(UroToday.com) The 2026 ASCO annual meeting featured a prostate cancer session and a presentation by Dr. Rana McKay discussing a quality of life analysis from COMRADE, a multicenter, randomized, phase 2, investigator-initiated ETCTN trial of olaparib + radium-223 versus radium-223 in metastatic castration resistant prostate cancer (mCRPC) with bone metastases.
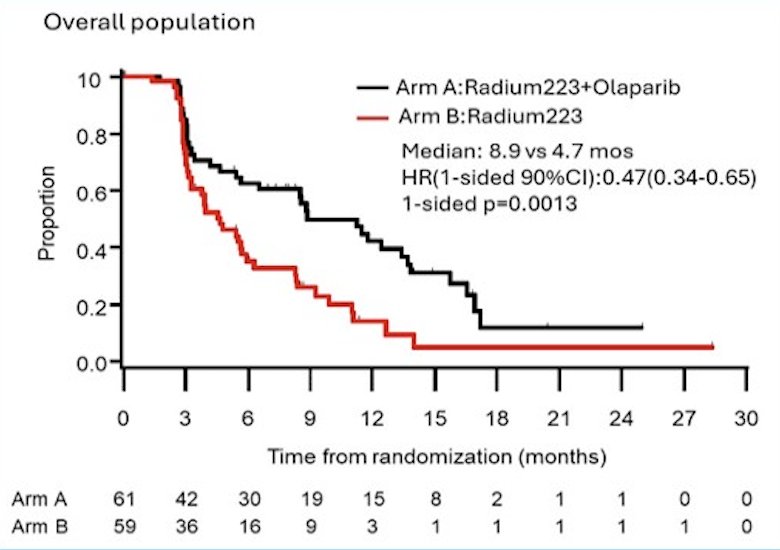
Bone metastases occur in ~90% of patients with advanced mCRPC and are associated with symptomatic skeletal events, including pathologic fractures, spinal cord compression, or the need for palliative radiation or surgery. Radium-223 is an α-emitting radioisotope that improves overall survival in men with mCRPC and bone metastases. In the ALSYMPCA trial, radium-223 was also associated with improved quality of life, delayed time to first opioid use, and pain palliation.1 Dr. McKay and colleagues previously reported superior radiographic progression-free survival with the addition of olaparib to radium-223 in the randomized phase 2 COMRADE study:2
At the ASCO 2026 annual meeting, Dr. McKay reported patient-reported quality of life outcomes from the COMRADE trial.
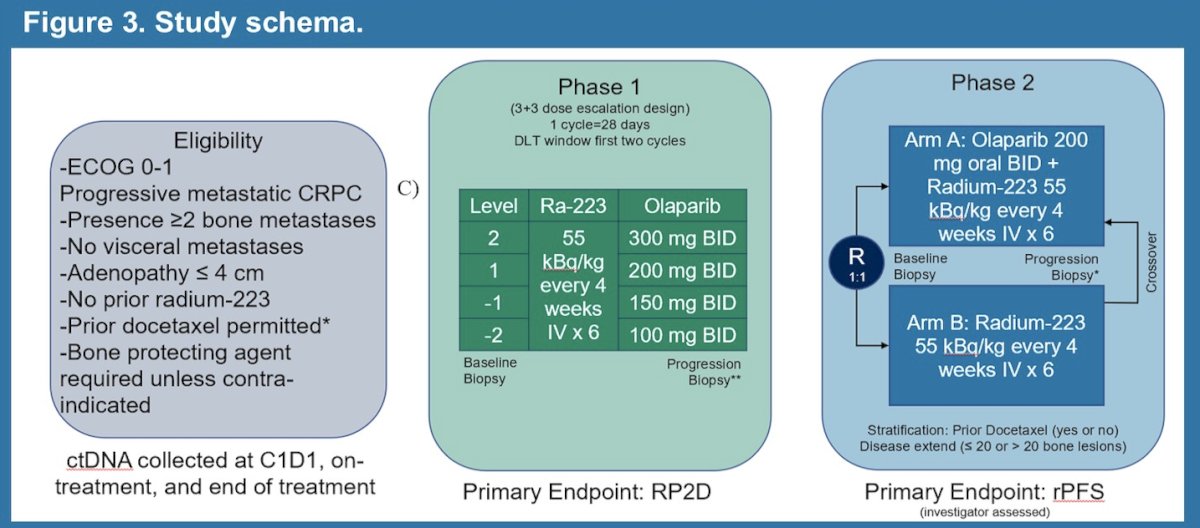
Patients were randomized 1:1 to olaparib 200 mg twice daily + radium-223 (Arm A) or radium-223 alone (Arm B):
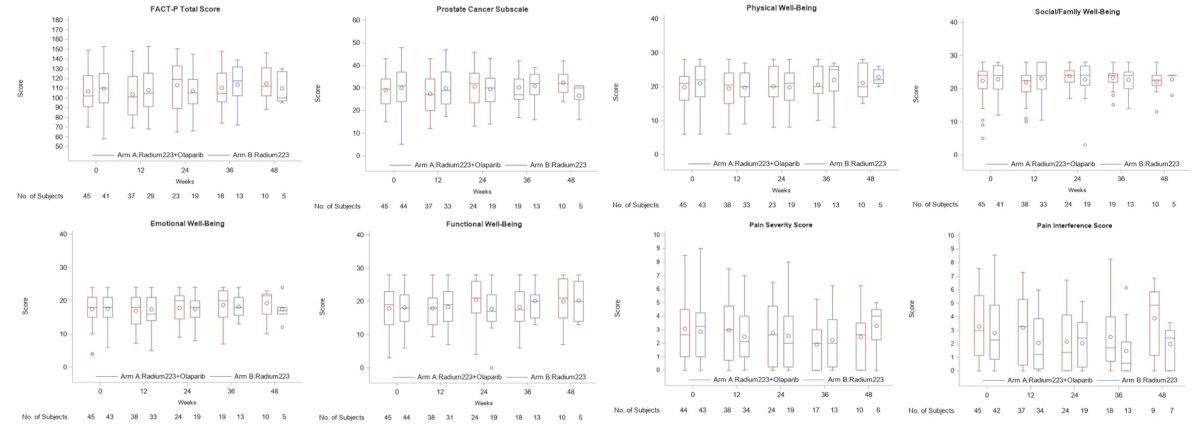
Quality of life was assessed using the Functional Assessment of Cancer Therapy-Prostate (FACT-P) and Brief Pain Inventory (BPI) at baseline and every 12 weeks. Mixed-effects ANCOVA models assessed treatment effects on quality of life changes from baseline, adjusting for baseline score, timepoint, age, and ECOG performance status. Least squares mean changes were reported for each arm with between-arm differences and 95% confidence intervals. Analysis was limited to patients with baseline and ≥1 post-baseline assessment within 24 weeks.
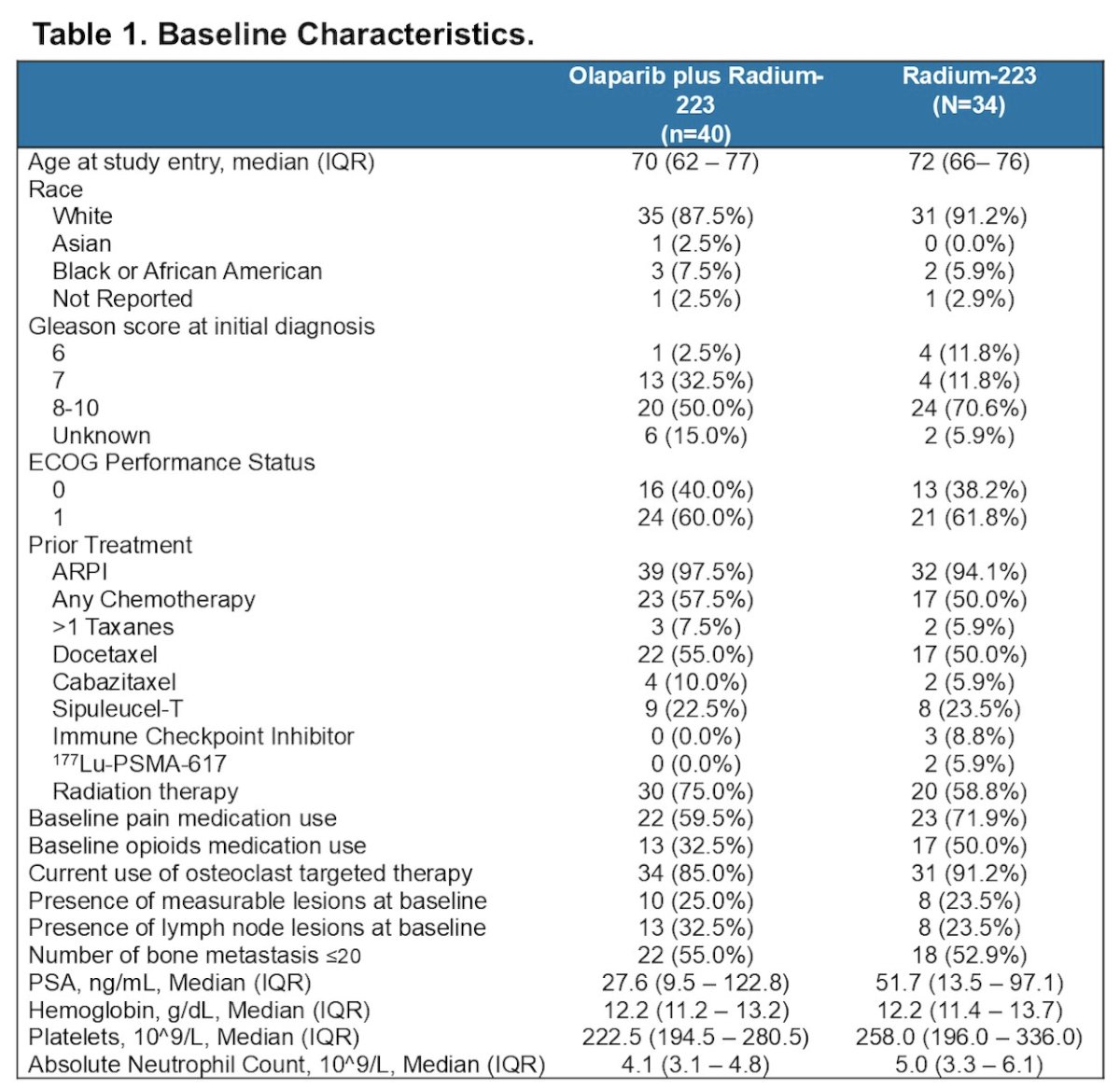
Of 114 treated patients, 74 (65%) were evaluable for quality of life analysis (Arm A, n = 40; Arm B, n = 34), including 71 (62%) for FACT-P and 72 (63%) for BPI pain severity and pain interference. Baseline characteristics were well balanced: the median age was 70 and 72 years, ECOG performance status 1 was present in 60% and 62%, prior docetaxel was received by 55% and 50%, > 20 bone metastases were present in 45% and 47%, and pain medication use at baseline was reported in 60% and 72% of patients in Arms A and B, respectively:
There were no significant differences in least squares mean change from baseline in FACT-P total score between arms at week 12 (Arm A: -5.09 versus Arm B: -0.23; difference -4.87, 95% CI -13.4 to 3.62) or week 24 (Arm A: -1.41 versus Arm B: -3.20; difference 1.79, 95% CI -8.28 to 11.9). Similarly, no significant between-arm differences were observed in least squares mean changes in BPI pain severity at week 12 (difference 0.44, 95% CI -0.44 to 1.33) or week 24 (difference -0.20, 95% CI -1.32 to 0.93):
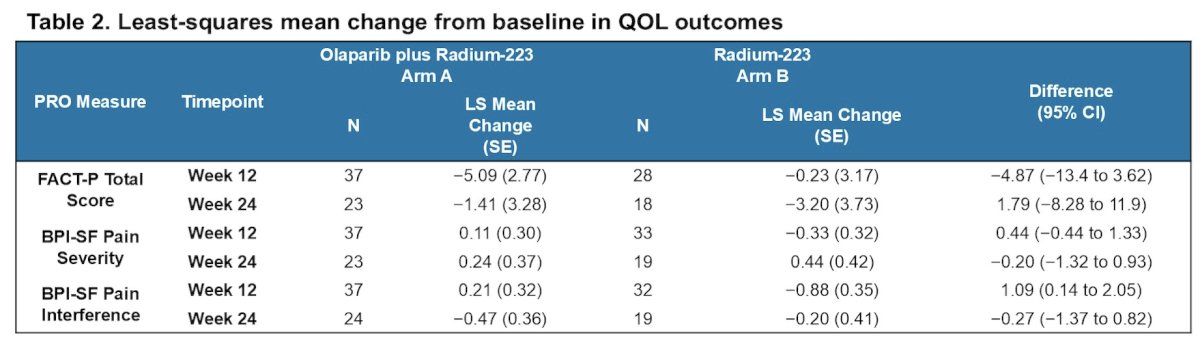
Arm B showed greater improvement in BPI pain interference at week 12 (least squares mean change: Arm A +0.21 versus Arm B -0.88; difference 1.09, 95% CI 0.14 to 2.05), but this difference was not sustained at week 24 (difference -0.27, 95% CI -1.37 to 0.82):
Dr. McKay concluded her presentation, discussing a quality of life analysis from COMRADE, by stating that the addition of olaparib to radium-223 achieved superior radiographic progression-free survival without significant detriment to patient-reported quality of life or pain compared to radium-223 alone, supporting the tolerability of this combination in mCRPC patients with bone metastases
Presented by: Rana R. McKay, MD, Professor of Medicine and Urology, Department of Medicine, University of California, San Diego Moores Cancer Center, La Jolla, CA, USA
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Associate Professor of Urology, Georgia Cancer Center, Wellstar MCG Health, @zklaassen_md on Twitter during the American Society of Clinical Oncology Genitourinary (ASCO) Annual Meeting held in Chicago, IL between May 29th and June 1st, 2026
References:
- Parker C, Nilsson S, Heinrich D, et al. Alpha emitter radium-223 and survival in metastatic prostate cancer. N Engl J Med 2013;369(3):213-223.
- McKay RR, Xie W, Ajmera A, et al. Multicenter, randomized, phase II trial of olaparib plus radium-223 versus radium-223 in men with castration-resistant prostate cancer with bone metastases (COMRADE). J Clin Oncol. 2026 May 7 [Epub ahead of print].