(UroToday.com) The 2026 ASCO annual meeting featured a prostate cancer session and a presentation by Dr. Atish Choudhury discussing results from CLEARED, a trial assessing a comeback from a long-course androgen deprivation therapy (ADT) with relugolix and darolutamide in hormone-sensitive prostate cancer. The oral luteinizing hormone-releasing hormone antagonist relugolix and androgen receptor pathway inhibitor (ARPI) darolutamide are approved for the treatment of advanced prostate cancer, but the combination has not been prospectively investigated.
Radiation therapy with 2 years of LHRH agonist or antagonist + ARPI is a common regimen for high-risk localized, node-positive, or oligometastatic prostate cancer. Testosterone recovery is more rapid after 1 year of relugolix compared to leuprolide, but recovery after 2 years of relugolix has not been reported. At the ASCO 2026 annual meeting, Dr. Choudhury and colleagues reported pharmacokinetics as well as initial safety and reduction in testosterone and PSA from a phase 2 trial of relugolix + darolutamide in high-risk localized, lymph node-positive, or low volume metastatic prostate cancer.
Eligible patients had PSA > 0.02 ng/ml, testosterone ≥ lower limit of normal, and were planned for 2 years of ADT + ARPI for high-risk localized, lymph node-positive, or low-volume metastatic prostate cancer. Prior ADT ± ARPI was permitted if testosterone recovered to ≥ the lower limit of normal, but patients with high volume metastatic prostate cancer, prior PSA rise with castrate testosterone, or on medications with significant predicted drug-drug interactions with relugolix or darolutamide were excluded. Patients received relugolix 360 mg ×1 on day 1 (D1) followed by 120 mg QD and darolutamide 600 mg BID starting on D1, and elected for pharmacokinetics sampling at 0h, 2h, 4h, 8h on D1 (cohort 1) or pre-dose on D1, 2, 8, and 29 (cohort 2). Radiation therapy to local and/or metastatic sites was delivered per standard of care. Patients received up to 26 28-day treatment cycles with PSA/testosterone monitoring every 3 months until 18 months after the end of treatment:
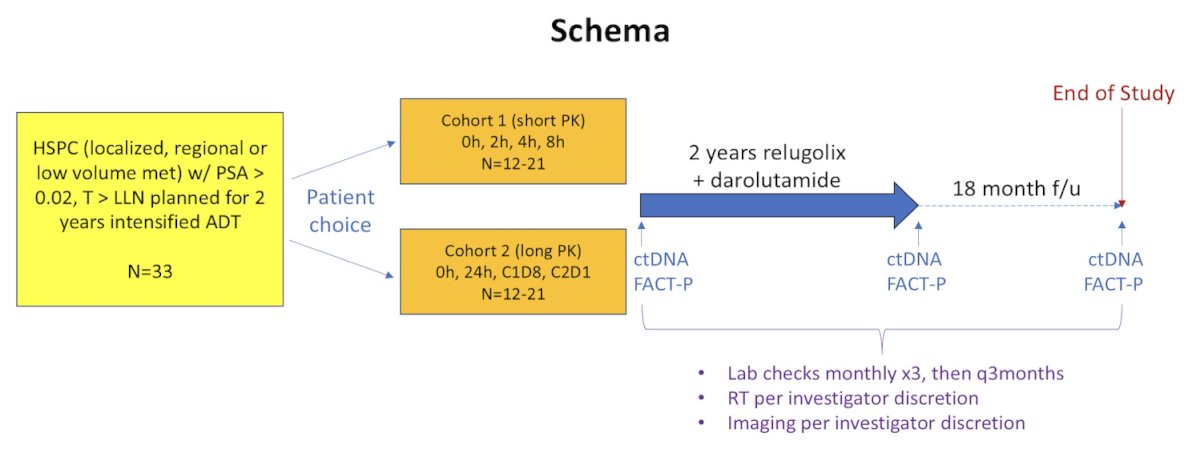
The primary endpoints are the rate of testosterone recovery to > lower limit of normal by 18 months after the end of treatment and safety/adverse events. Secondary endpoints include pharmacokinetics, rate of treatment discontinuation, and patient-reported outcomes.
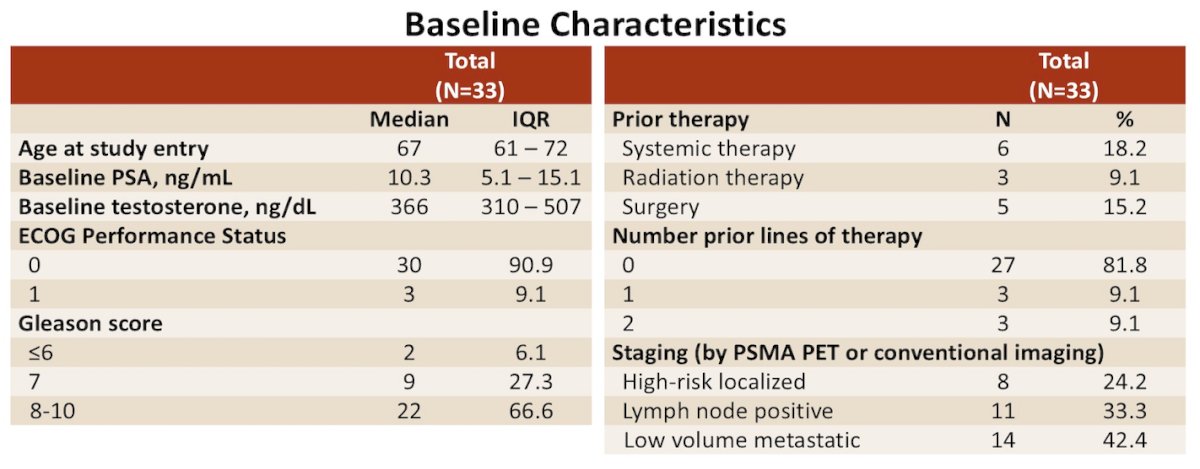
There were 33 patients enrolled: 8 with high-risk localized, 11 with lymph node-positive, and 14 with low-volume metastatic prostate cancer. Overall, 21 patients chose cohort 1, and 12 chose cohort 2:
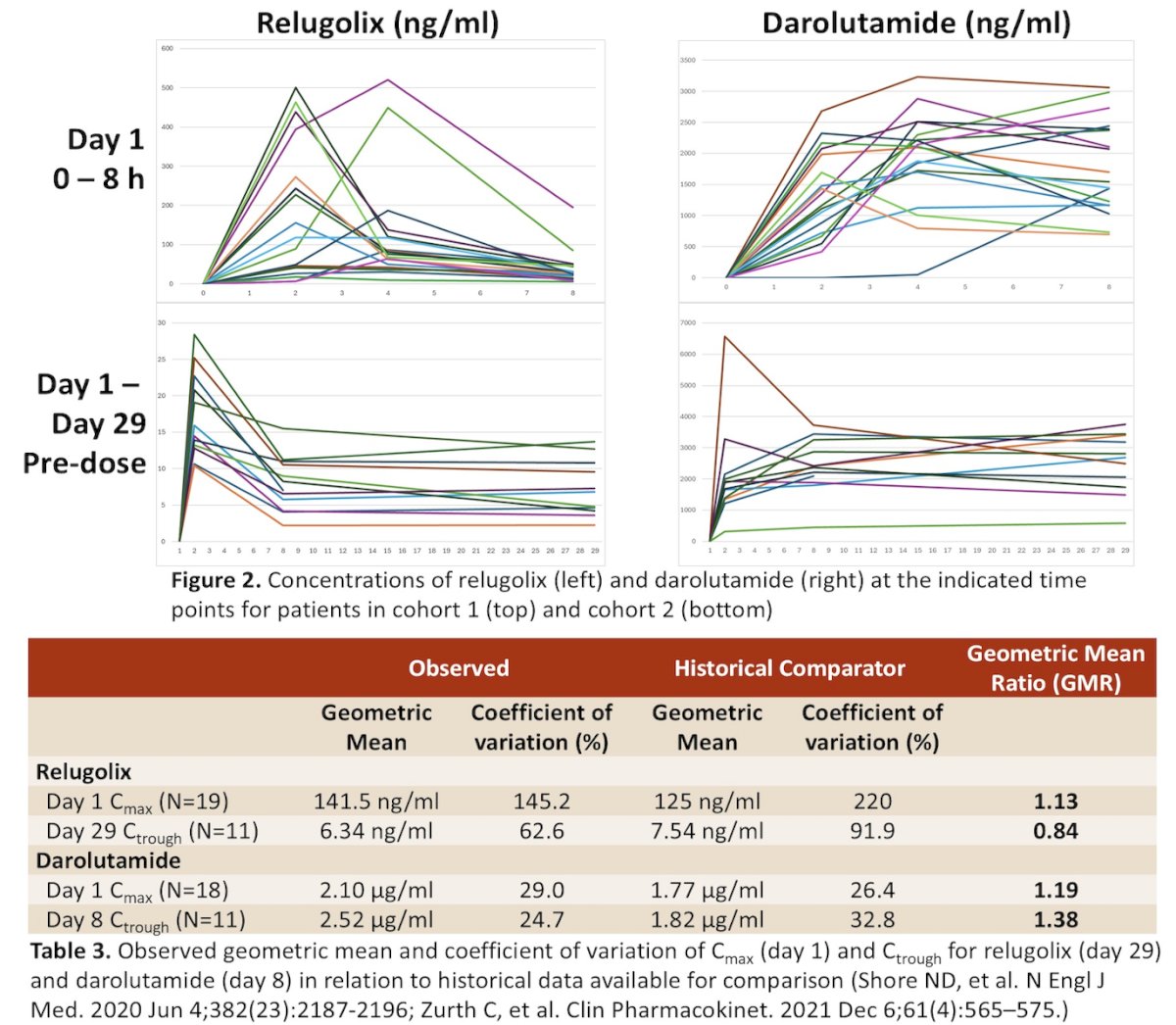
Single dose maximum concentrations (Cmax) on D1 for relugolix and darolutamide, and D29 pre-dose trough level (Ctrough) for relugolix were similar to historical monotherapy comparators with geometric mean ratios (GMR) between 0.80-1.25, while D8 Ctrough for darolutamide was slightly outside this range:
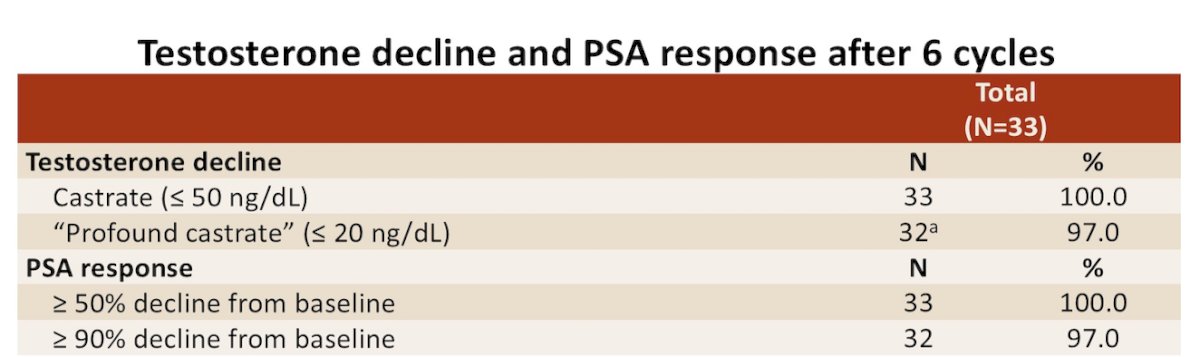
By cycle 7 (C7) D1, 15 patients experienced Grade ≥3 adverse events: 12 lymphopenia (3 possibly related to darolutamide), with the remainder not treatment related. There were no patients who discontinued relugolix or darolutamide, although 3 dose reduced doses of darolutamide. All 33 patients achieved castrate testosterone < 50 ng/dl, and 32/33 (97%) achieved profound castrate testosterone < 20 ng/dl (1 with testosterone 24 ng/dl on C7 D1). PSA decline of ≥50% was achieved in all patients and decline ≥90% in 32/33 (97%) by C7 D1:
Dr. Choudhury concluded his presentation discussing results from CLEARED, a trial assessing a comeback from a long-course ADT with relugolix and darolutamide in hormone-sensitive prostate cancer, with the following take-home points:
- The combination of relugolix and darolutamide was safe and well-tolerated during the first 6 treatment cycles, with pharmacokinetic parameters similar to historical monotherapy comparators
- Appropriate initial testosterone and PSA reduction were observed, and patients will be followed after the end of treatment for the primary endpoint of testosterone recovery
- Patients will be followed after the end of treatment for the primary endpoint of testosterone recovery
- Plasma for ctDNA and FACT-P questionnaires for patient-reported outcomes are being collected for future analysis
Presented by: Atish D. Choudhury, MD, PhD, Medical Oncologist, Clinical/Translational Investigator, Lank Center for Genitourinary Oncology, Dana Farber Cancer Institute, Boston, MA
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Associate Professor of Urology, Georgia Cancer Center, Wellstar MCG Health, @zklaassen_md on Twitter during the American Society of Clinical Oncology Genitourinary (ASCO) Annual Meeting held in Chicago, IL between May 29th and June 1st, 2026