(UroToday.com) The 2026 ASCO annual meeting featured a prostate cancer session and a presentation by Dr. Fred Saad discussing a post hoc analysis of ARANOTE assessing PSA outcomes of darolutamide and ADT in patient subgroups by age, comorbidities, and concomitant medications. Darolutamide + ADT significantly improved radiological progression free survival (HR 0.54, 95% CI 0.41–0.71; p < 0.0001) versus placebo + ADT in patients with metastatic hormone-sensitive prostate cancer (mHSPC) in the phase 3 ARANOTE trial, with a favorable safety profile.1 In a post hoc analysis, efficacy (radiographic progression free survival, time to mCRPC, and time to PSA progression), quality of life, and safety outcomes with darolutamide + ADT were improved in patients with mHSPC versus placebo + ADT, regardless of age. In another post hoc analysis, a radiographic progression free survival benefit was previously seen across all patient subgroups with mHSPC, regardless of the number of comorbidities and concomitant medications reported at baseline, with no new safety signals. At the ASCO 2026 annual meeting, Dr. Saad reported the impact of age, comorbidities, and use of concomitant medications ongoing at baseline on PSA outcomes in patients treated with darolutamide or placebo.
Patients in ARANOTE were randomized 2:1 to darolutamide 600 mg orally twice daily or placebo, both with ADT:
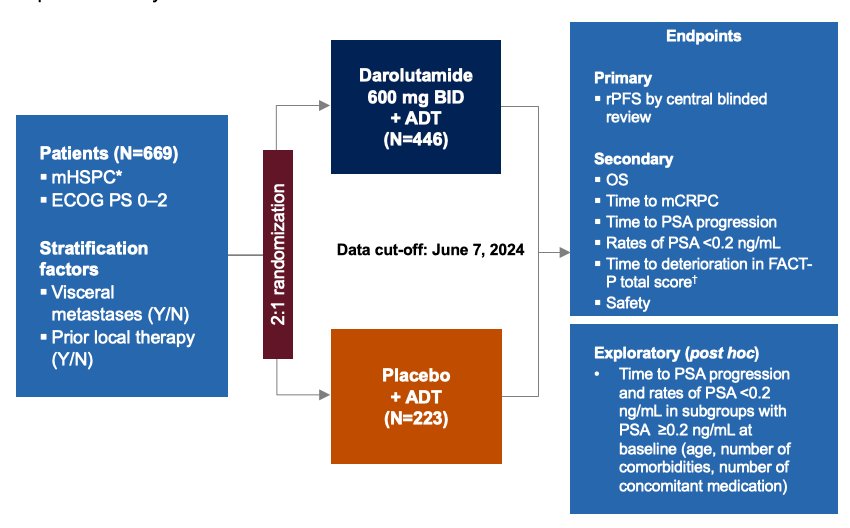
Patients were grouped by age and number/type of comorbidities or concomitant medications reported at baseline. Descriptive statistics (post hoc) summarized baseline demographics, disease characteristics, and PSA outcomes by age, comorbidities, and concomitant medication subgroups.
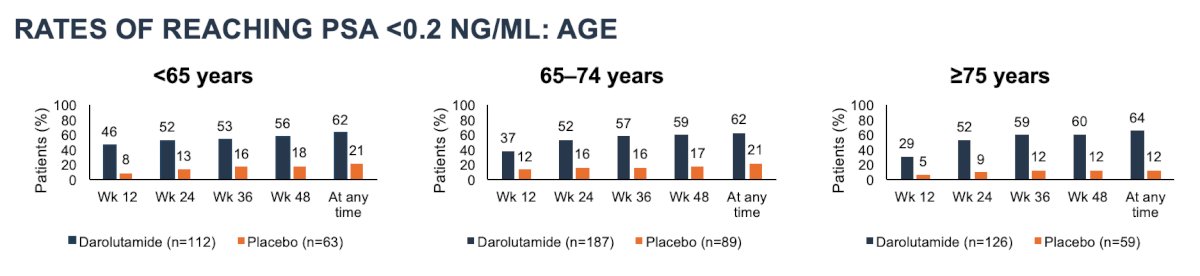
Baseline demographics and disease characteristics were generally similar between darolutamide (n = 446) and placebo (n = 223) across all subgroups by age (<65, 65–74, or ≥75 years), comorbidities (<5 or ≥5), and concomitant medications (<5 or ≥5), respectively. Rates of reaching PSA <0.2 ng/mL at any time were consistently higher with darolutamide versus placebo across all age (<65 years, 62% [n = 69/112] versus 21% [n = 13/63]; 65–74 years, 62% [n = 116/187] versus 21% [n = 19/89]; ≥75 years, 64% [n = 81/126] versus 12% [n = 7/59]):
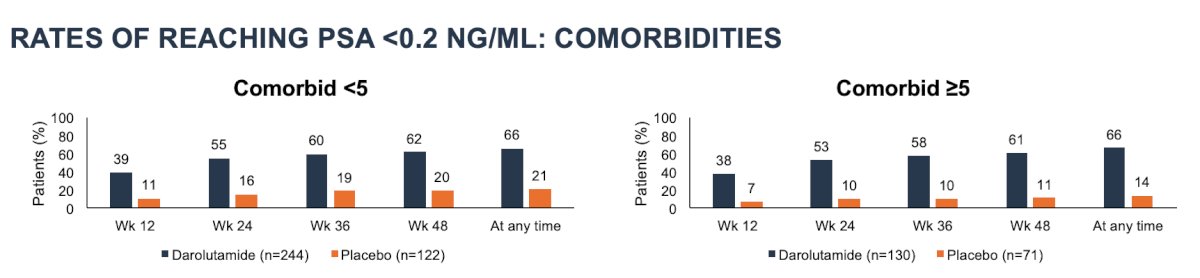
Similar results favoring darolutamide were also seen for comorbidity (<5, 66% [n = 160/244] versus 21% [n = 26/122]; ≥5, 66% [n = 86/130] versus 14% [n = 10/71]) subgroups:
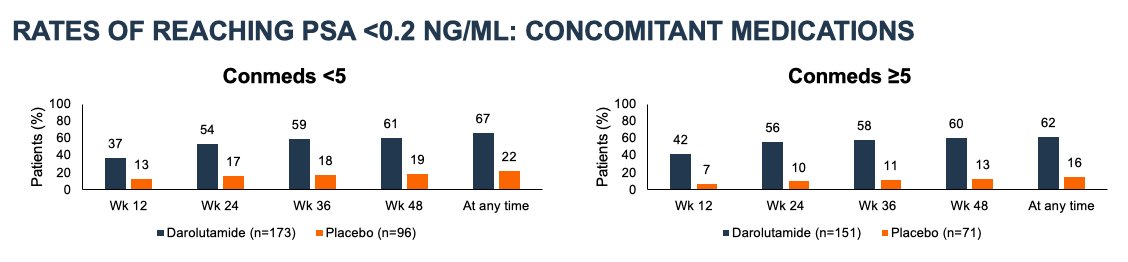
and concomitant medication (<5, 67% [n = 115/173] versus 22% [n = 21/96]; ≥5, 62% [n = 93/151] versus 16% [n = 11/71]) subgroups:
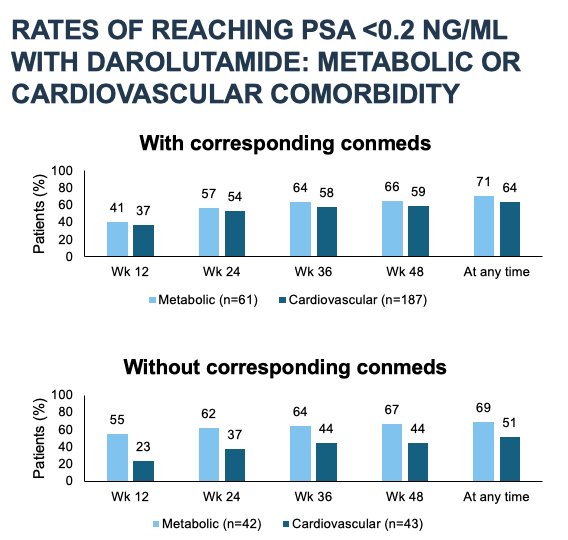
With darolutamide, rates of reaching PSA <0.2 ng/mL at any time were consistent among patients with metabolic disorders with or without corresponding concomitant medications (71% [n = 43/61] versus 69% [n = 29/42]). The rate of reaching PSA <0.2 ng/ml was slightly lower in patients with cardiovascular disorders who were not receiving corresponding concomitant medications at baseline (51% [n = 22/43]) compared with those receiving corresponding concomitant medications (64% [n = 119/187]):
A substantially lower rate of PSA progression was observed with darolutamide (8% [n = 22/266]) versus placebo (33% [n = 13/39]) among patients that reached PSA <0.2 ng/mL. The median time to PSA progression among patients that reached PSA <0.2 ng/mL was 421 days (range, 85–702) and 256 days (range, 85–514) for darolutamide and placebo, respectively.
Dr. Saad concluded his presentation discussing a post hoc analysis of ARANOTE assessing PSA outcomes of darolutamide and ADT in patient subgroups by age, comorbidities, and concomitant medications with the following take home points:
- Overall, an efficacy benefit was observed with darolutamide, irrespective of age, and number of comorbidities or concomitant medications reported at baseline in patients with mHSPC, including those with cardiovascular or metabolic disorders, with or without corresponding concomitant medications, respectively
- These results support the use of darolutamide in mHSPC, even in patients with older age, substantial comorbidities, and greater use of concomitant medications
Presented by: Fred Saad, MD, FRCS, CQ, FCAHS, Centre Hospitalier de l’Universite de Montreal, Montreal, Quebec, Canada
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Associate Professor of Urology, Georgia Cancer Center, Wellstar MCG Health, @zklaassen_md on Twitter during the American Society of Clinical Oncology Genitourinary (ASCO) Annual Meeting held in Chicago, IL between May 29th and June 1st, 2026
References: