(UroToday.com) The 2026 ASCO annual meeting featured a prostate cancer trials in progress session and a presentation by Dr. Donald Vile discussing OMAHA-004, a phase 3 trial of steroidogenesis inhibitor opevesostat versus androgen receptor pathway inhibitor (ARPI) switch in participants with metastatic castration resistant prostate cancer (mCRPC) after a prior ARPI. Activating androgen receptor somatic mutations are a common mechanism of resistance to androgen receptor-directed therapies in mCRPC, and they may permit continued hormonal dependence. Upstream targeting of androgen biosynthesis may provide a therapeutic advantage over available androgen receptor antagonist therapies for mCRPC. Opevesostat (MK-5684; ODM-208) is an oral, nonsteroidal inhibitor of cytochrome P450 11A1 (CYP11A1), a catalyst of the first and rate-limiting step of steroid biosynthesis from cholesterol. Opevesostat previously showed antitumor activity in participants with heavily pretreated mCRPC in the phase 1/2 CYPIDES trial. The randomized, open-label, phase 3 OMAHA-004 trial is designed to evaluate the efficacy and safety of opevesostat in participants with mCRPC after a prior ARPI.
Eligible participants have mCRPC that progressed during ADT ≤6 months before screening and on or after one ARPI for metastatic or nonmetastatic hormone-sensitive prostate cancer (HSPC) or CRPC for ≥8 weeks (≥14 weeks with bone progression). Prior ARPI + docetaxel for HSPC is permitted if participants received no more than 6 cycles of docetaxel without radiographic disease progression. Approximately 1,314 participants will be randomized 1:1 to opevesostat 5 mg orally twice-daily plus dexamethasone 1.5 mg and fludrocortisone 0.1 mg orally once daily or abiraterone acetate 1,000 mg orally once daily plus prednisone 5 mg orally twice daily (if prior enzalutamide, darolutamide, or apalutamide) or enzalutamide 160 mg orally once-daily (if prior abiraterone). Stratification factors are metastatic site (bone only versus liver versus other), androgen receptor ligand binding mutation status (positive versus negative), and prior docetaxel treatment for HSPC (yes versus no):
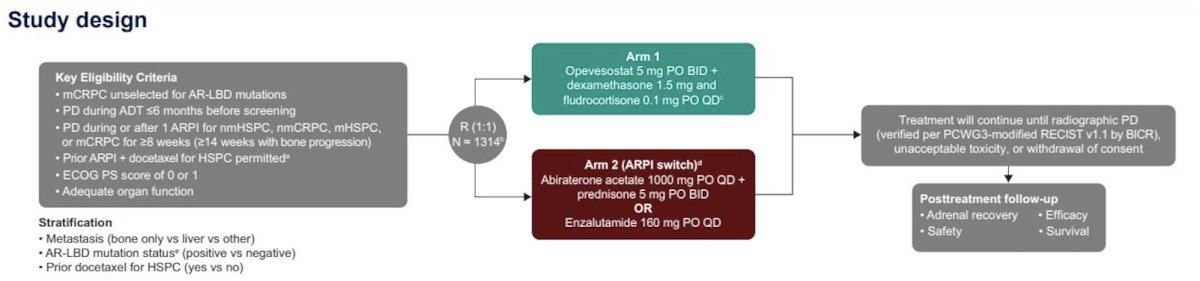
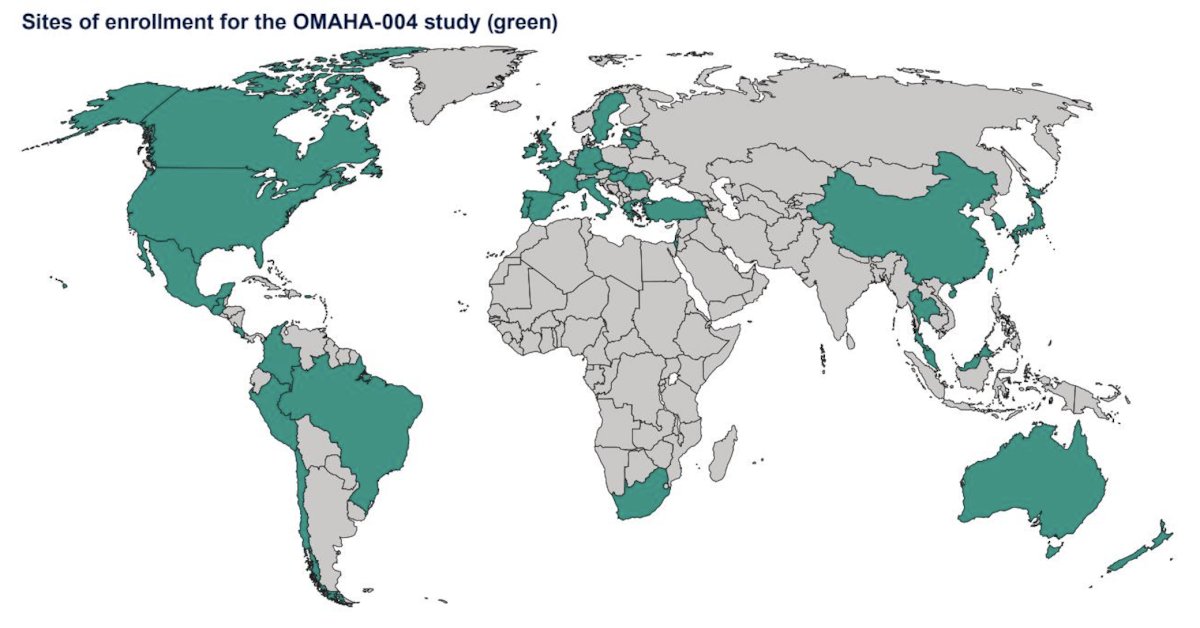
Once the predefined enrollment threshold for participants with either mutation status (androgen receptor ligand binding mutation-positive, ~400 participants, or androgen receptor ligand binding mutation-negative, ~914 participants) is met, no additional participants with that mutation status will be permitted to enroll. The protocol was amended to use radiographic progression free survival per PCWG3-modified RECIST v1.1 by blinded independent central review, analyzed separately in participants with androgen receptor ligand binding mutation-positive and -negative disease, as the primary end point and overall survival as a key secondary end point. Other secondary end points include time to initiation of first subsequent anticancer therapy or death, objective response rate, and duration of response per PCWG3-modified RECIST v1.1 by blinded independent central review, time to pain progression, time to PSA progression, PSA response rate, time to first symptomatic skeletal-related event, and safety and tolerability. Enrollment is ongoing at the following global sites:
Presented by: Donald C. Vile, MD, Blue Ridge Cancer Care, Roanoke, VA
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Associate Professor of Urology, Georgia Cancer Center, Wellstar MCG Health, @zklaassen_md on Twitter during the American Society of Clinical Oncology Genitourinary (ASCO) Annual Meeting held in Chicago, IL between May 29th and June 1st, 2026