; p=0.02).
Dr. Murphy emphasized that this raises several important biological and clinical questions for the field. He questioned whether the difference may relate to the specific ARPI utilized, although both are very good ARPIs, whether incorporation of composite imaging endpoints, including PSMA PET could have altered ENZARAD outcomes, or whether surgery itself may fundamentally contribute differently to disease control compared with radiation-based strategies and is potentially better in this setting. He also noted that despite the use of a composite metastasis-free survival endpoint in PROTEUS, the trial remained a large, rigorously conducted randomized study with clinically meaningful findings.

Lastly, Dr. Murphy proposed a new treatment algorithm for patients with high-risk localized prostate cancer, integrating the emerging PROTEUS data into the broader multidisciplinary management landscape. He emphasized that treatment decisions should increasingly account for disease heterogeneity, biologic risk, imaging findings, patient comorbidities, and anticipated quality-of-life implications.
He suggested that perioperative treatment intensification with apalutamide plus ADT followed by radical prostatectomy may now represent an important option for appropriately selected patients with very high-risk disease, particularly those with aggressive pathologic or imaging characteristics. At the same time, he stressed that radiation-based intensification strategies remain highly relevant, underscoring the importance of individualized multidisciplinary decision-making rather than a “one-size-fits-all” approach.

Dr. Murphy concluded his discussant presentation with the following take home points:
- PROTEUS is a landmark surgical trial in high-risk localized prostate cancer and establishes a new benchmark for perioperative systemic intensification
- The positive metastasis-free survival, pathologic response, and treatment-free interval endpoints represent clinically meaningful gains for appropriately selected patients
- Delaying subsequent therapy is an important patient-focused endpoint that may translate into years of reduced treatment burden and fewer downstream interventions for many men
- Perioperative ADT plus apalutamide is likely to become a new standard of care for men with the highest-risk prostate cancer undergoing radical prostatectomy
Presented by: Declan Murphy, MB, BCh, BaO, FRACS, FRCS Urol, Peter MacCallum Cancer Centre, Melbourne, Australia
Written by: Julian Chavarriaga, MD, Clinical Assistant Professor, Urologic Oncologist, Department of Urology at Penn State Health @chavarriagaj on X during the American Society of Clinical Oncology Genitourinary (ASCO) Annual Meeting held in Chicago, IL between May 29th and June 1st, 2026
Related content: PROTEUS Trial: Neoadjuvant Apalutamide and Androgen Deprivation Therapy in High-Risk Localized Prostate Cancer - Mary-Ellen Taplin
References:
- Joniau S, Briganti A, Gontero P, Gandaglia G, Tosco L, Fieuws S, Tombal B, Marchioro G, Walz J, Kneitz B, Bader P, Frohneberg D, Tizzani A, Graefen M, van Cangh P, Karnes RJ, Montorsi F, Van Poppel H, Spahn M; European Multicenter Prostate Cancer Clinical and Translational Research Group (EMPaCT). Stratification of high-risk prostate cancer into prognostic categories: a European multi-institutional study. Eur Urol. 2015 Jan;67(1):157-164. doi: 10.1016/j.eururo.2014.01.020. Epub 2014 Jan 25. PMID: 24486307.
- Ravi P, Kwak L, Acosta AM, Rastogi S, Xie W, Abdelnaser A, Einstein DJ, Chang P, Wagner AA, McKay RR, Kibel AS, Taplin ME. Long-term Outcomes and Prognostic Impact of Residual Cancer Burden After Intensified Neoadjuvant Therapy in High-risk Prostate Cancer. Eur Urol. 2025 Jun;87(6):643-650. doi: 10.1016/j.eururo.2025.01.015. Epub 2025 Feb 7. PMID: 39920004.
- Bolla M, Gonzalez D, Warde P, Dubois JB, Mirimanoff RO, Storme G, Bernier J, Kuten A, Sternberg C, Gil T, Collette L, Pierart M. Improved survival in patients with locally advanced prostate cancer treated with radiotherapy and goserelin. N Engl J Med. 1997 Jul 31;337(5):295-300. doi: 10.1056/NEJM199707313370502. PMID: 9233866.
- Attard G, Murphy L, Clarke NW, et al. Abiraterone acetate and prednisolone with or without enzalutamide for high-risk non-metastatic prostate cancer: A meta-analysis of primary results from two randomized controlled phase 3 trials of the STAMPEDE platform protocol. Lancet. 2022; 399(10323):447-460.
- https://www.urotoday.com/conference-highlights/esmo-2025/esmo-2025-prostate-cancer/164090-esmo-2025-randomized-phase-iii-trial-of-androgen-deprivation-therapy-adt-with-radiation-therapy-with-or-without-enzalutamide-for-high-risk-clinically-localized-prostate-cancer-enzarad-anzup-1303.html