(UroToday.com) The 2026 American Society of Clinical Oncology Genitourinary (ASCO) Annual Meeting held in Chicago, IL, was host to the Prostate, Testicular, and Penile Cancer - Oral Abstracts. Dr. Neeraj Agarwal presented Abstract LBA5007: TALAPRO-3: Talazoparib + enzalutamide compared with placebo + enzalutamide for the treatment of patients with mCSPC harboring HRR gene alterations.
Dr. Agarwal began by highlighting prior data supporting combined PARP and androgen receptor pathway inhibition strategies in advanced prostate cancer.1,2 He noted that in the phase III TALAPRO-2 trial, the addition of talazoparib to enzalutamide significantly prolonged radiographic progression-free survival and overall survival in patients with metastatic castration-resistant prostate cancer, with the greatest benefit observed among patients harboring homologous recombination repair gene alterations.1
He further referenced the BRCAway study led by Dr. Hussain, which demonstrated that combination therapy with a PARP inhibitor plus an ARPI was more effective than either agent alone or sequential treatment approaches in patients with HRR gene-altered metastatic castration-resistant prostate cancer.3 Despite contemporary treatment intensification with ADT plus ARPIs in metastatic castration-sensitive prostate cancer, Dr. Agarwal emphasized that outcomes among patients with HRR gene alterations remain suboptimal, highlighting a persistent unmet clinical need for improved treatment strategies earlier in the disease course. Based on these observations, investigators hypothesized that the combination of talazoparib plus enzalutamide could improve efficacy compared with enzalutamide alone in men with HRR gene-altered metastatic castration-sensitive prostate cancer receiving ADT.
TALAPRO-3 is a randomized phase III trial evaluating talazoparib plus enzalutamide versus placebo plus enzalutamide in patients with homologous recombination repair gene-altered metastatic castration-sensitive prostate cancer receiving ADT. Eligible patients were required to have HRR gene alterations, ECOG performance status 0–1, radiographically confirmed metastatic disease by bone scan, CT, or MRI, and could have received up to 3 months of prior ADT with or without an ARPI for mCSPC. Prior docetaxel for mCSPC was not permitted. A total of 599 patients were randomized in a 1:1 fashion to receive talazoparib 0.5 mg plus enzalutamide 160 mg daily or placebo plus enzalutamide 160 mg daily, both on a background of ADT. Stratification factors included de novo versus relapsed metastatic disease, high- versus low-volume disease, and BRCA-mutated versus non-BRCA HRR-altered disease. The study design is shown below:
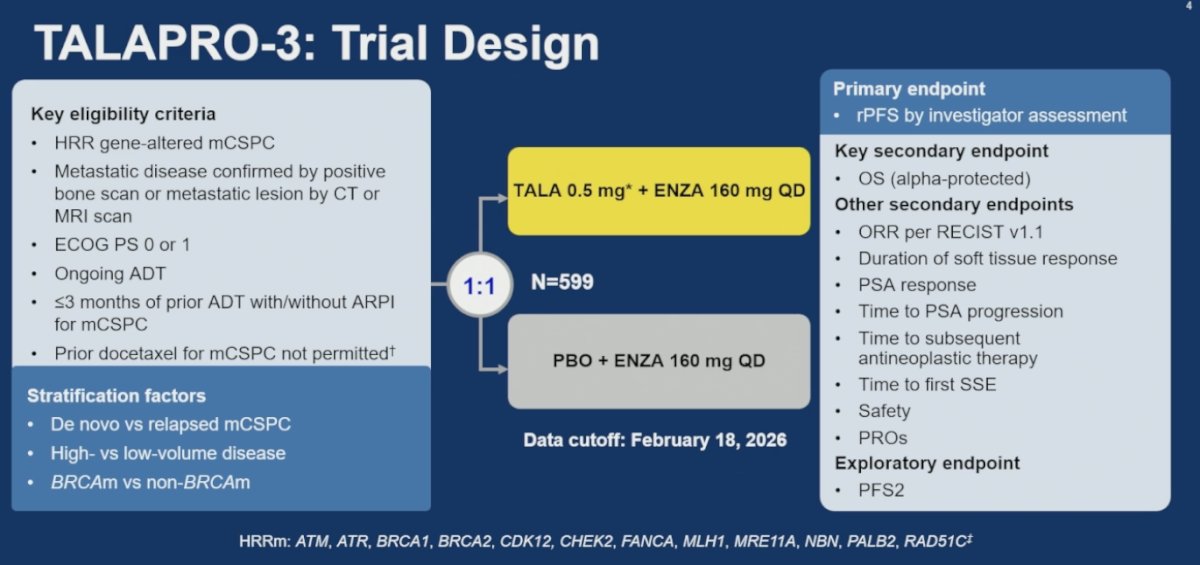
The primary endpoint was investigator-assessed radiographic progression-free survival. Overall survival was the key alpha-protected secondary endpoint. Additional secondary endpoints included objective response rate by RECIST v1.1, duration of soft tissue response, PSA response, time to PSA progression, time to subsequent antineoplastic therapy, time to first symptomatic skeletal event, safety, and patient-reported outcomes. PFS2 was included as an exploratory endpoint.
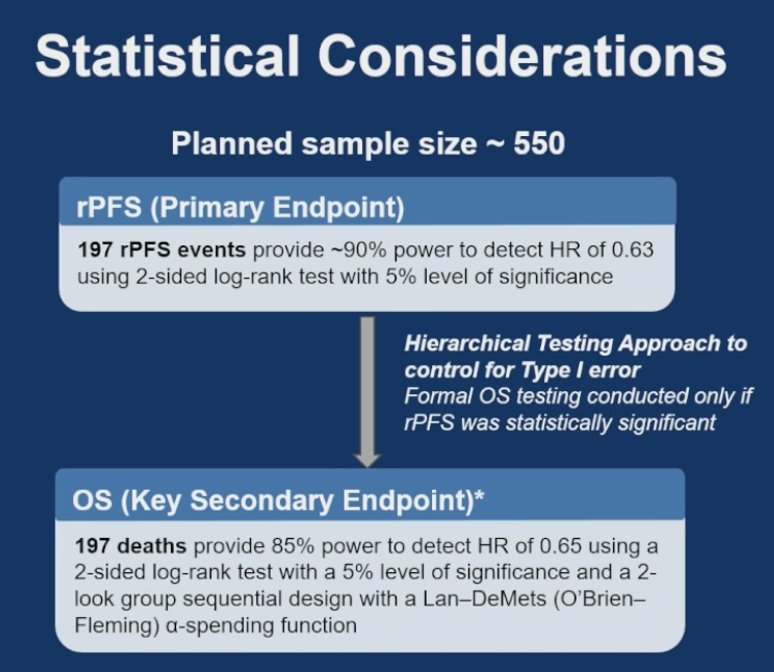
Statistical analyses for TALAPRO-3 were performed in the intention-to-treat population, with efficacy comparing talazoparib plus enzalutamide versus placebo plus enzalutamide in all randomized patients. The study planned to enroll approximately 550 patients, with 197 radiographic progression-free survival events providing approximately 90% power to detect a hazard ratio of 0.63 using a two-sided log-rank test with a 5% significance level. Importantly, the study utilized a hierarchical testing strategy to control for type I error, meaning overall survival, the key secondary endpoint, would only be formally tested if the primary radiographic progression-free survival endpoint was statistically significant. For overall survival, 197 deaths were estimated to provide 85% power to detect a hazard ratio of 0.65. Kaplan-Meier methods were used for time-to-event analyses, while Cox proportional hazards models estimated hazard ratios and associated 95% confidence intervals.
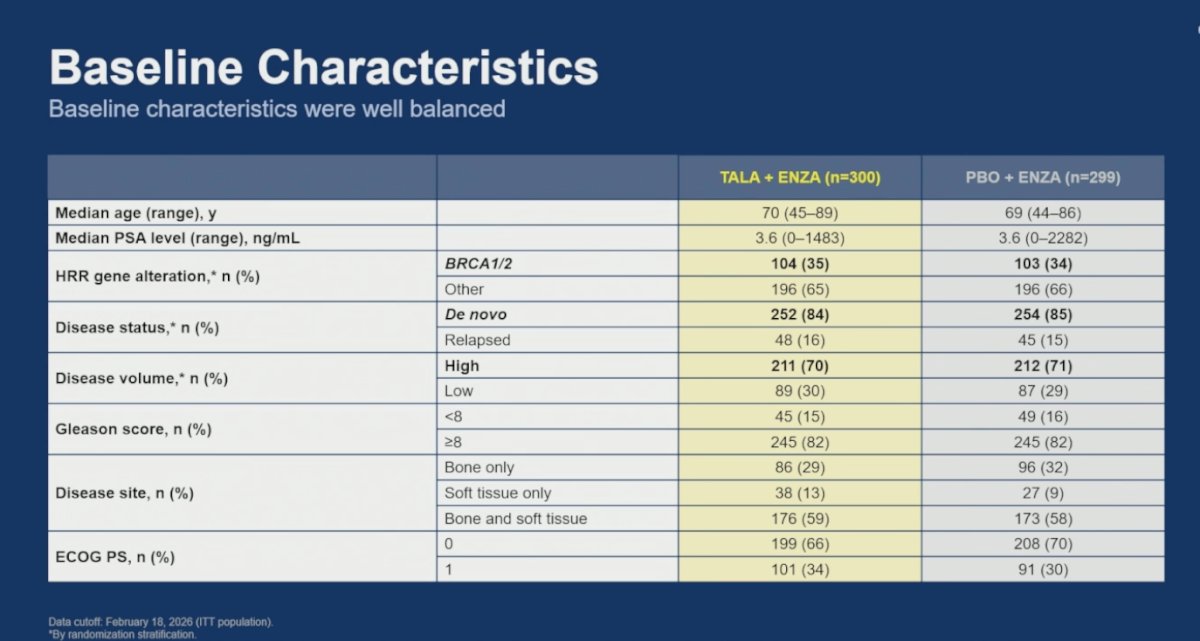
Baseline characteristics were overall well balanced between treatment arms. In the talazoparib plus enzalutamide arm, the median age was 70 years compared with 69 years in the placebo plus enzalutamide arm, and median PSA levels were identical at 3.6 ng/mL in both groups. BRCA1/2 alterations were present in approximately one-third of patients (35% versus 34%), while the majority of patients harbored non-BRCA HRR alterations. Most patients presented with de novo metastatic disease (84% versus 85%) and high-volume disease (70% versus 71%). Gleason score ≥8 was observed in 82% of patients in both treatment arms. Regarding metastatic distribution, combined bone and soft tissue disease was the most common presentation, occurring in 59% and 58% of patients, respectively, while ECOG performance status was also well balanced between groups.
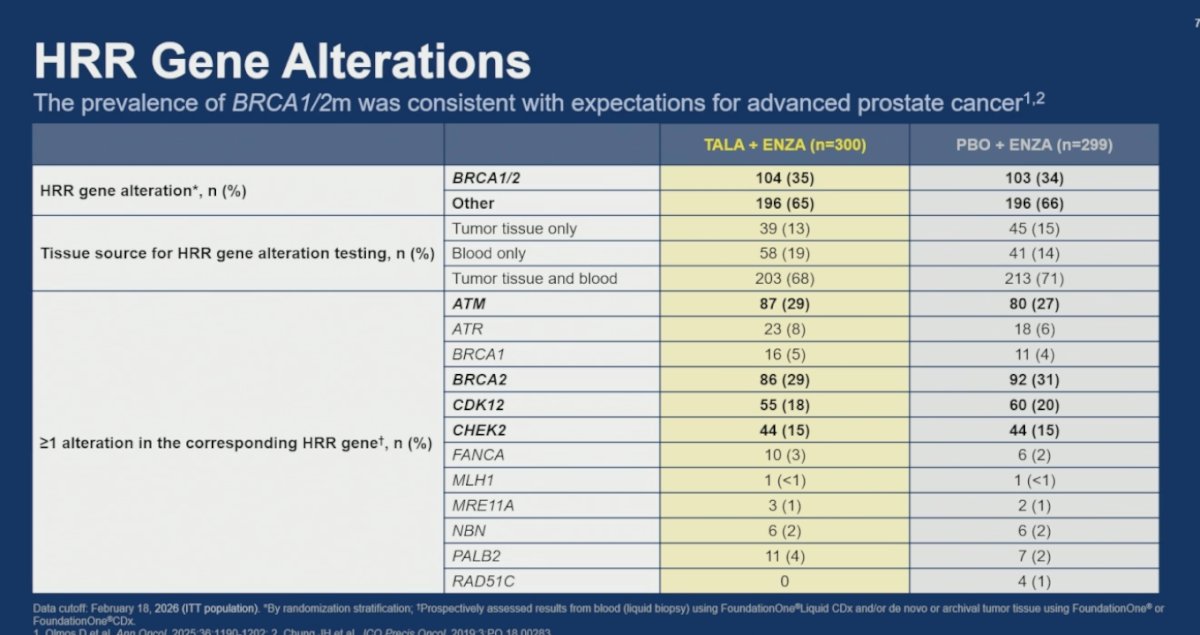
Dr. Agarwal also reviewed the distribution of homologous recombination repair gene alterations across the study population. Beyond BRCA1/2 alterations, ATM mutations were among the most common non-BRCA alterations, observed in 29% of patients treated with talazoparib plus enzalutamide and 27% of those receiving placebo plus enzalutamide. CDK12 alterations were identified in 18% and 20% of patients, respectively, while CHEK2 alterations were present in 15% of patients in both treatment arms.
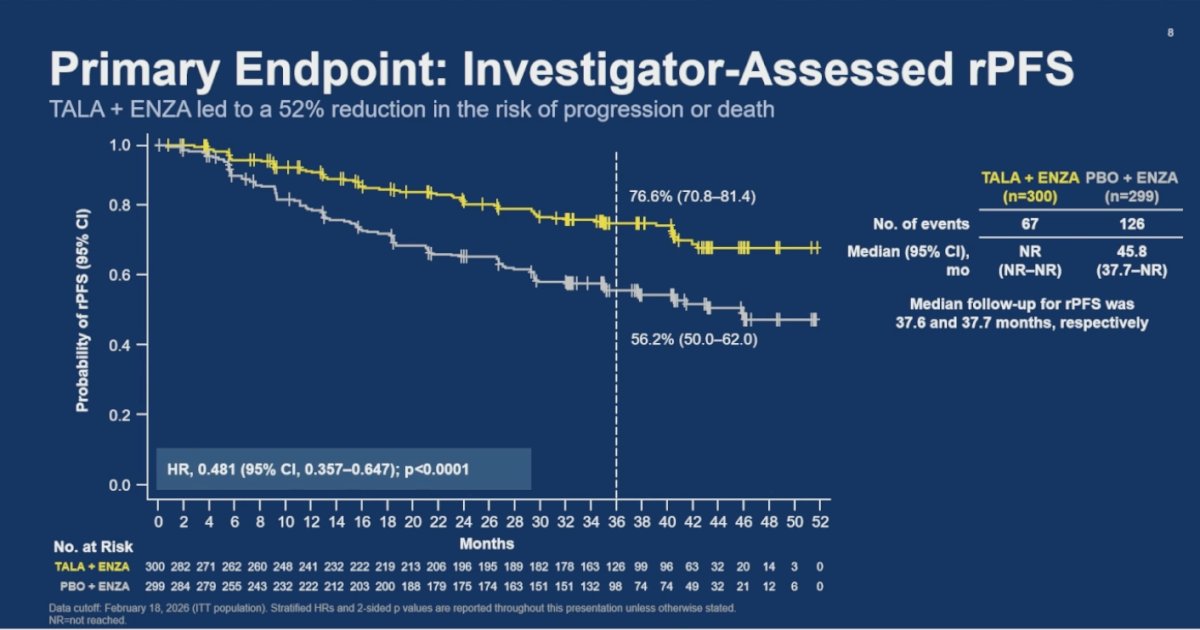
The primary endpoint of investigator-assessed radiographic progression-free survival was met, with talazoparib plus enzalutamide demonstrating a significant reduction in the risk of radiographic progression or death compared with placebo plus enzalutamide. Median radiographic progression-free survival was not reached in the talazoparib-containing arm versus 45.8 months in the control arm, corresponding to a hazard ratio of 0.481 (95% CI 0.357–0.647; p<0.0001). At approximately 36 months, radiographic progression-free survival rates were 76.6% in the talazoparib plus enzalutamide arm compared with 56.2% in the placebo plus enzalutamide arm, clearly favoring the combination strategy.
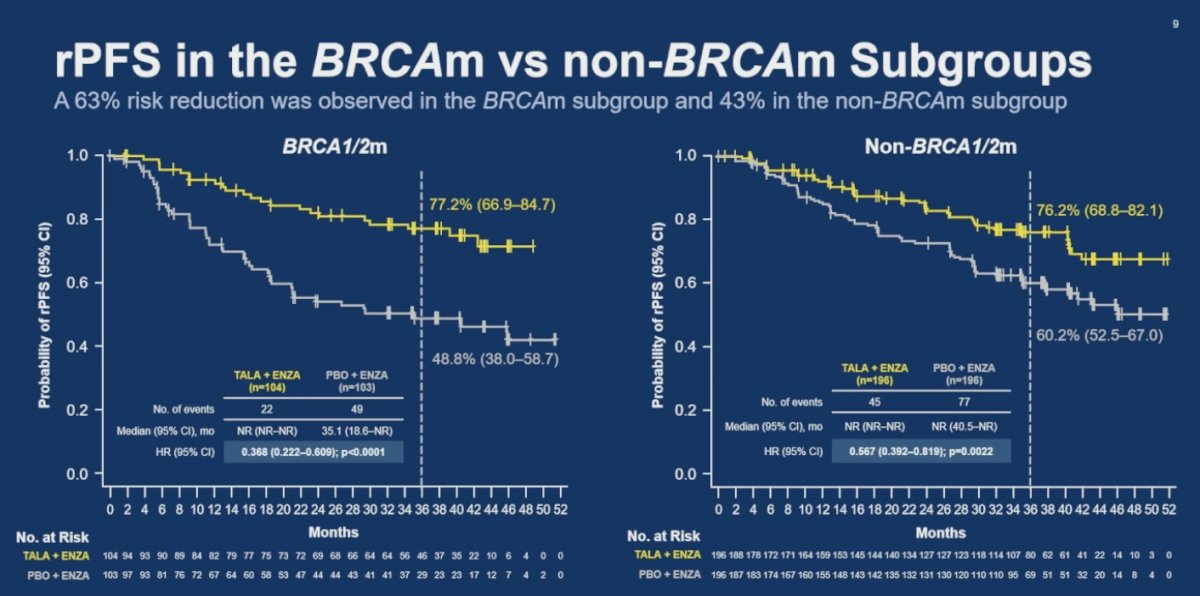
In subgroup analyses, the combination of talazoparib plus enzalutamide favored radiographic progression-free survival across both BRCA-mutated and non-BRCA HRR-altered populations. Among patients with BRCA1/2 alterations, the combination was associated with a 63% reduction in the risk of progression or death (HR 0.368; 95% CI 0.222–0.609; p<0.0001). Importantly, benefit was also observed in the non-BRCA1/2 subgroup, where talazoparib plus enzalutamide reduced the risk of progression or death by 43% compared with placebo plus enzalutamide (HR 0.567; 95% CI 0.392–0.819; p=0.0022).
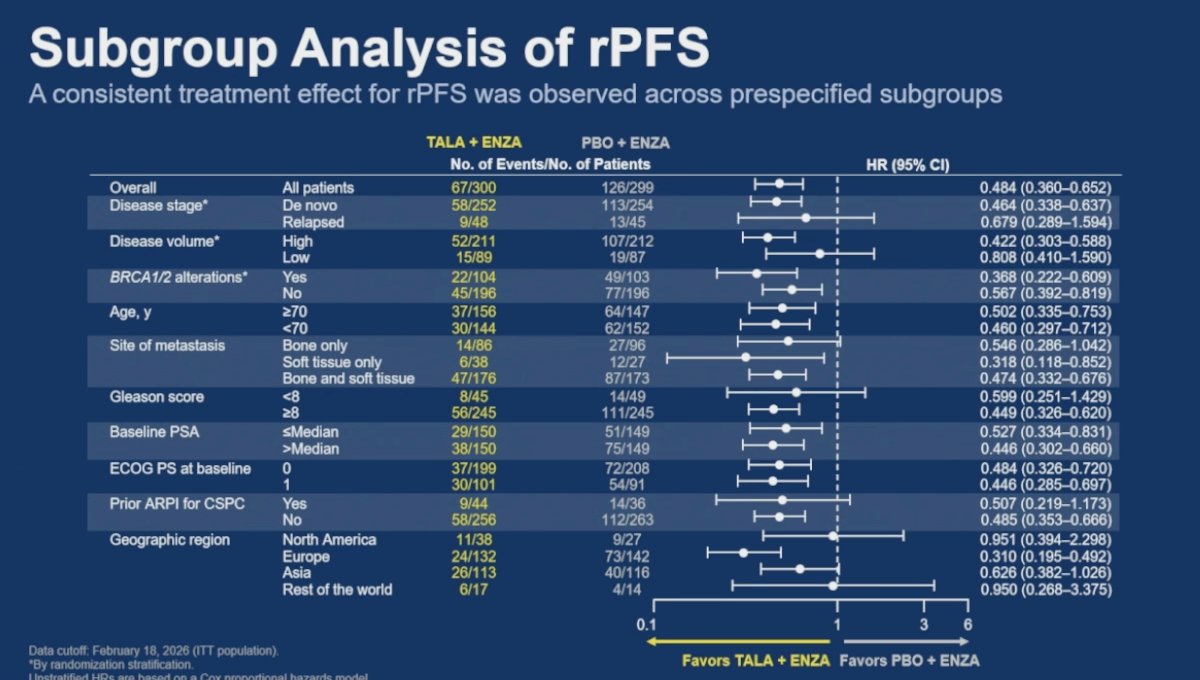
Subgroup analyses demonstrated a consistent radiographic progression-free survival benefit favoring talazoparib plus enzalutamide across nearly all prespecified patient populations. Benefit was observed regardless of disease stage, disease volume, BRCA alteration status, age, Gleason score, baseline PSA, ECOG performance status, prior ARPI exposure for castration-sensitive prostate cancer, and metastatic disease site. The most pronounced benefit continued to be observed among patients harboring BRCA1/2 alterations (HR 0.368), although a clinically meaningful benefit was also maintained in patients without BRCA alterations (HR 0.567). Notably, patients with high-volume disease demonstrated substantial benefit with the combination strategy (HR 0.422), while outcomes consistently favored talazoparib plus enzalutamide across most geographic regions and metastatic patterns.
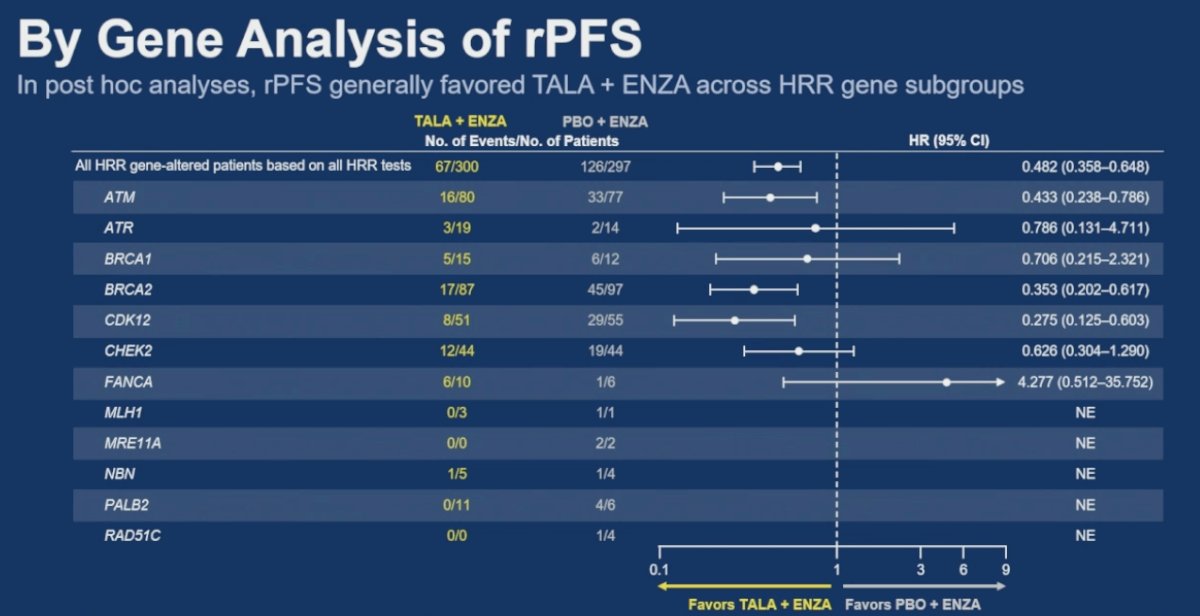
An interesting exploratory post hoc analysis evaluated radiographic progression-free survival according to individual HRR gene alterations. Dr. Agarwal highlighted that clinically meaningful benefit with talazoparib plus enzalutamide appeared particularly notable among patients harboring ATM alterations (HR 0.433), BRCA2 alterations (HR 0.353), and CDK12 alterations (HR 0.275). While several additional HRR subgroups numerically favored the talazoparib-containing combination, many of these analyses were limited by small patient numbers and wide confidence intervals, and therefore should be interpreted cautiously.
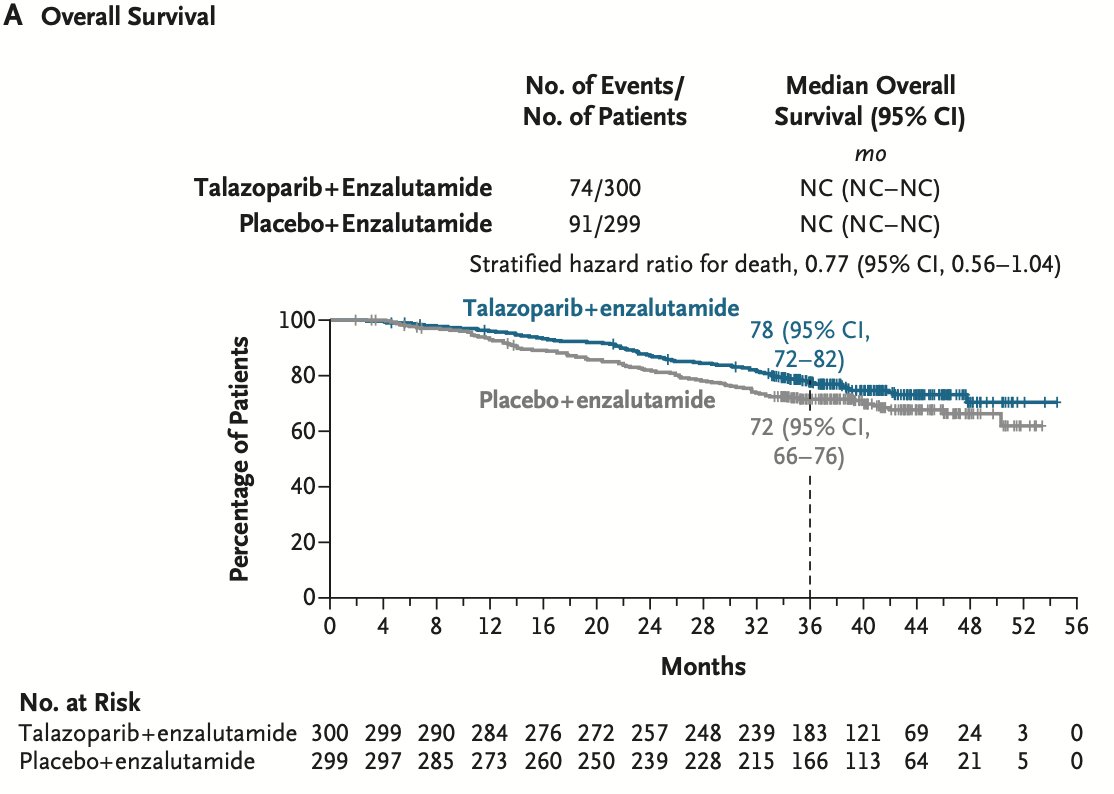
Overall survival data remain immature at the current analysis. Median overall survival was not reached in either treatment arm, although a numerical trend favoring talazoparib plus enzalutamide was observed, with a stratified hazard ratio for death of 0.77 (95% CI 0.56–1.04). At approximately 36 months, overall survival rates were 78% in the talazoparib plus enzalutamide arm compared with 72% in the placebo plus enzalutamide arm.
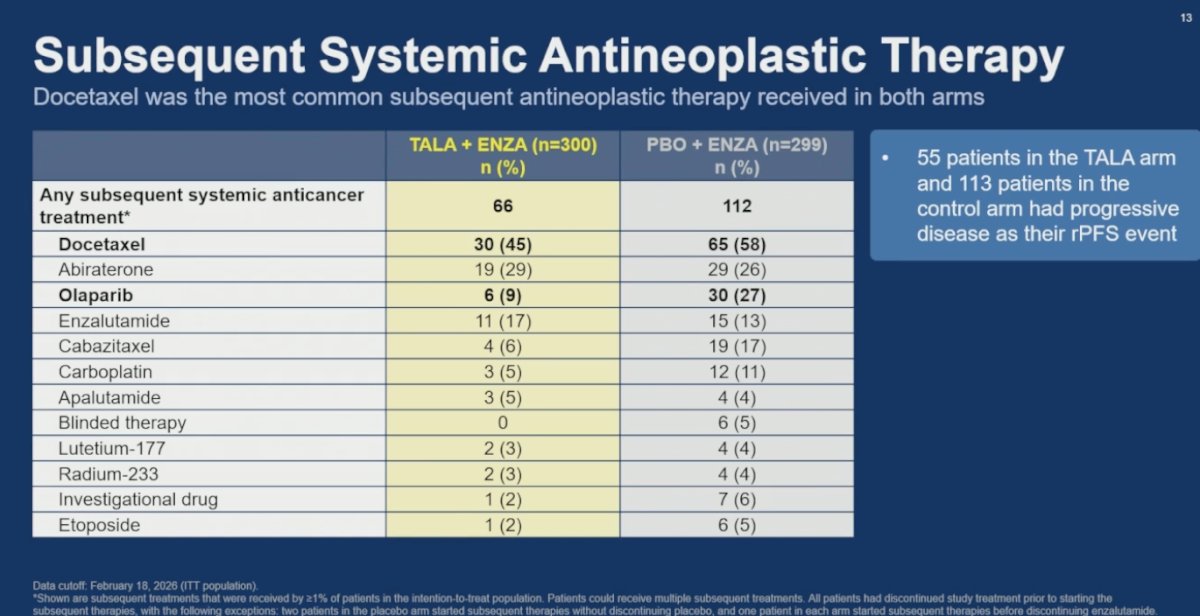
Dr. Agarwal also reviewed subsequent systemic antineoplastic therapies received after progression. Fewer patients in the talazoparib plus enzalutamide arm required subsequent anticancer treatment compared with the control arm (66 versus 112 patients). Docetaxel was the most common subsequent therapy in both groups, administered to 45% of patients in the talazoparib arm and 58% in the placebo plus enzalutamide arm. Notably, subsequent olaparib use was substantially lower among patients previously treated with talazoparib plus enzalutamide (9% versus 27%). Additionally, 55 patients in the talazoparib arm and 113 patients in the control arm experienced progressive disease as their radiographic progression-free survival event.
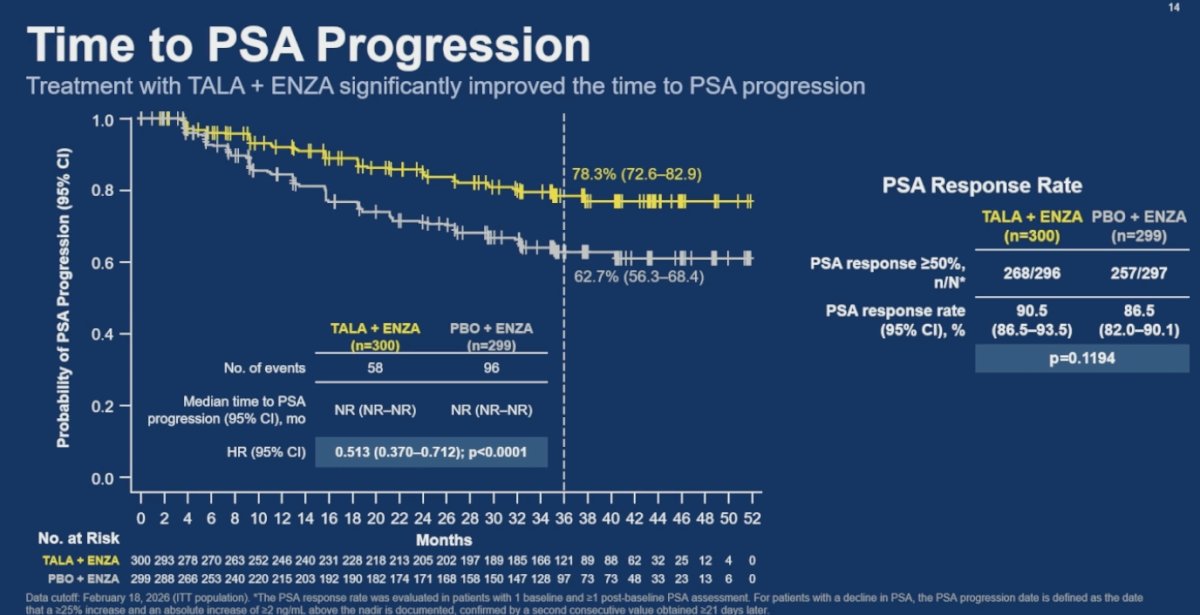
Treatment with talazoparib plus enzalutamide significantly improved time to PSA progression compared with placebo plus enzalutamide (HR 0.513; 95% CI 0.370–0.712; p<0.0001). PSA response rates ≥50% were high in both treatment arms, with no statistically significant difference observed (90.5% versus 86.5%; p=0.1194).
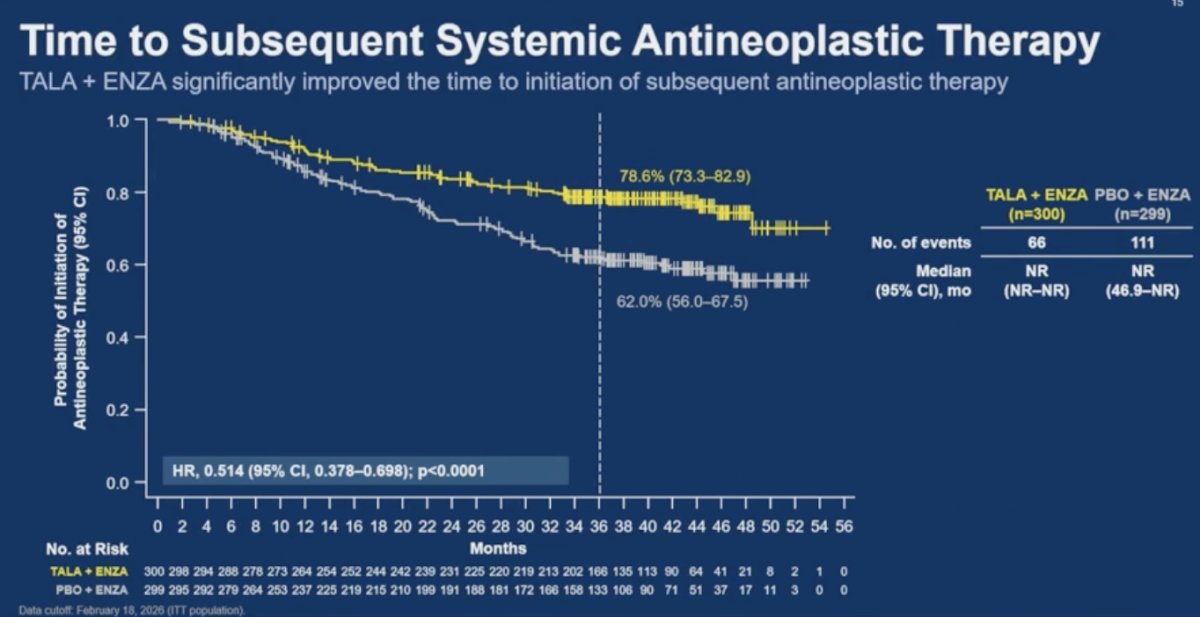
Talazoparib plus enzalutamide significantly delayed the initiation of subsequent systemic antineoplastic therapy compared with placebo plus enzalutamide (HR 0.514; 95% CI 0.378–0.698; p<0.0001).
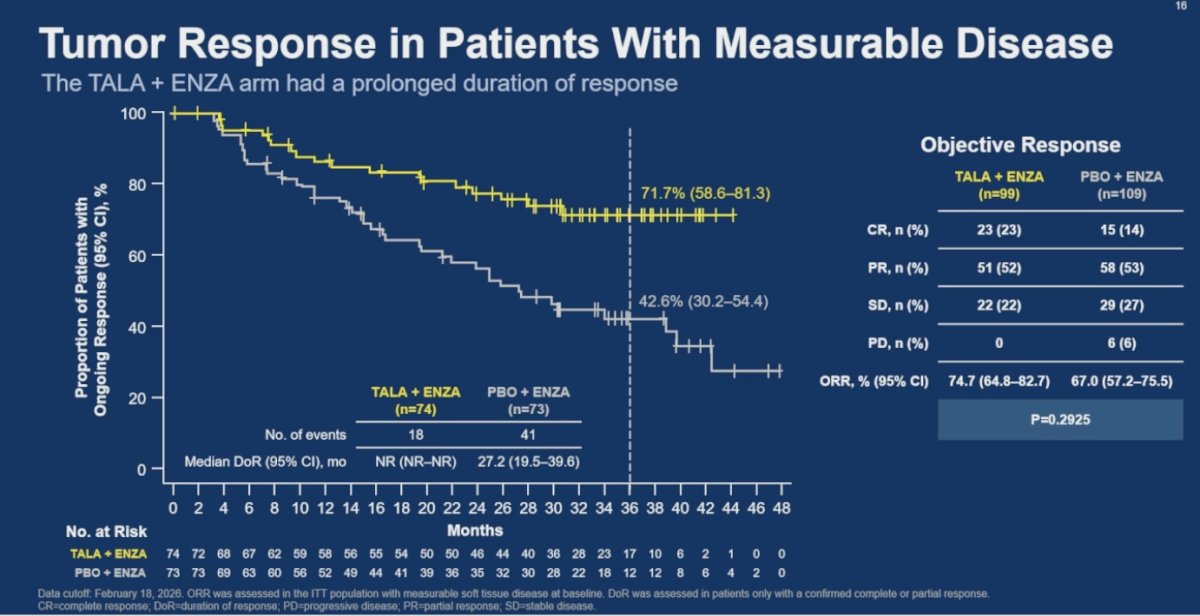
Moreover, among patients with measurable disease at baseline, talazoparib plus enzalutamide was associated with a more prolonged duration of response compared with placebo plus enzalutamide. Median duration of response was not reached in the combination arm versus 27.2 months in the control arm, while objective response rates were numerically higher with talazoparib plus enzalutamide (74.7% versus 67.0%), although this difference was not statistically significant (p=0.2925).
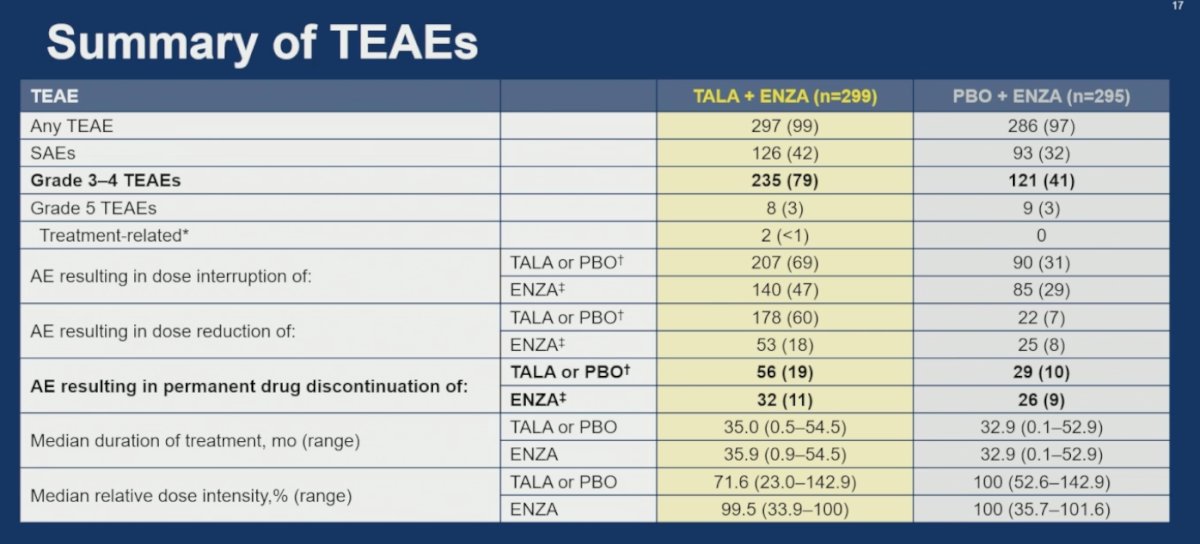
Grade 3–4 treatment-emergent adverse events occurred in 79% of patients treated with talazoparib plus enzalutamide compared with 41% in the placebo plus enzalutamide arm. Despite the higher rate of high-grade toxicities, relatively few patients required permanent treatment discontinuation, occurring in 19% versus 10% for talazoparib/placebo and 11% versus 9% for enzalutamide, respectively.
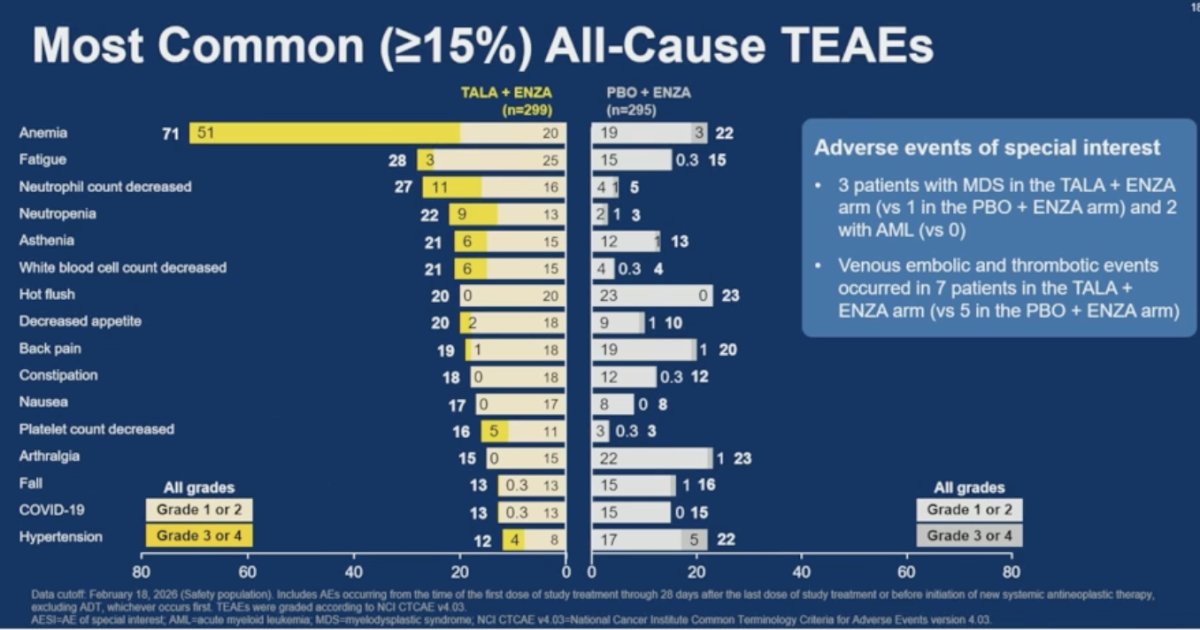
The most common treatment-emergent adverse events in the talazoparib plus enzalutamide arm were anemia, fatigue, neutrophil count decrease, neutropenia, asthenia, and decreased white blood cell count. Anemia was particularly frequent, occurring in 71% of patients in the combination arm compared with 22% in the control arm. Dr. Agarwal also highlighted adverse events of special interest, including myelodysplastic syndrome, which occurred in 3 patients treated with talazoparib plus enzalutamide versus 1 patient in the placebo plus enzalutamide arm, as well as acute myeloid leukemia, observed in 2 patients in the talazoparib-containing arm and none in the control group. Additionally, venous embolic and thrombotic events occurred in 7 patients receiving talazoparib plus enzalutamide compared with 5 patients treated with placebo plus enzalutamide.
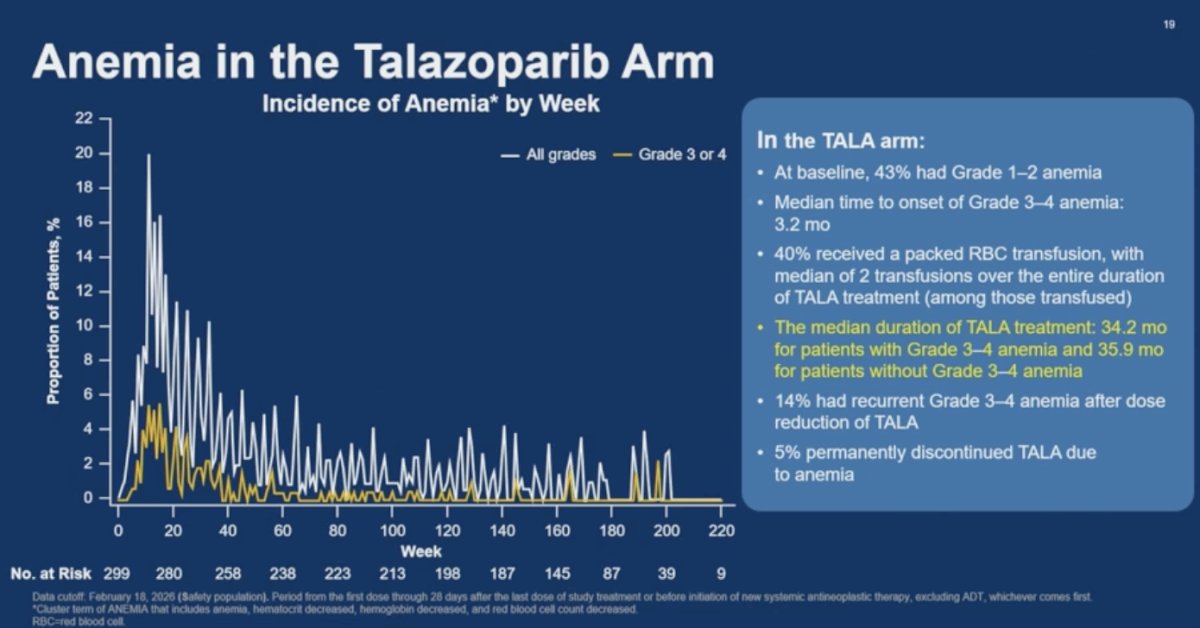
Because anemia was the most common adverse event observed with talazoparib plus enzalutamide, Dr. Agarwal spent additional time reviewing the anemia profile in the combination arm. At baseline, 43% of patients already had grade 1–2 anemia, while the median time to onset of grade 3–4 anemia was 3.2 months. Forty percent of patients required packed red blood cell transfusions, with a median of 2 transfusions among transfused patients over the course of treatment.
Importantly, the protocol mandated talazoparib dose reductions in the setting of grade 3–4 anemia. Despite these events, the median duration of talazoparib treatment remained similar between patients who developed grade 3–4 anemia and those who did not, at 34.2 months versus 35.9 months, respectively. Recurrent grade 3–4 anemia after talazoparib dose reduction occurred in 14% of patients, while only 5% of patients permanently discontinued talazoparib due to anemia.
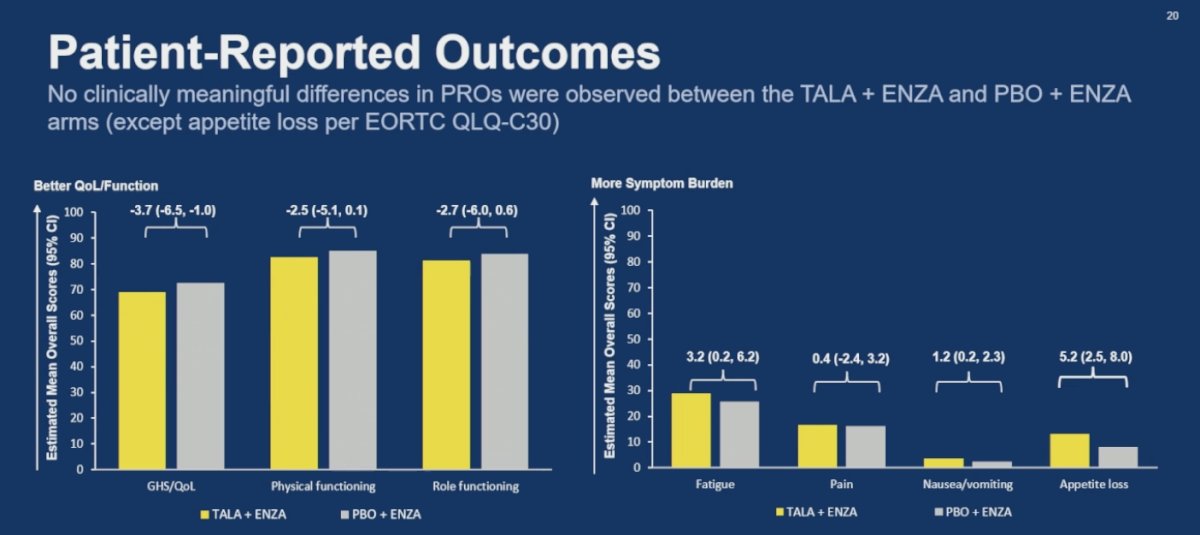
Patient-reported outcomes were generally similar between treatment arms, with no clinically meaningful differences observed between talazoparib plus enzalutamide and placebo plus enzalutamide across global quality of life, physical functioning, role functioning, fatigue, pain, or nausea/vomiting domains. The only notable difference was a higher appetite loss symptom burden observed in the talazoparib-containing arm according to EORTC QLQ-C30 assessments.
Dr Agarwal concluded his presentation with the following key takeaways:
- TALAPRO-3 demonstrated a clinically meaningful and statistically significant improvement in radiographic progression-free survival with talazoparib plus enzalutamide compared with enzalutamide alone in patients with HRR gene-altered metastatic castration-sensitive prostate cancer (HR 0.48).
- Radiographic progression-free survival benefit was consistent across clinical subgroups, including both BRCA-mutated (HR 0.37) and non-BRCA-mutated (HR 0.57) populations.
- Interim overall survival analyses numerically favored the talazoparib plus enzalutamide combination, although overall survival data remain immature.
- Improvements in time to PSA progression and time to subsequent systemic antineoplastic therapy were directionally consistent with the primary radiographic progression-free survival findings.
- The most common adverse events with the combination strategy were hematologic toxicities, particularly anemia and neutrophil count decrease, as well as fatigue.
- Treatment-emergent adverse events were generally manageable with dose modifications and supportive care measures, and the median duration of talazoparib treatment was similar regardless of whether patients developed grade 3–4 anemia.
- Permanent discontinuation of talazoparib due to anemia occurred in only 5% of patients.
- Addition of talazoparib to enzalutamide did not result in clinically meaningful deterioration in patient-reported outcomes compared with enzalutamide alone.
- These results support talazoparib plus enzalutamide as a potential treatment option for patients with HRR gene-altered metastatic castration-sensitive prostate cancer and further underscore the critical importance of early molecular testing in prostate cancer.
- These data were concurrently published in the New England Journal of Medicine (DOI: 10.1056/NEJMoa2604126).
Presented by: Neeraj Agarwal, MD, FASCO, Professor, Presidential Endowed Chair of Cancer Research, Director GU Program and the Center of Investigational Therapeutics (CIT), Huntsman Cancer Institute, University of Utah, Salt Lake City, UT
Written by: Julian Chavarriaga, MD, Clinical Assistant Professor, Urologic Oncologist, Department of Urology at Penn State Health @chavarriagaj on X during the American Society of Clinical Oncology Genitourinary (ASCO) Annual Meeting held in Chicago, IL between May 29th and June 1st, 2026
Related content: TALAPRO-3 Trial Results for Talazoparib plus Enzalutamide in HRR-Mutant mHSPC - Neeraj Agarwal
- Agarwal N, Azad AA, Carles J, Fay AP, Matsubara N, Szczylik C, De Giorgi U, Young Joung J, Fong PCC, Voog E, Jones RJ, Shore ND, Saad F, Dunshee C, Zschäbitz S, Oldenburg J, Lin X, Healy CG, Kalac M, Kennedy D, Fizazi K. Talazoparib plus enzalutamide in men with metastatic castration-resistant prostate cancer: final overall survival results from the randomised, placebo-controlled, phase 3 TALAPRO-2 trial. Lancet. 2025 Aug 2;406(10502):447-460. doi: 10.1016/S0140-6736(25)00684-1. Epub 2025 Jul 16. PMID: 40683290.
- Saad F, Clarke NW, Oya M, Shore N, Procopio G, Guedes JD, Arslan C, Mehra N, Parnis F, Brown E, Schlürmann F, Joung JY, Sugimoto M, Sartor O, Liu YZ, Poehlein C, Barker L, Del Rosario PM, Armstrong AJ. Olaparib plus abiraterone versus placebo plus abiraterone in metastatic castration-resistant prostate cancer (PROpel): final prespecified overall survival results of a randomised, double-blind, phase 3 trial. Lancet Oncol. 2023 Oct;24(10):1094-1108. doi: 10.1016/S1470-2045(23)00382-0. Epub 2023 Sep 12. Erratum in: Lancet Oncol. 2024 May;25(5):e180. doi: 10.1016/S1470-2045(24)00209-2. PMID: 37714168.
- Hussain M, Kocherginsky M, Agarwal N, Adra N, Zhang J, Paller CJ, Picus J, Reichert ZR, Szmulewitz RZ, Tagawa ST, Kuzel TM, Bazzi LA, Daignault-Newton S, Whang YE, Dreicer R, Stephenson RD, Rettig MB, Shevrin D, Gerke T, Chinnaiyan AM, Antonarakis ES. Abiraterone, Olaparib, or Abiraterone + Olaparib in First-Line Metastatic Castration-Resistant Prostate Cancer with DNA Repair Defects (BRCAAway). Clin Cancer Res. 2024 Oct 1;30(19):4318-4328. doi: 10.1158/1078-0432.CCR-24-1402. PMID: 39115414.
- Agarwal N, Matsubara N, et al. PARP and androgen-signaling inhibition plus ADT in metastatic prostate cancer. N Engl J Med. 2026. doi:10.1056/NEJMoa2604126.