(UroToday.com) The 2026 American Society of Clinical Oncology Genitourinary (ASCO) Annual Meeting held in Chicago, IL, was host to the Prostate, Testicular, and Penile Cancer - Oral Abstracts. Dr. David Olmos discussed PARPi-Palooza: Sorting out the many options in prostate cancer.
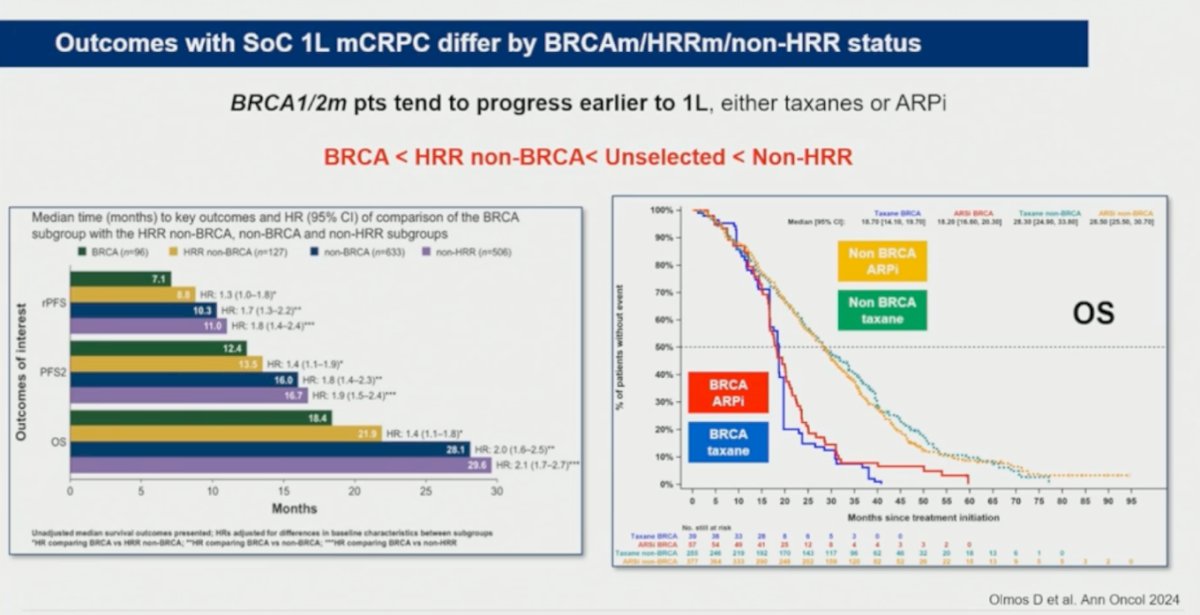
Dr. Olmos highlighted that outcomes with standard-of-care first-line mCRPC treatment differ significantly according to BRCA and HRR status. Patients harboring BRCA1/2 alterations tended to progress earlier on first-line therapies, including both taxane- and ARPI-based approaches, compared with patients with non-BRCA HRR alterations, unselected populations, and non-HRR tumors. Across multiple clinical endpoints, outcomes followed a consistent pattern: BRCA-mutated disease had the poorest prognosis, followed by HRR non-BRCA tumors, while non-HRR disease demonstrated the most favorable outcomes.1 Kaplan-Meier overall survival curves below further illustrate worse outcomes among BRCA-mutated patients regardless of whether they received ARPI- or taxane-based therapy, underscoring the aggressive biology and unmet clinical need in this molecular subgroup.
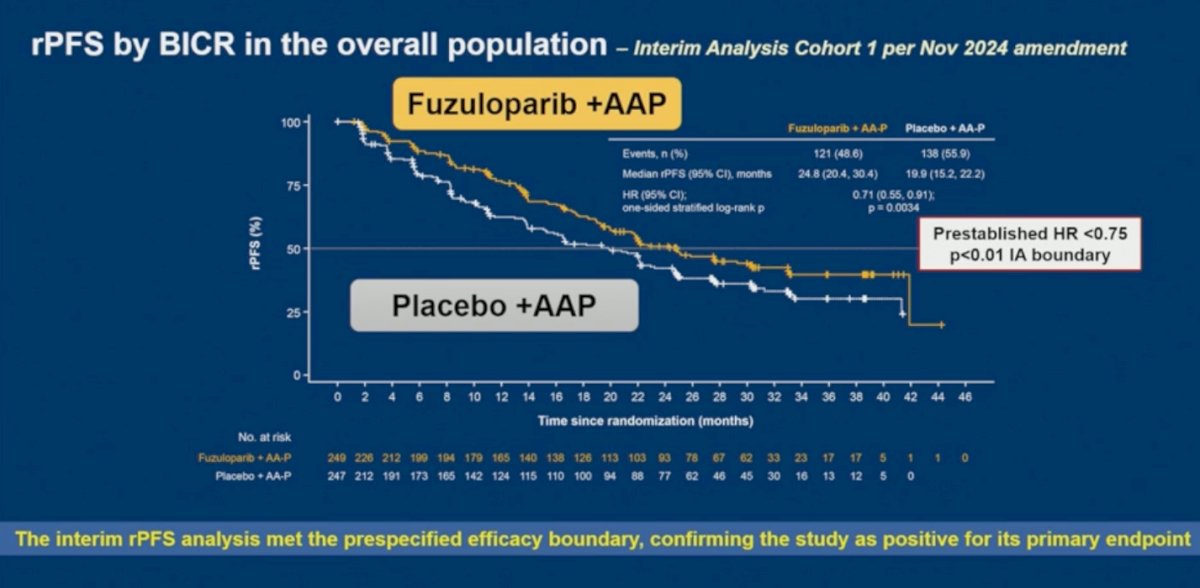
An interim analysis of FUZUPRO confirmed the study as positive for its primary endpoint. Fuzuloparib plus abiraterone acetate and prednisone significantly improved blinded independent central review-assessed radiographic progression-free survival compared with placebo plus AA-P, with a median radiographic progression-free survival of 24.8 versus 19.9 months (HR 0.71; 95% CI 0.55–0.91; p=0.0034). Dr. Olmos highlighted that the prespecified efficacy boundary was met, which required a hazard ratio <0.75 and p<0.01 at interim analysis.
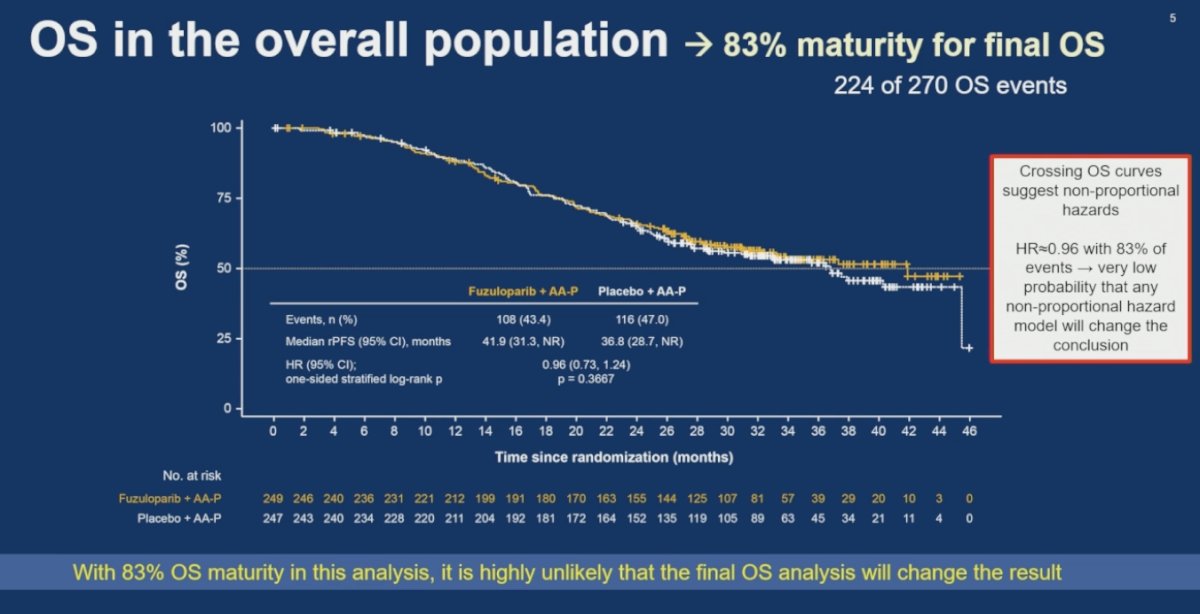
Dr. Olmos further noted that the overall survival curves demonstrated crossing over time, suggesting the presence of non-proportional hazards. However, despite this observation, the overall survival hazard ratio remained 0.96 with approximately 83% of events already observed, indicating a very low likelihood that alternative non-proportional hazards modeling would meaningfully alter the overall conclusion regarding survival outcomes.
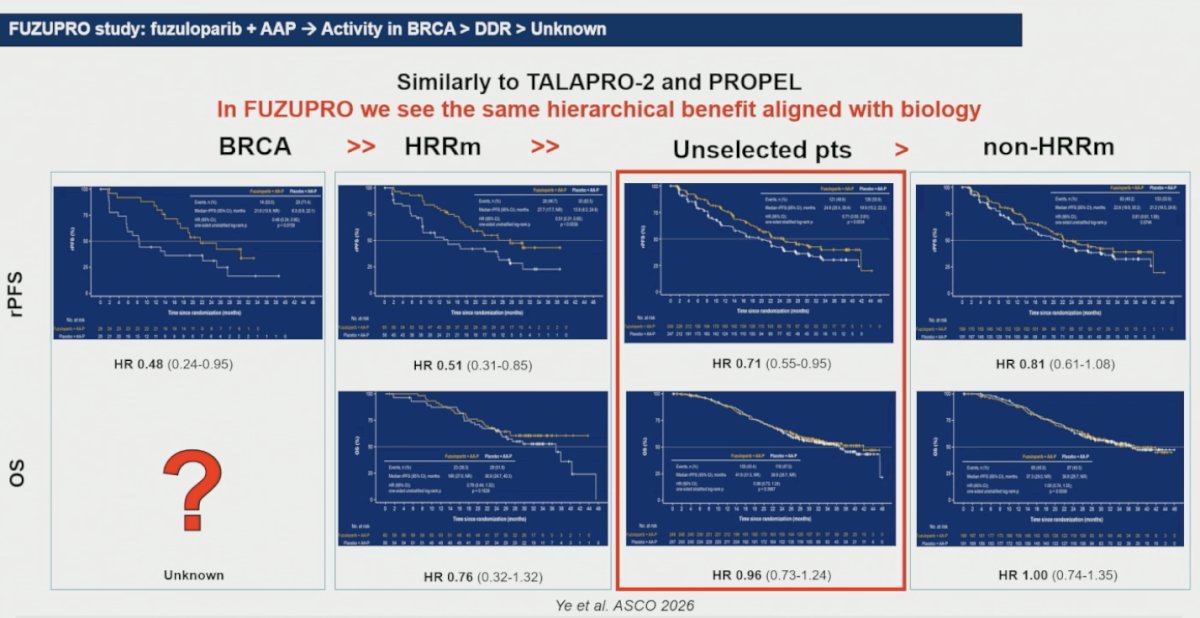
Dr. Olmos highlighted that the FUZUPRO results followed a hierarchical pattern of benefit aligned with tumor biology, similar to what has previously been observed in TALAPRO-2 and PROPEL.2,3 The greatest radiographic progression-free survival benefit was observed in patients harboring BRCA alterations (HR 0.48), followed by the broader HRR-deficient population (HR 0.51), then the unselected overall population (HR 0.71), while the smallest magnitude of benefit was seen among non-HRR-altered tumors (HR 0.81). A similar trend was observed for overall survival. While overall survival data in BRCA-mutated patients remained immature, exploratory analyses suggested more favorable outcomes in the HRR-deficient subgroup (HR 0.76), whereas the overall population demonstrated no clear overall survival difference (HR 0.96), and the non-HRR subgroup showed essentially neutral results (HR 1.00) as illustrated below:
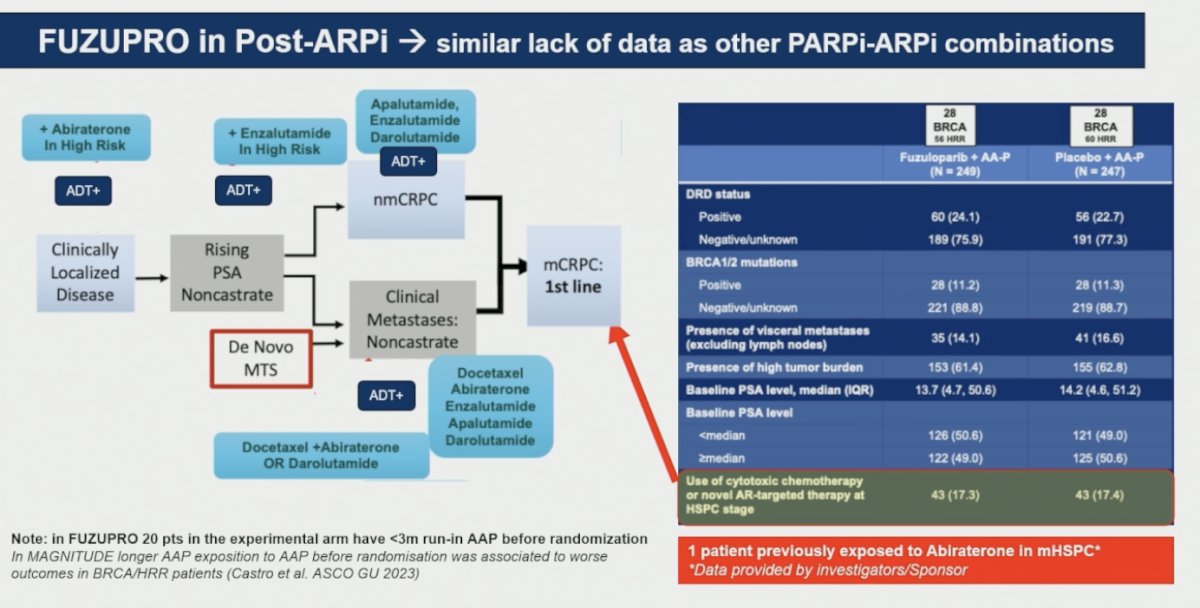
Dr. Olmos noted that, similar to other PARP inhibitor and ARPI combination studies in the first-line mCRPC setting, FUZUPRO included very limited data regarding patients previously exposed to ARPI therapy in the metastatic hormone-sensitive setting. Only 17.3% of patients in the fuzuloparib arm and 17.4% in the placebo arm had received prior cytotoxic chemotherapy or novel AR-targeted therapy during the hormone-sensitive disease stage, and notably, only one patient had prior exposure to abiraterone in the mHSPC setting. He emphasized that this remains a major limitation across studies evaluating PARP inhibitor and ARPI combinations in first-line mCRPC, particularly as treatment intensification continues to move earlier in the disease course.
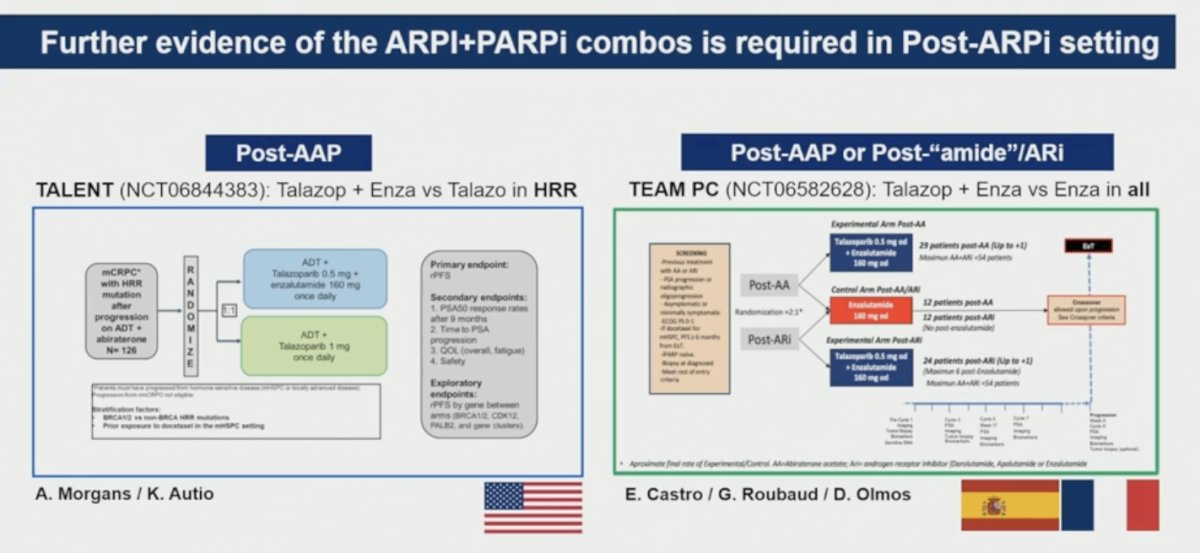
Dr. Olmos highlighted that additional evidence supporting PARP inhibitor and ARPI combinations in the post-ARPI setting remains needed. He discussed ongoing studies, including TALENT, evaluating talazoparib plus enzalutamide versus talazoparib alone in HRR-altered mCRPC progressing after prior abiraterone, as well as TEAM-PC, which is evaluating talazoparib plus enzalutamide versus enzalutamide alone in patients previously treated with abiraterone or other AR pathway inhibitors.
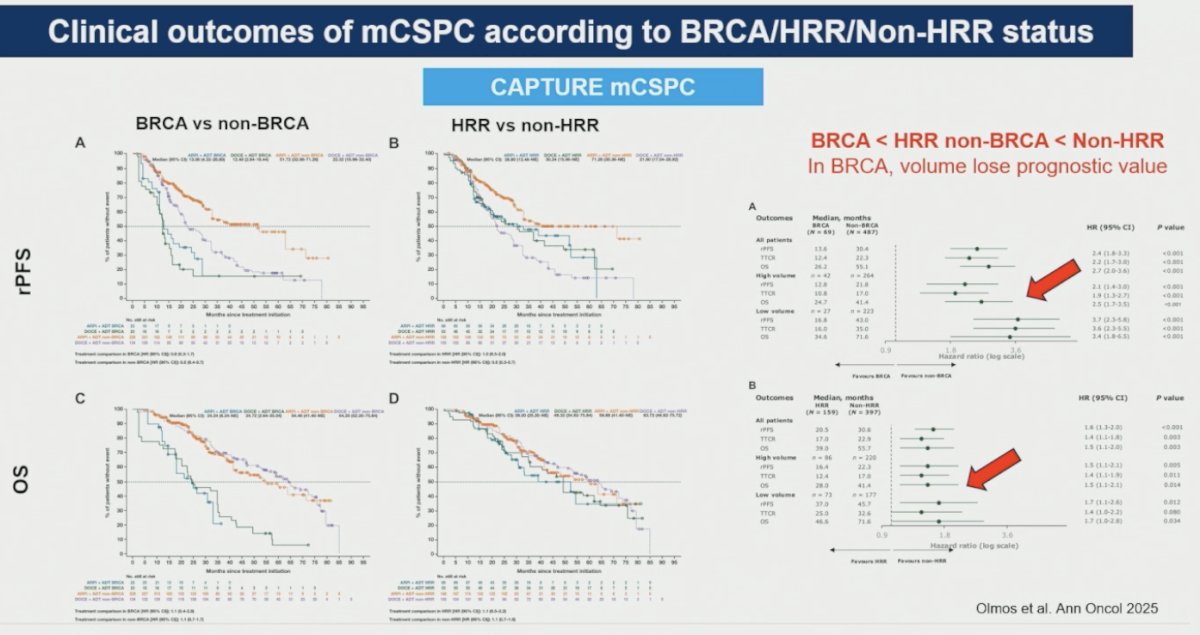
We have also learned from the CAPTURE mCSPC dataset, highlighting that clinical outcomes in metastatic castration-sensitive prostate cancer differ substantially according to BRCA and HRR status. Patients harboring BRCA alterations demonstrated the poorest radiographic progression-free survival and overall survival outcomes, followed by patients with non-BRCA HRR alterations, while non-HRR tumors had the most favorable prognosis. He further noted that, within the BRCA-mutated subgroup, disease volume appeared to lose some of its traditional prognostic value, suggesting that underlying tumor biology may play a dominant role in driving outcomes in these patients.1
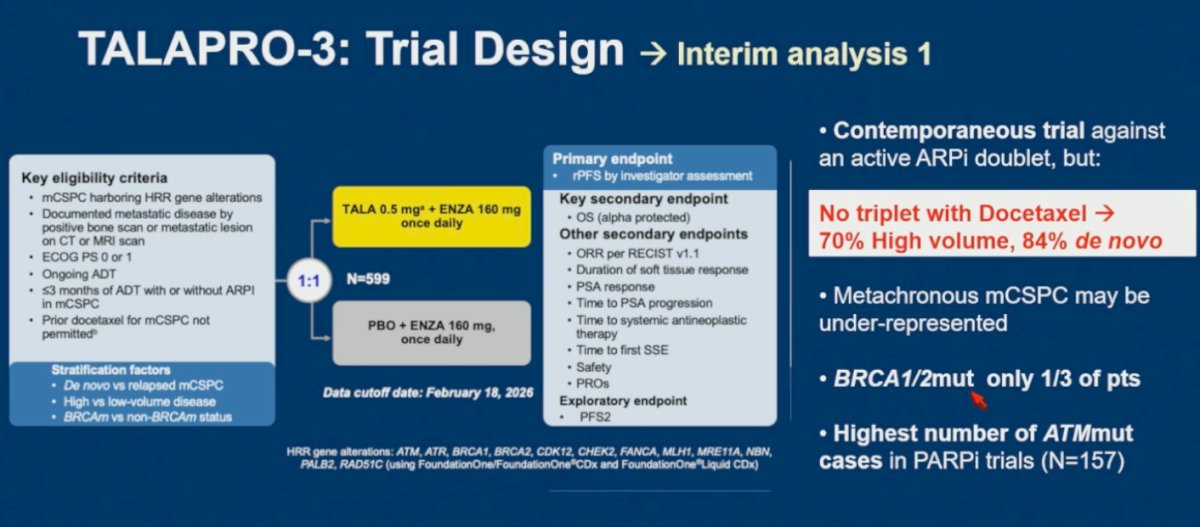
We have now moved forward from the initial PARP inhibitor studies conducted in all-comer populations, as TALAPRO-3 and AMPLITUDE4,5 specifically enrolled patients with HRR-selected disease. Dr. Olmos noted several important considerations when interpreting TALAPRO-3, including the absence of triplet therapy with docetaxel despite 70% of patients having high-volume disease and 84% presenting with de novo metastatic disease. He also highlighted the substantial representation of ATM-mutated tumors across TALAPRO-3 (n=157) while BRCA1/2-mutated patients accounted for approximately one-third of enrolled patients.
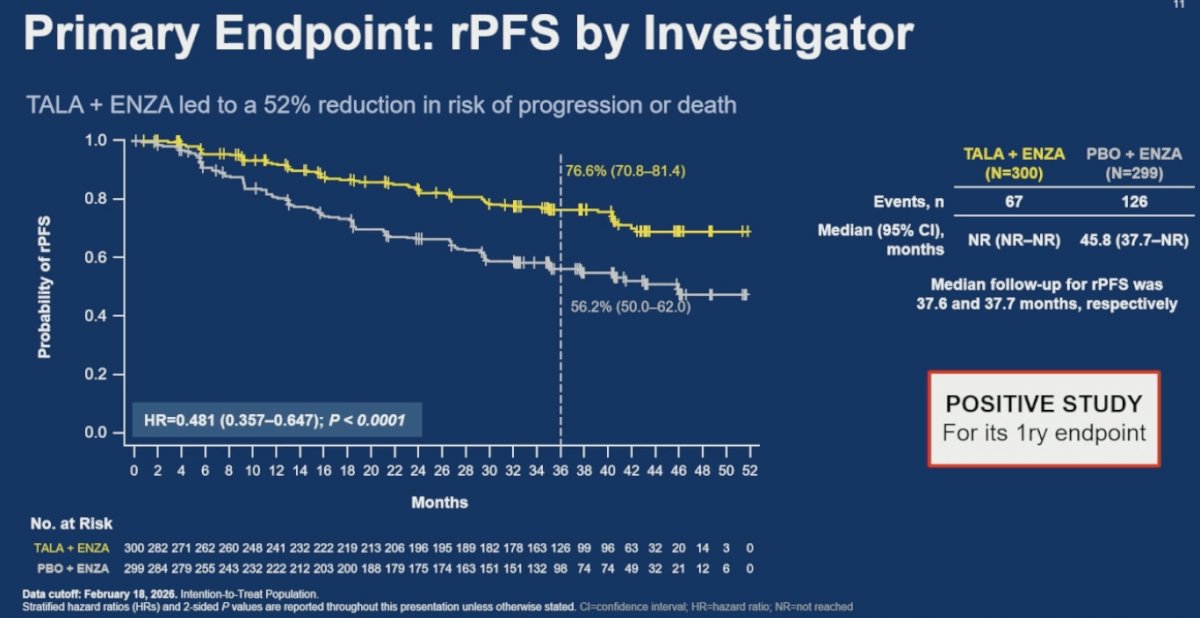
TALAPRO-3 met its primary endpoint, with talazoparib plus enzalutamide significantly improving investigator-assessed radiographic progression-free survival compared with placebo plus enzalutamide in patients with HRR-altered mCSPC. The combination reduced the risk of progression or death by 52% (HR 0.48; 95% CI 0.36–0.65; p<0.0001). Median radiographic progression-free survival was not reached in the talazoparib plus enzalutamide arm compared with 45.8 months in the control arm, with clear separation of the Kaplan-Meier curves favoring the combination strategy.5
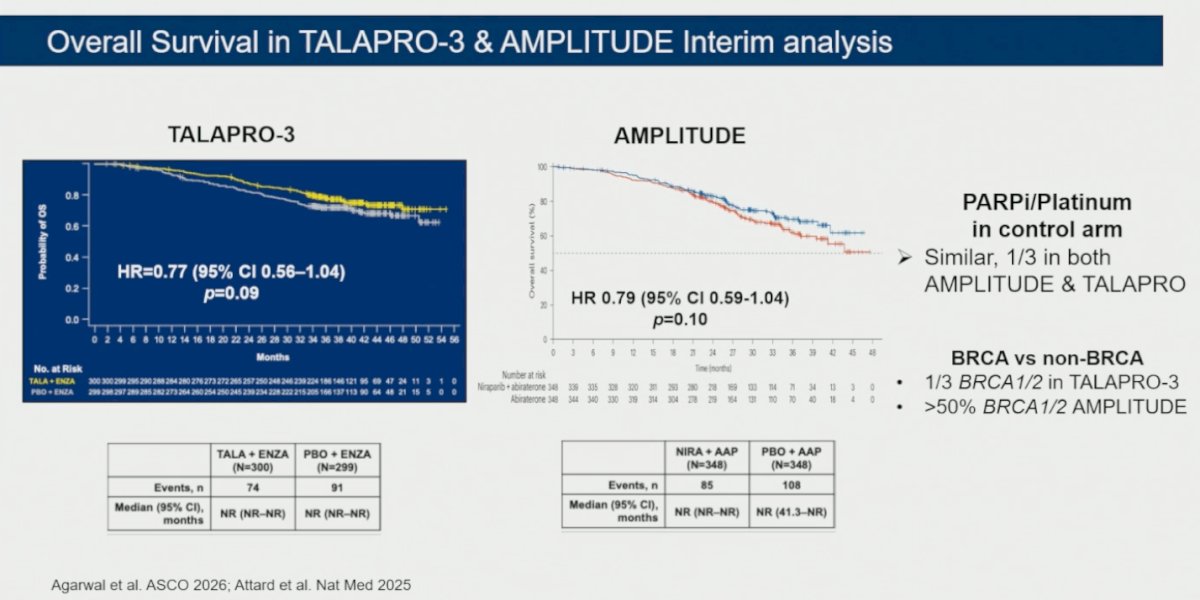
Dr. Olmos compared interim overall survival results from TALAPRO-3 and AMPLITUDE,4,5 noting that both studies demonstrated similar trends favoring PARP inhibitor combinations, with hazard ratios of 0.77 and 0.79, respectively, although neither analysis was yet statistically significant. He highlighted several important differences between the studies, including that approximately one-third of patients in both trials received PARP inhibitors or platinum-based therapy in the control arm after progression. Additionally, BRCA1/2-mutated patients represented only about one-third of TALAPRO-3, whereas they accounted for more than 50% of patients enrolled in AMPLITUDE, which may partially explain differences observed between the studies.
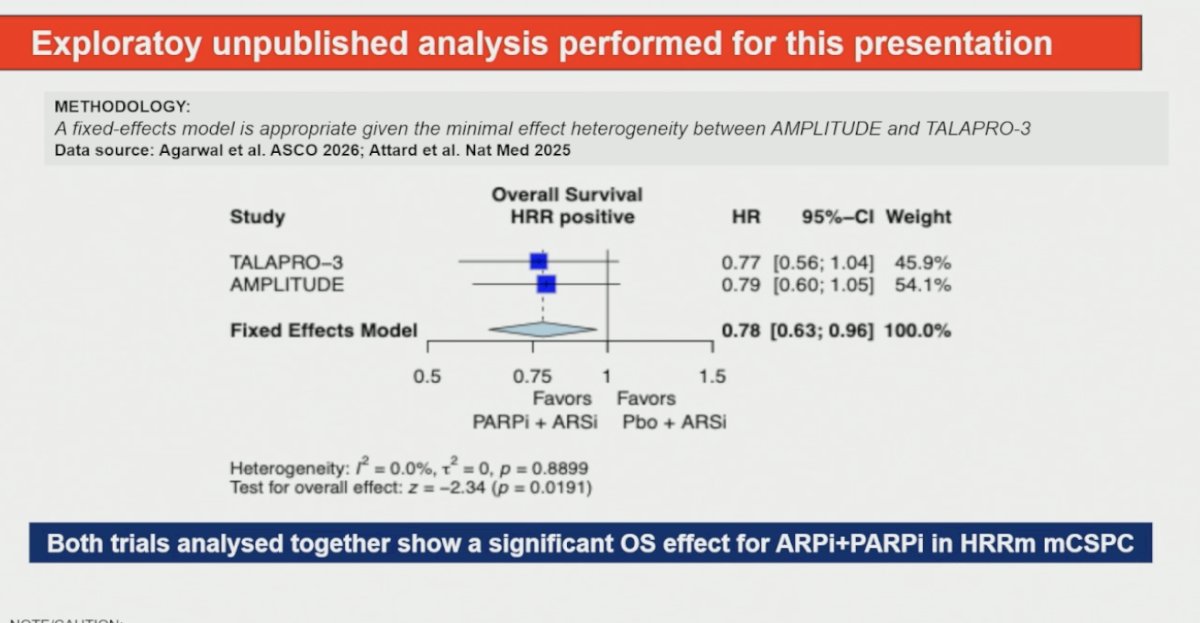
Dr. Olmos performed an exploratory unpublished pooled analysis for this presentation combining TALAPRO-3 and AMPLITUDE, noting minimal heterogeneity between studies, supporting the use of a fixed-effects model. When analyzed together, PARP inhibitor plus ARSI combinations demonstrated a statistically significant overall survival benefit in patients with HRR-altered mCSPC, with a pooled hazard ratio of 0.78 (95% CI 0.63–0.96; p=0.0191) as shown below.
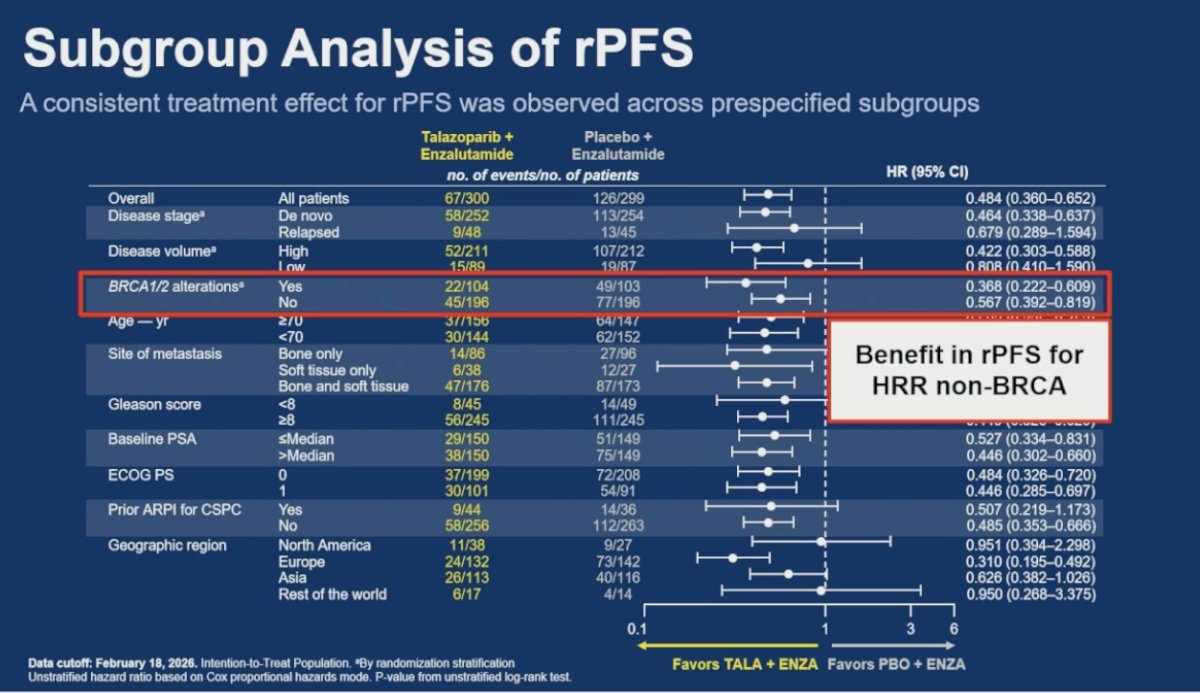
Subgroup analyses from TALAPRO-3 demonstrated a consistent radiographic progression-free survival benefit across prespecified patient populations. Importantly, benefit was observed not only in BRCA1/2-altered tumors (HR 0.37), but also among patients with non-BRCA HRR alterations (HR 0.57), suggesting clinical activity of talazoparib plus enzalutamide beyond BRCA-mutated disease.5 Therefore we need to identify the gene mutations that are driving this benefit in non-BRCA patients.
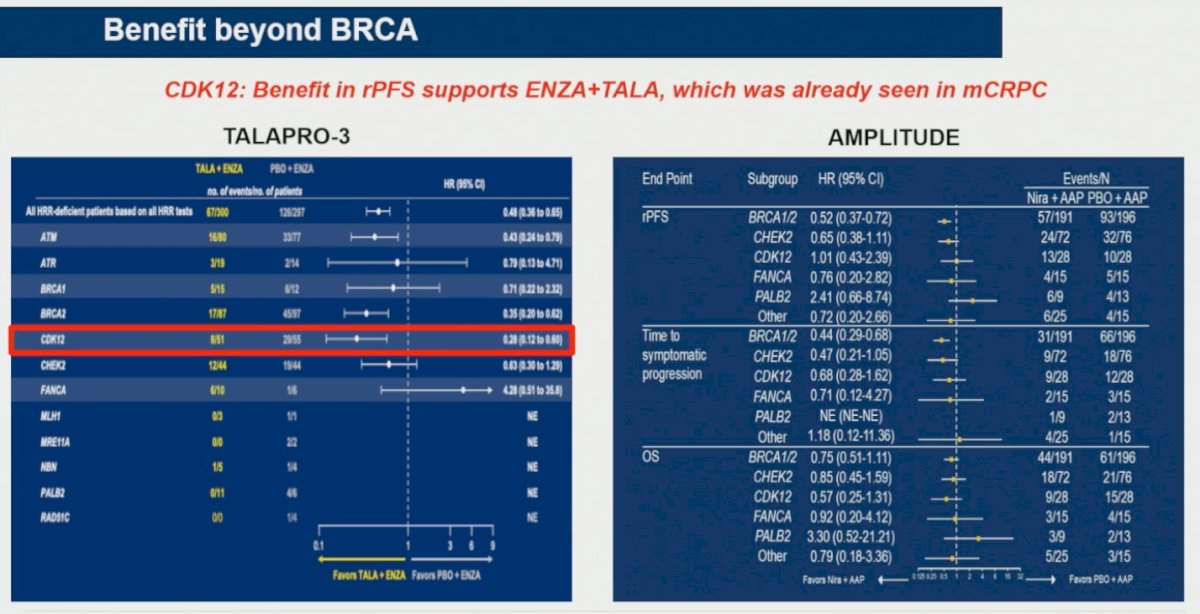
Dr. Olmos noted that one of the most interesting signals beyond BRCA alterations was observed in patients harboring CDK12 alterations. In TALAPRO-3, the subgroup of patients with CDK12-mutated tumors appeared to derive meaningful radiographic progression-free survival benefit with talazoparib plus enzalutamide (HR 0.28; 95% CI 0.12–0.60), consistent with signals previously observed in the mCRPC setting.
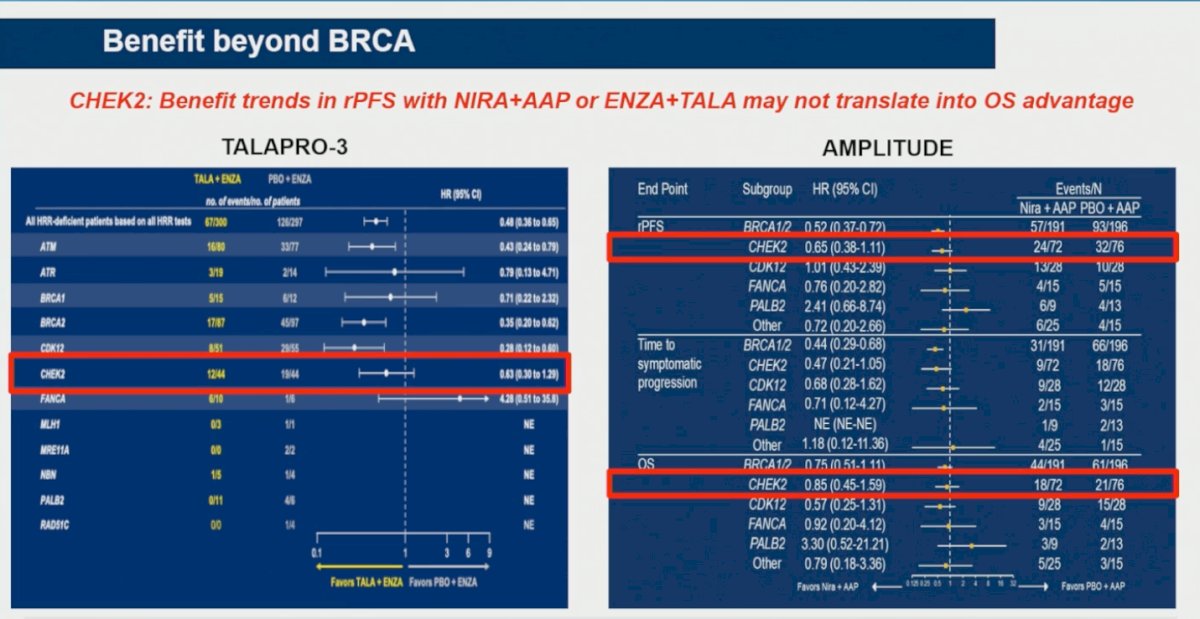
Moreover, Dr. Olmos highlighted differences in outcomes among patients harboring CHEK2 alterations across TALAPRO-3 and AMPLITUDE. In TALAPRO-3, the radiographic progression-free survival signal for talazoparib plus enzalutamide in CHEK2-mutated disease appeared more modest (HR 0.63; 95% CI 0.30–1.29), whereas AMPLITUDE demonstrated a numerically stronger radiographic progression-free survival benefit with niraparib plus abiraterone (HR 0.65; 95% CI 0.38–1.11).
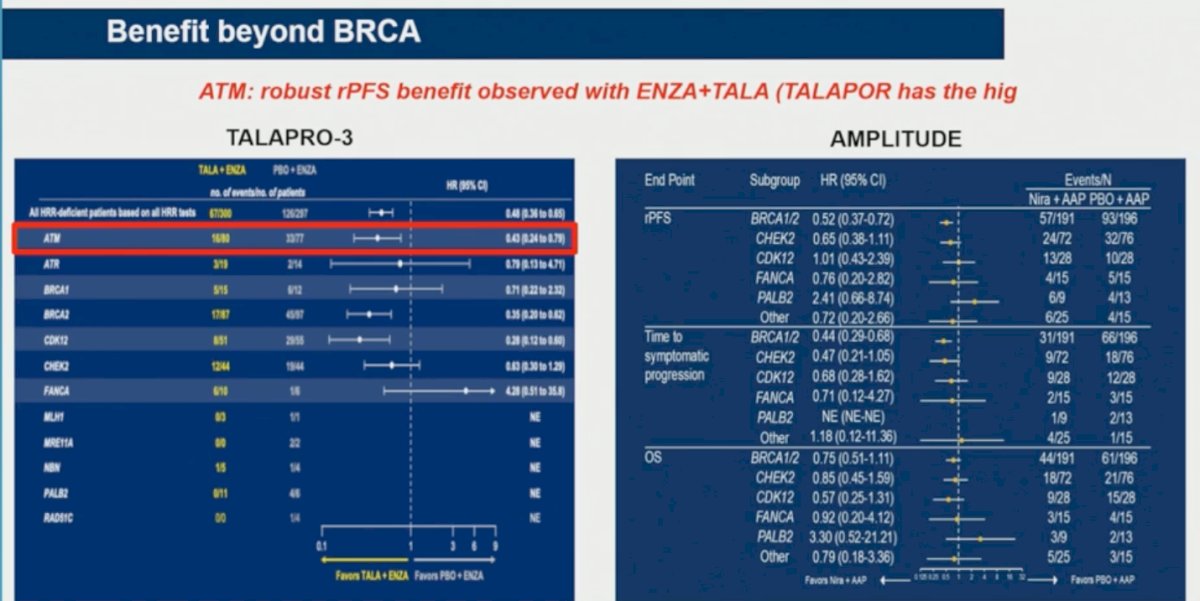
The third candidate is ATM, there is encouraging activity in patients harboring ATM alterations, noting a robust radiographic progression-free survival benefit with talazoparib plus enzalutamide in TALAPRO-3 (HR 0.43; 95% CI 0.23–0.78). He emphasized that TALAPRO-3 included the largest cohort of ATM-mutated patients evaluated in a PARP inhibitor trial to date.
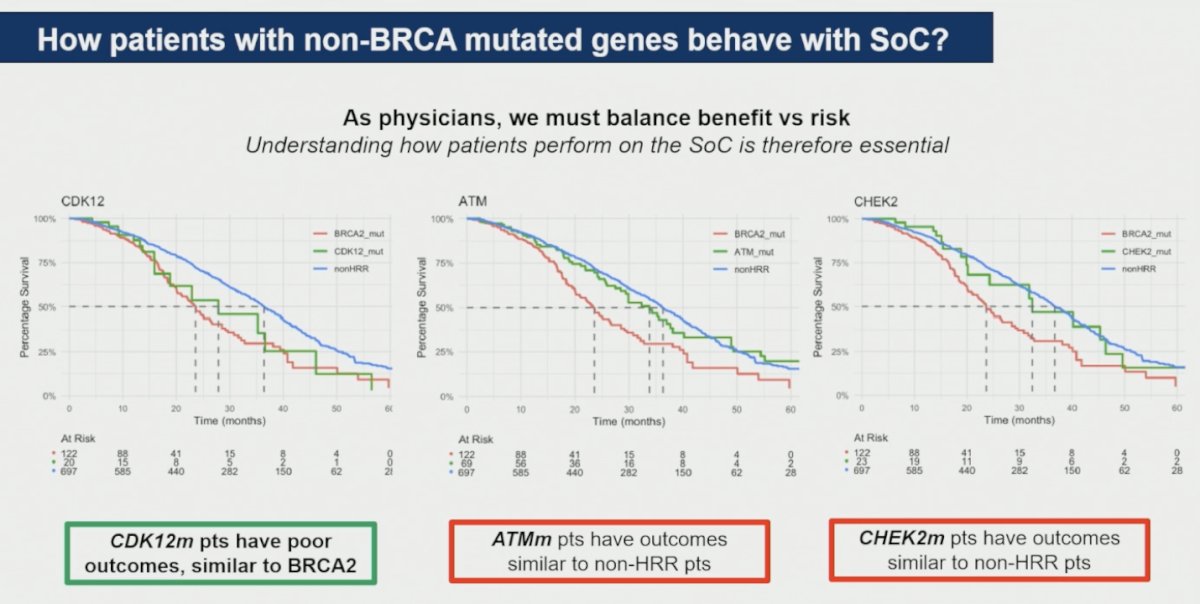
Lastly, Dr. Olmos highlighted that patients harboring CDK12 alterations demonstrated poor outcomes with standard-of-care therapy, with survival outcomes resembling those observed in BRCA2-mutated disease. In contrast, patients with ATM and CHEK2 alterations appeared to have outcomes more similar to those seen in non-HRR-altered tumors.
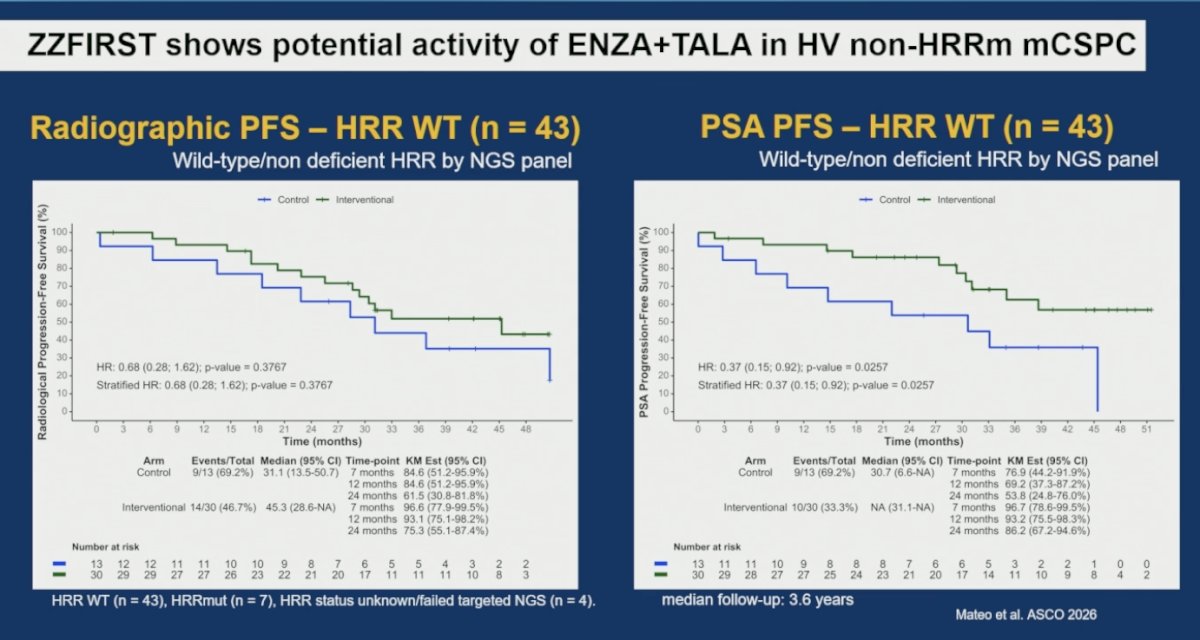
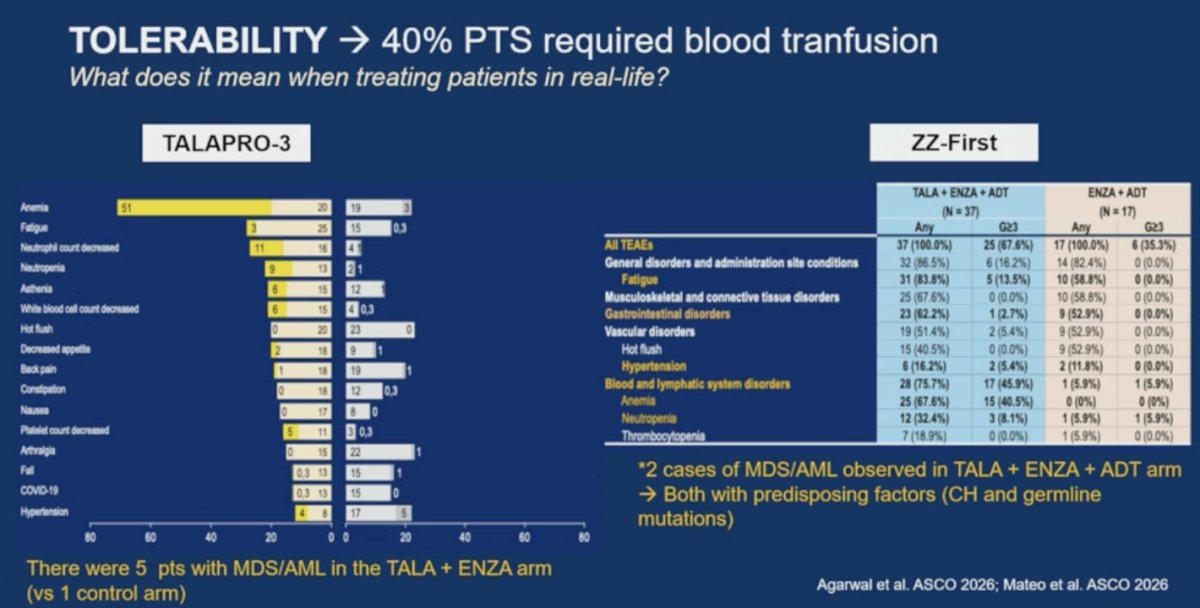
Dr. Olmos also discussed the investigator-initiated ZZFIRST trial presented by Dr. Mateo, highlighting signals of potential activity with enzalutamide plus talazoparib even among patients with high-volume non-HRR-mutated mCSPC. In the HRR wild-type subgroup, the combination demonstrated numerical improvements in radiographic progression-free survival and significant improvement in PSA progression-free survival (HR 0.37; p=0.0257), suggesting that selected non-HRR populations may still derive benefit from PARP inhibitor combinations.
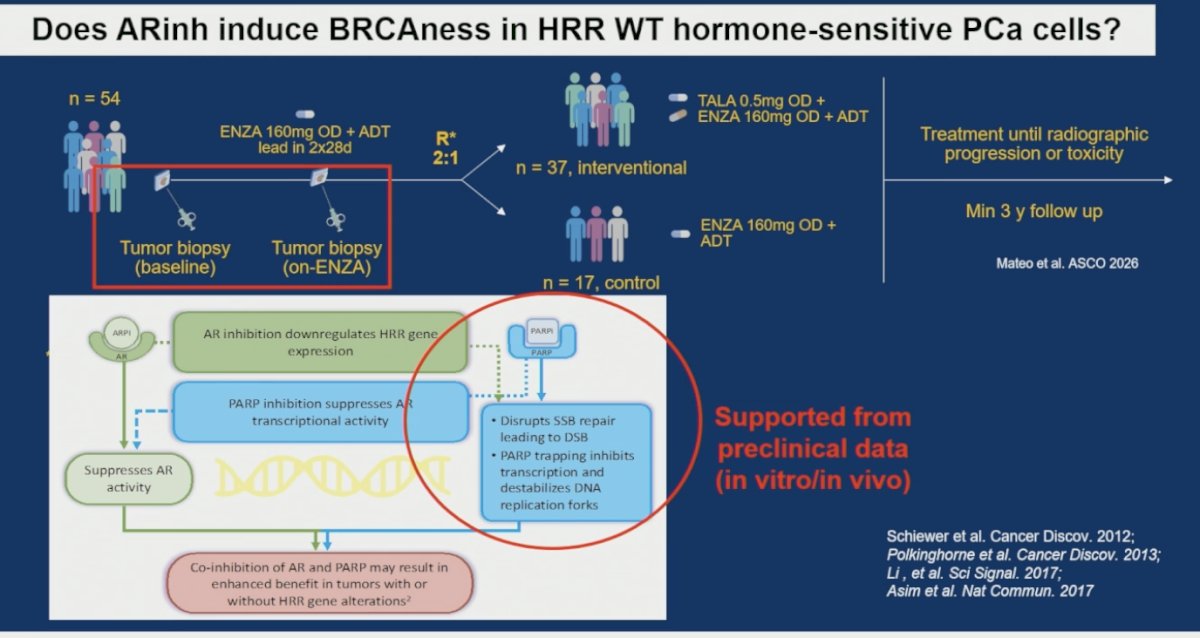
However, Dr. Olmos noted that the most important information from this trial came from the translational analyses. The hypothesis that AR inhibition induces a “BRCAness” phenotype in HRR wild-type prostate cancer remains incompletely understood. He discussed the ZZFIRST translational design, which incorporated paired baseline and on-treatment tumor biopsies after an enzalutamide lead-in period to better characterize tumor adaptation to AR blockade. While preclinical studies have suggested that AR inhibition may downregulate HRR gene expression and enhance susceptibility to PARP inhibition, clinical validation of a true functional HR-deficient state in HRR wild-type tumors remains limited.
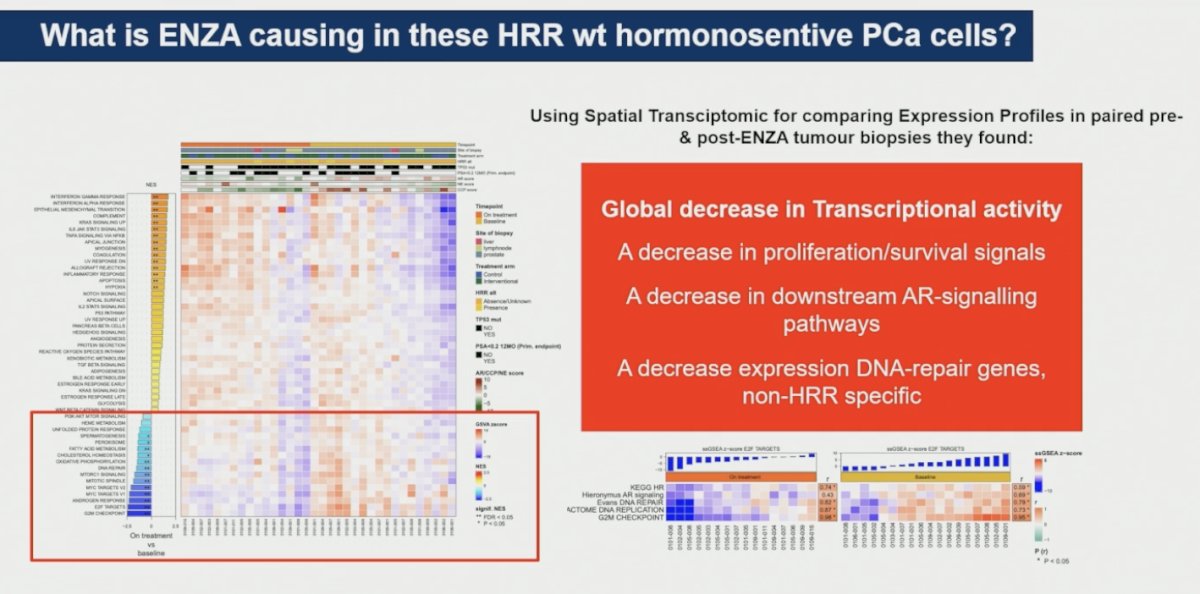
Using spatial transcriptomics to compare expression profiles in paired pre- and post-enzalutamide tumor biopsies, investigators observed a global decrease in transcriptional activity following AR inhibition. This was accompanied by reductions in proliferation and survival signaling, downstream AR-signaling pathways, and expression of DNA repair genes, although these changes were not specific to homologous recombination repair pathways.
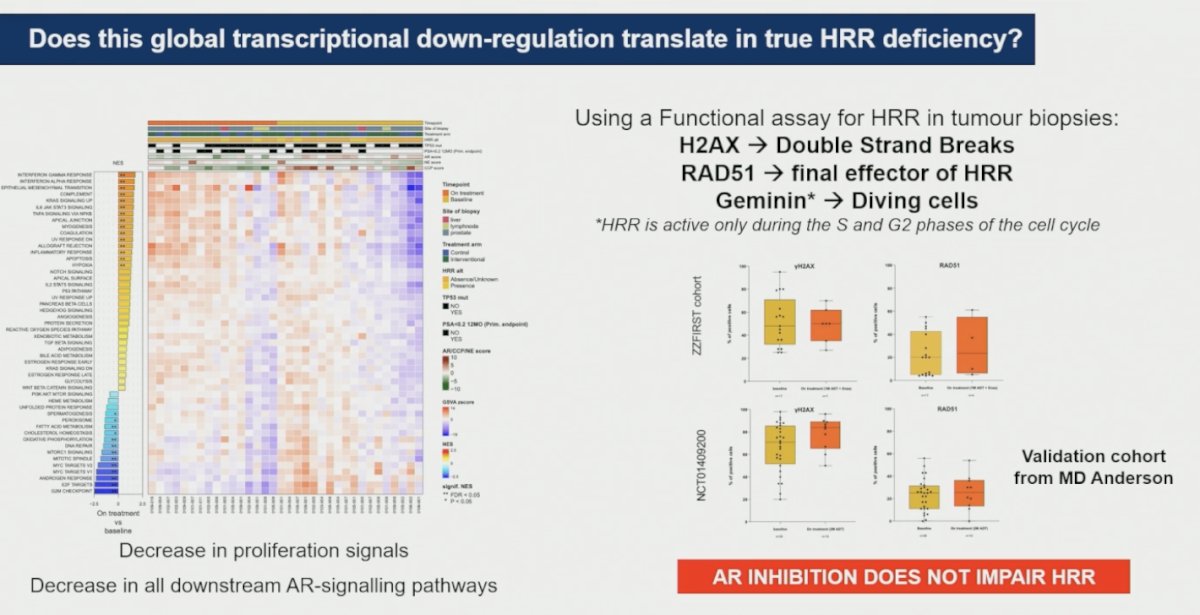
To determine whether this global transcriptional downregulation translated into a true homologous recombination repair-deficient state, investigators performed functional HRR assays on paired tumor biopsies. These analyses evaluated γH2AX as a marker of double-strand DNA breaks, RAD51 as a key final effector of homologous recombination repair, and geminin as a marker of actively dividing cells. Despite reductions in proliferation signals and downstream AR-signaling pathways after enzalutamide exposure, functional analyses, including a validation cohort from MD Anderson, demonstrated that AR inhibition did not impair homologous recombination repair function, arguing against the induction of a true HRR-deficient phenotype in HRR wild-type tumors.
Dr. Olmos also spent time placing the toxicity profile of PARP inhibitor combinations into clinical perspective, emphasizing that efficacy outcomes must be weighed carefully against treatment-related adverse events. He highlighted that approximately 40% of patients required blood transfusions, with frequent dose reductions and treatment interruptions observed across studies. He further noted concern regarding rare but potentially fatal toxicities, including myelodysplastic syndrome and acute myeloid leukemia, particularly as these agents move earlier in the disease course and patients remain exposed for longer periods. In this context, he underscored the potential importance of screening for clonal hematopoiesis and germline alterations when selecting patients for PARP inhibitor-based treatment strategies.
Dr Olmos wrapped up his discussion of this three abstracts with the following key points:
- TALAPRO-3 reinforces ARPI + PARPi combinations as a standard-of-care approach for patients with BRCA1/2-mutated mCSPC
- Selected patients with non-BRCA HRR alterations may also derive benefit from enzalutamide plus talazoparib
- Fuzuloparib plus AAP emerged as a potential option for patients with BRCA1/2-mutated, ARPI-naïve mCRPC
- No clear benefit was observed in non-BRCA HRR-altered or non-HRR populations with fuzuloparib combinations
- Results from the ZZFIRST study suggested that AR inhibition does not induce true HRR deficiency or “BRCAness”
- No clear mechanistic rationale currently supports ARPI + PARPi synergy in HRR-competent prostate cancer
- Overall, use of PARP inhibitor plus ARPI combinations in mCSPC and mCRPC should remain biomarker-driven and balanced against treatment-related toxicities and tolerability
Presented by: David Olmos, MD, PhD, Medical Oncologist, Hospital Universitario 12 de Octubre, Madrid, Spain
Written by: Julian Chavarriaga, MD, Clinical Assistant Professor, Urologic Oncologist, Department of Urology at Penn State Health @chavarriagaj on X during the American Society of Clinical Oncology Genitourinary (ASCO) Annual Meeting held in Chicago, IL between May 29th and June 1st, 2026
References:- Olmos D, Lorente D, Alameda D, Cattrini C, Romero-Laorden N, Lozano R, Lopez-Casas PP, Jambrina A, Capone C, Vanden Broecke AM, Trevisan M, Van Sanden S, Jürgens A, Herrera-Imbroda B, Castro E. Treatment patterns and outcomes in metastatic castration-resistant prostate cancer patients with and without somatic or germline alterations in homologous recombination repair genes. Ann Oncol. 2024 May;35(5):458-472. doi: 10.1016/j.annonc.2024.01.011. Epub 2024 Feb 27. PMID: 38417742.
- Agarwal N, Azad AA, Carles J, Fay AP, Matsubara N, Szczylik C, De Giorgi U, Young Joung J, Fong PCC, Voog E, Jones RJ, Shore ND, Saad F, Dunshee C, Zschäbitz S, Oldenburg J, Lin X, Healy CG, Kalac M, Kennedy D, Fizazi K. Talazoparib plus enzalutamide in men with metastatic castration-resistant prostate cancer: final overall survival results from the randomised, placebo-controlled, phase 3 TALAPRO-2 trial. Lancet. 2025 Aug 2;406(10502):447-460. doi: 10.1016/S0140-6736(25)00684-1. Epub 2025 Jul 16. PMID: 40683290.
- Saad F, Clarke NW, Oya M, Shore N, Procopio G, Guedes JD, Arslan C, Mehra N, Parnis F, Brown E, Schlürmann F, Joung JY, Sugimoto M, Sartor O, Liu YZ, Poehlein C, Barker L, Del Rosario PM, Armstrong AJ. Olaparib plus abiraterone versus placebo plus abiraterone in metastatic castration-resistant prostate cancer (PROpel): final prespecified overall survival results of a randomised, double-blind, phase 3 trial. Lancet Oncol. 2023 Oct;24(10):1094-1108. doi: 10.1016/S1470-2045(23)00382-0. Epub 2023 Sep 12. Erratum in: Lancet Oncol. 2024 May;25(5):e180. doi: 10.1016/S1470-2045(24)00209-2. PMID: 37714168.
- Attard G, Agarwal N, Graff JN, Sandhu S, Efstathiou E, Özgüroğlu M, Pereira de Santana Gomes AJ, Vianna K, Luo H, Gotto GT, Cheng HH, Kim W, Varela CR, Schaeffer D, Kramer K, Li S, Baron B, Shen F, Mundle SD, McCarthy SA, Olmos D, Chi KN, Rathkopf DE. Niraparib and abiraterone acetate plus prednisone for HRR-deficient metastatic castration-sensitive prostate cancer: a randomized phase 3 trial. Nat Med. 2025 Dec;31(12):4109-4118. doi: 10.1038/s41591-025-03961-8. Epub 2025 Oct 7. PMID: 41057655; PMCID: PMC12705445.
- Agarwal N, Matsubara N, et al. PARP and androgen-signaling inhibition plus ADT in metastatic prostate cancer. N Engl J Med. 2026. doi:10.1056/NEJMoa2604126.