(UroToday.com) The 2026 American Society of Clinical Oncology (ASCO) Annual Meeting was host to State-of-the-Art Session on advances in the perioperative management of bladder and kidney cancers. Dr. Brendan Guercio presented a state-of-the-art review examining the prognostic significance of pCR, the implications of contemporary perioperative immunotherapy-based treatment strategies, the emerging role of circulating tumor DNA (ctDNA), and ongoing efforts to individualize adjuvant therapy and bladder preservation approaches in muscle-invasive bladder cancer (MIBC).
To frame the discussion, Dr. Guercio presented a clinical case of a 68-year-old woman with newly diagnosed cT3N0M0 urothelial carcinoma of the bladder who was cisplatin-ineligible due to a creatinine clearance of 39 mL/min and baseline grade 2 hearing loss. She received three cycles of perioperative enfortumab vedotin plus pembrolizumab (EVP) as per KEYNOTE-905 and subsequently underwent radical cystectomy with pelvic lymph node dissection, achieving ypT0N0 disease (pCR). The central clinical question was whether adjuvant therapy remains necessary after pCR and whether ctDNA can be used to guide treatment de-escalation.
Dr. Guercio began by reviewing the prognostic significance of pCR following neoadjuvant therapy. Data from SWOG 8710 demonstrated that patients achieving pT0 disease after neoadjuvant chemotherapy experienced excellent long-term outcomes, with approximately 85% 5-year overall survival.1 Furthermore, a meta-analysis demonstrated a pooled risk ratio for recurrence-free survival of 0.19 among patients achieving pCR compared to those without pCR, highlighting the strong prognostic value of complete pathologic eradication of disease. As a result, pCR has become a commonly utilized endpoint in signal-seeking phase II studies and has increasingly been incorporated as a co-primary endpoint in phase III perioperative trials. Conversely, residual high-risk disease after neoadjuvant chemotherapy, such as ypT2 disease or node-positive disease, remains an indication for adjuvant treatment.
The therapeutic landscape of perioperative MIBC has evolved rapidly over the last several years. Dr. Guercio emphasized that current treatment paradigms are increasingly defined by cisplatin eligibility and the incorporation of perioperative immunotherapy-based “sandwich” regimens.
For cisplatin-ineligible patients, KEYNOTE-905 established perioperative EVP as a standard treatment approach, consisting of three cycles of preoperative EVP followed by cystectomy and subsequent adjuvant EVP.2 More recently, the phase III VOLGA study reported positive results with preoperative enfortumab vedotin plus perioperative durvalumab with or without tremelimumab, demonstrating improvements in event-free and overall survival compared with cystectomy-based standard approaches.
Among cisplatin-eligible patients, NIAGARA established perioperative durvalumab plus gemcitabine/cisplatin as a new standard of care. At 24 months, overall survival was 82.2% with durvalumab plus chemotherapy versus 75.2% with chemotherapy alone.3 The VESPER study previously demonstrated superior survival outcomes with dose-dense MVAC compared to gemcitabine/cisplatin, albeit at the expense of increased toxicity.4 More recently, KEYNOTE-B15 reported that perioperative EVP improved overall survival compared with neoadjuvant gemcitabine/cisplatin and remains under regulatory review.5
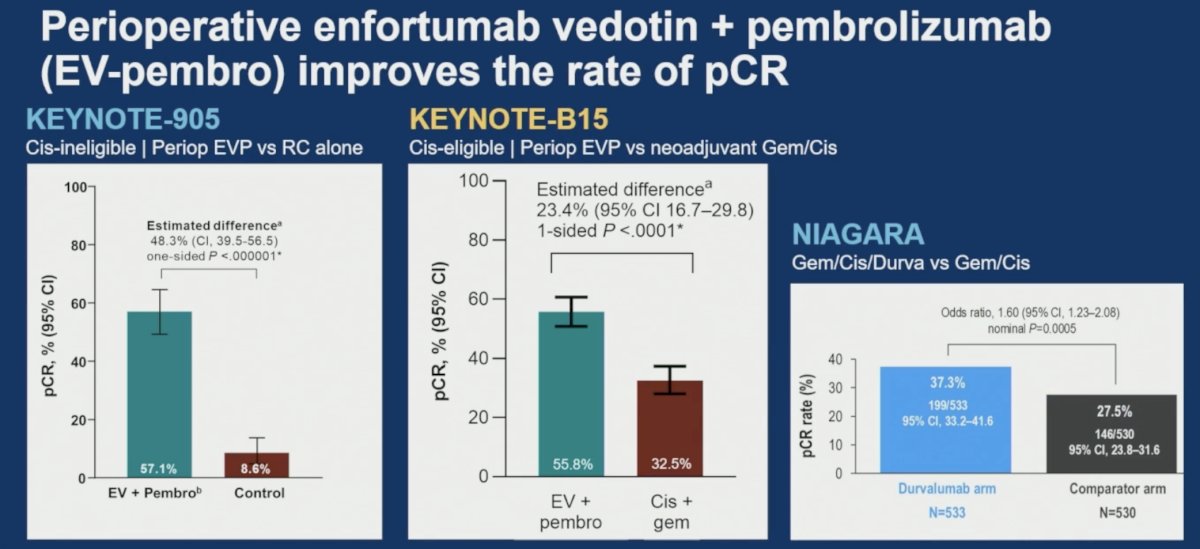
Dr. Guercio highlighted that these contemporary perioperative regimens substantially increase pCR rates. In KEYNOTE-905, perioperative EVP achieved a pCR rate of 57.1% compared with only 8.6% for surgery alone, representing an absolute improvement of 48.3% (95% CI: 39.5–56.5; p<0.00001). Similarly, KEYNOTE-B15 demonstrated a pCR rate of 55.8% with EVP compared to 32.5% with gemcitabine/cisplatin, corresponding to an estimated difference of 23.4% (95% CI: 16.7–29.8; p<0.0001). In NIAGARA, durvalumab plus chemotherapy increased pCR rates to 37.3% compared with 27.5% for chemotherapy alone (OR 1.60, 95% CI: 1.23–2.08; nominal p=0.0005).
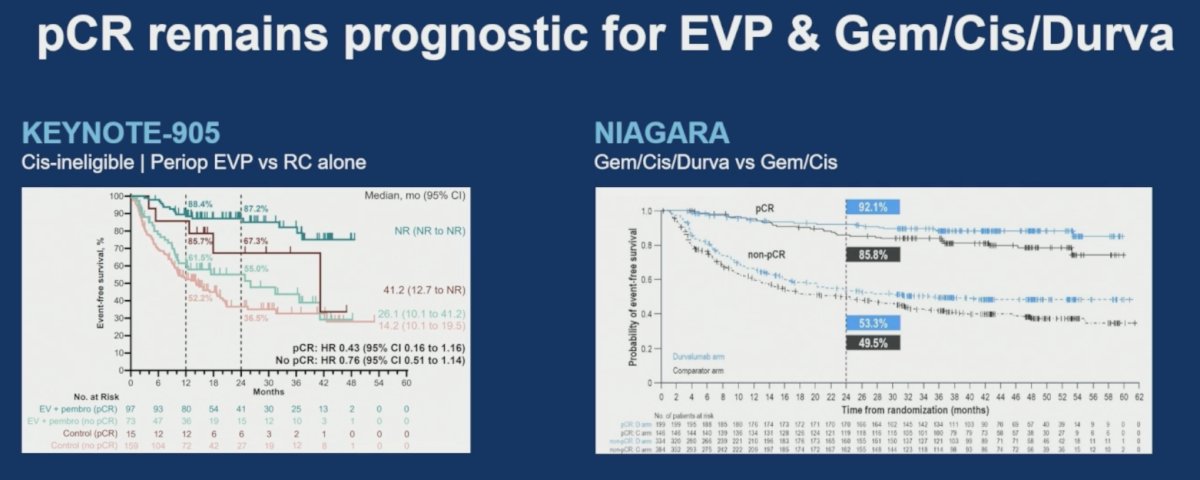
Importantly, pCR continued to demonstrate prognostic significance even in the setting of these newer perioperative immunotherapy-based approaches. In KEYNOTE-905, patients achieving pCR experienced excellent event-free survival outcomes irrespective of treatment arm. Similarly, analyses from NIAGARA demonstrated markedly improved outcomes among patients achieving pCR compared with those without pCR, supporting the continued clinical relevance of pathologic response despite advances in systemic therapy.
A critical question addressed during the presentation was whether patients who achieve pCR after perioperative immunotherapy can safely omit the planned adjuvant component of treatment. Dr. Guercio emphasized that current evidence does not support this strategy. In contemporary perioperative “sandwich” regimens, the standard approach remains completion of the planned postoperative treatment regardless of pathologic response.
Specifically, patients treated according to the NIAGARA regimen should resume durvalumab for an additional eight months following cystectomy, while patients treated with perioperative EVP should continue the planned postoperative EVP component. In contrast, among patients receiving neoadjuvant cisplatin-based chemotherapy alone, surveillance following pCR remains standard practice. Important unanswered questions remain regarding the relative contributions of preoperative versus postoperative therapy and whether biomarkers such as pCR or ctDNA can safely guide treatment de-escalation.
The latter portion of the presentation focused on the rapidly evolving field of ctDNA. Dr. Guercio reviewed data from the IMvigor011 study,6 which established the prognostic importance of postoperative ctDNA assessment. Patients with detectable ctDNA following cystectomy experienced substantially higher recurrence risk and appeared to derive benefit from adjuvant atezolizumab, with a disease-free survival hazard ratio of 0.62. Conversely, patients with persistently negative ctDNA demonstrated favorable outcomes without adjuvant therapy, achieving approximately 88% 2-year disease-free survival.
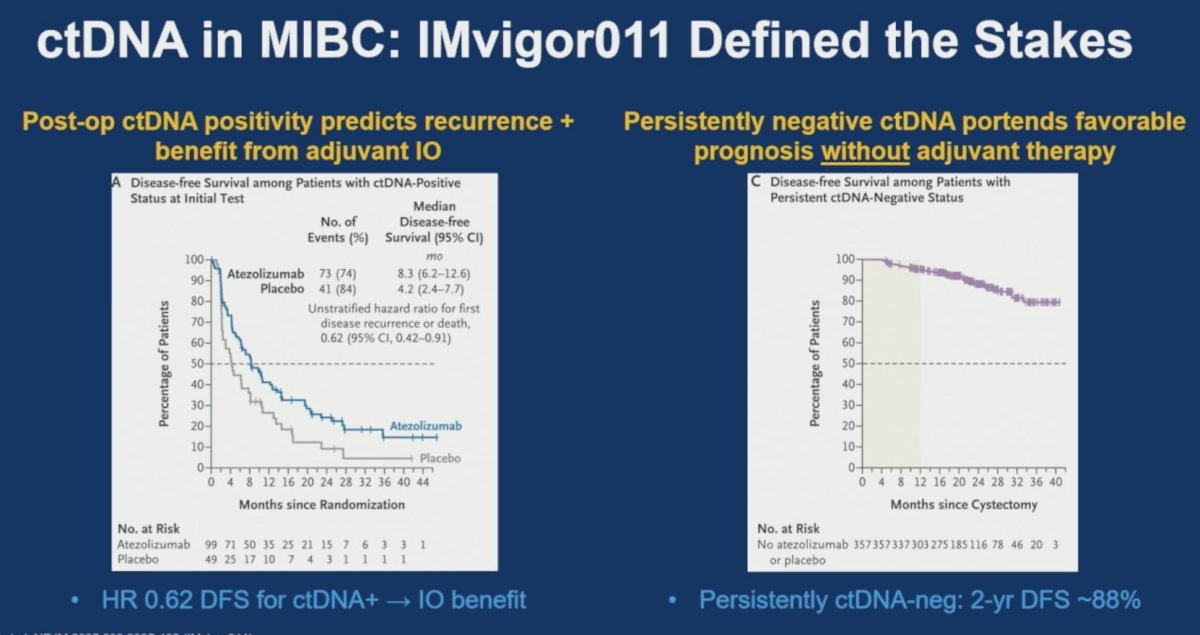
Despite these promising findings, Dr. Guercio cautioned against overinterpreting ctDNA-negative results in the modern perioperative immunotherapy era. IMvigor011 excluded patients achieving pCR and largely enrolled patients who had not received preoperative immunotherapy. Furthermore, approximately 11% of ctDNA-negative patients still experienced recurrence or death, underscoring that negative ctDNA does not guarantee cure. Consequently, while IMvigor011 provided valuable insight into when adjuvant immunotherapy should be initiated, it did not establish when immunotherapy can safely be stopped.
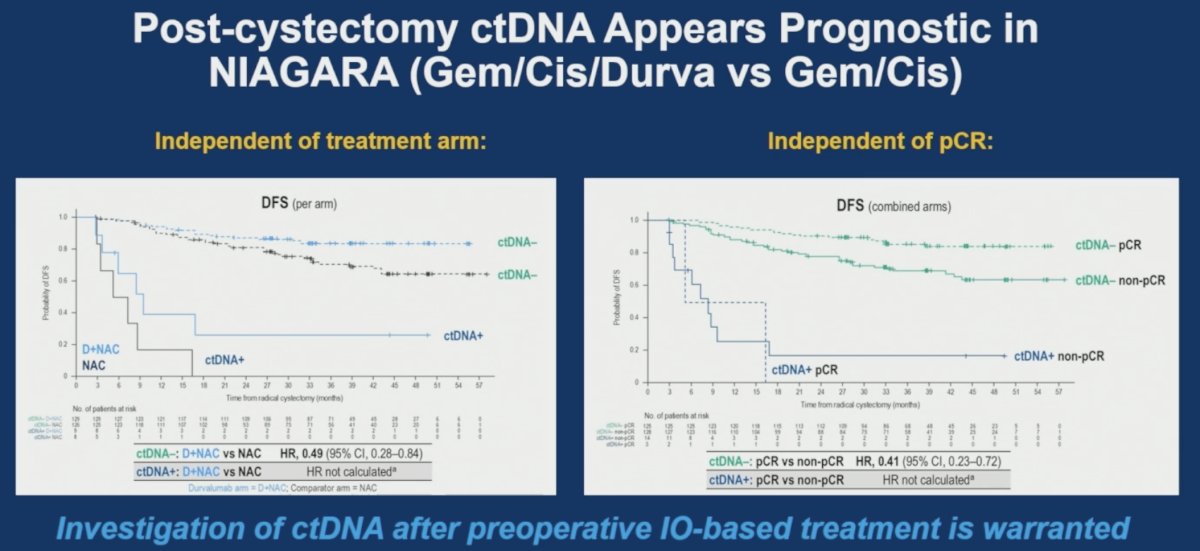
Emerging analyses from NIAGARA suggest that ctDNA retains prognostic value even following perioperative immunotherapy-based treatment. Post-cystectomy ctDNA negativity was associated with favorable disease-free survival irrespective of treatment arm and independent of pCR status. These findings support continued investigation of ctDNA as a biomarker in patients receiving contemporary perioperative immunotherapy regimens.
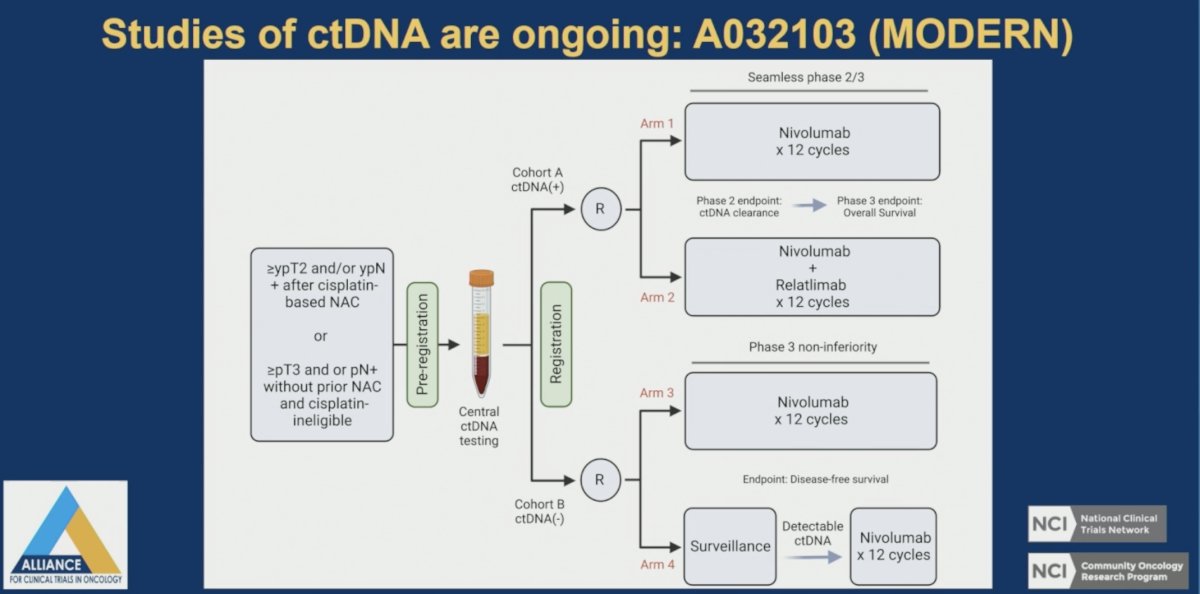
To address these unanswered questions, Dr. Guercio highlighted the ongoing Alliance A032103 (MODERN) trial. This adaptive study stratifies patients according to postoperative ctDNA status. Patients with detectable ctDNA are randomized to nivolumab alone versus nivolumab plus relatlimab, while ctDNA-negative patients are randomized to nivolumab versus surveillance. The study aims to determine whether ctDNA-guided treatment intensification and de-escalation strategies can improve outcomes while reducing overtreatment.
The presentation concluded with a discussion of bladder preservation strategies in patients achieving clinical complete response (cCR). As pCR rates exceed 50% with EVP-based therapy, increasing attention has focused on identifying patients who may safely avoid cystectomy. However, Dr. Guercio noted that conventional cCR assessment using cystoscopy, cytology, and imaging remains imperfect and may misclassify residual MIBC in up to one-quarter of patients. Emerging biomarkers, including ctDNA and urinary tumor DNA (utDNA), may improve prediction of pCR and enhance patient selection for bladder-sparing approaches, although further validation is needed.
Several ongoing studies are evaluating bladder preservation strategies after cCR, including HCRN GU16-257, RETAIN-1, RETAIN-2, EV-209, HCRN GU22-598, EV-309, and SURE-02. Additional studies investigating bladder preservation through radiation-based approaches include BRIGHT (S2427), EV-PRIME, and ARCHER (NRG-GU015).
Returning to the original clinical case, Dr. Guercio concluded that a cisplatin-ineligible patient achieving ypT0N0 disease after perioperative EVP should continue the planned adjuvant EVP component according to the KEYNOTE-905 treatment paradigm. Although serial ctDNA assessment may provide valuable prognostic information, it has not yet been validated as a tool to safely de-escalate adjuvant therapy.
Dr. Guercio closed with three key takeaways:
- First, pCR following neoadjuvant therapy remains a powerful positive prognostic marker in MIBC.
- Second, surveillance remains standard following pCR achieved with neoadjuvant chemotherapy alone, whereas completion of planned adjuvant therapy remains the standard after perioperative immunotherapy-based “sandwich” regimens.
- Third, although pCR and ctDNA hold significant promise as tools to guide treatment de-escalation, their use for this purpose remains investigational and should currently be restricted to clinical trials.
Presented by: Brendan J. Guercio, MD, Assistant Professor, Department of Medicine, University of Rochester, Rochester, NY, USA
Written by: Rashid K. Sayyid, MD, MSc, Assistant Professor, Urologic Oncologist, Department of Urology at The University of Arizona and Banner University Medical Center, Tucson, AZ – @rksayyid on X during the American Society of Clinical Oncology Genitourinary (ASCO) Annual Meeting held in Chicago, IL between May 29th and June 1st, 2026
Related content: Pathologic Complete Response and Bladder Sparing After Perioperative Systemic Therapy - Brendan Guercio
References:
- Grossman HB, Natale RB, Tangen CM, Speights VO, Vogelzang NJ, Trump DL, et al. Neoadjuvant chemotherapy plus cystectomy compared with cystectomy alone for locally advanced bladder cancer. N Engl J Med. 2003;349(9):859-866.
- Vulsteke C, Adra N, Danchaivijitr P, Sabadash M, Rodriguez-Vida A, Zhang Z, et al. Perioperative enfortumab vedotin and pembrolizumab in bladder cancer. N Engl J Med. 2026;394(13):1257-1269.
- Powles T, Catto JWF, Galsky MD, Al-Ahmadie H, Meeks JJ, Nishiyama H, et al. Perioperative durvalumab with neoadjuvant chemotherapy in operable bladder cancer. N Engl J Med. 2024;391:1773-1786.
- Pfister C, Gravis G, Flechon A, Chevreau C, Mahammedi H, Laguerre B, et al. Perioperative dose-dense methotrexate, vinblastine, doxorubicin, and cisplatin in muscle-invasive bladder cancer (VESPER): survival endpoints at 5 years in an open-label, randomised, phase 3 study. Lancet Oncol. 2024;25(2):255-264.
- Galsky MD, Valderrama BP, Maruzzo M, Font Pous A, Ciuleanu TE, Chatzkel JA, et al. Neoadjuvant and adjuvant enfortumab vedotin plus pembrolizumab for participants with muscle-invasive bladder cancer who are eligible for cisplatin: randomized, open-label, phase 3 KEYNOTE-B15 study. J Clin Oncol. 2026;44(Suppl 5):Abstract 661.
- Powles T, Kann AG, Castellano D, Gross-Goupil M, Nishiyama H, Bracarda S, et al. ctDNA-guided adjuvant atezolizumab in muscle-invasive bladder cancer. N Engl J Med. 2025;393(24):2395-2408.