(UroToday.com) The 2026 American Society of Clinical Oncology Genitourinary (ASCO) Annual Meeting held in Chicago, IL, was host to the Prostate, Testicular, and Penile Cancer - Oral Abstracts. Dr. Joaquin Mateo presented Abstract 5006: Final results from ZZFIRST: A randomized phase 2 trial of enzalutamide and talazoparib in mHNPC.
Dr. Mateo began by highlighting that treatment intensification with ADT plus an ARPI is now considered the standard of care for metastatic hormone-naïve prostate cancer (mHNPC/APMN), significantly improving clinical outcomes across multiple phase III studies.1,2 However, she emphasized that treatment responses remain heterogeneous, with a persistent unmet need for more effective upfront therapeutic strategies, particularly among patients with high-volume disease who continue to experience poorer long-term outcomes despite contemporary intensification approaches.
He further discussed the growing interest in combined androgen receptor and PARP inhibition strategies, noting that AR-PARPi co-targeting has demonstrated enhanced clinical activity in metastatic castration-resistant prostate cancer. Nevertheless, important biological questions remain unresolved. Specifically, the underlying mechanisms governing the interaction between androgen receptor signaling and DNA damage repair pathways are still incompletely understood, and the proposed concept of treatment-induced “BRCAness” has not yet been definitively demonstrated in patient biopsy samples. He also emphasized ongoing uncertainty regarding the optimal patient population for this therapeutic approach. Currently, the combination of enzalutamide plus talazoparib is approved in metastatic castration-resistant prostate cancer based on TALAPRO-2,1 while its role in metastatic hormone-sensitive disease continues to be investigated in TALAPRO-3.3
Dr. Mateo then presented the investigator-initiated ZZFIRST trial, which evaluated enzalutamide with or without talazoparib in patients with metastatic hormone-naïve prostate cancer and high-volume disease, regardless of homologous recombination repair (HRR) mutation status. He emphasized that the primary scientific objective of the study was not only to evaluate clinical activity, but also to better understand tumor adaptation and mechanisms of resistance to enzalutamide through paired tumor biopsies obtained before treatment initiation and again during therapy. These translational analyses were designed to provide mechanistic insight into the biologic rationale underlying AR-PARP combination strategies.
The study enrolled 54 men with histologically confirmed prostate adenocarcinoma, high-volume metastatic disease by CHAARTED criteria, PSA ≥4 ng/mL at diagnosis or prior to ADT initiation, and no prior systemic therapy for metastatic disease other than up to 28 days of ADT before cycle 1 day 1. All patients initially received a lead-in phase consisting of enzalutamide 160 mg daily plus ADT for two 28-day cycles, with mandatory baseline and on-treatment tumor biopsies. After this initial 2-month treatment period, patients were randomized in a 2:1 fashion to either the interventional arm receiving talazoparib 0.5 mg daily plus enzalutamide and ADT, or the control arm receiving enzalutamide plus ADT alone. Randomization was stratified according to HRR mutation status from baseline tumor biopsies. Treatment continued until radiographic progression or unacceptable toxicity, with a planned minimum follow-up of 3 years.
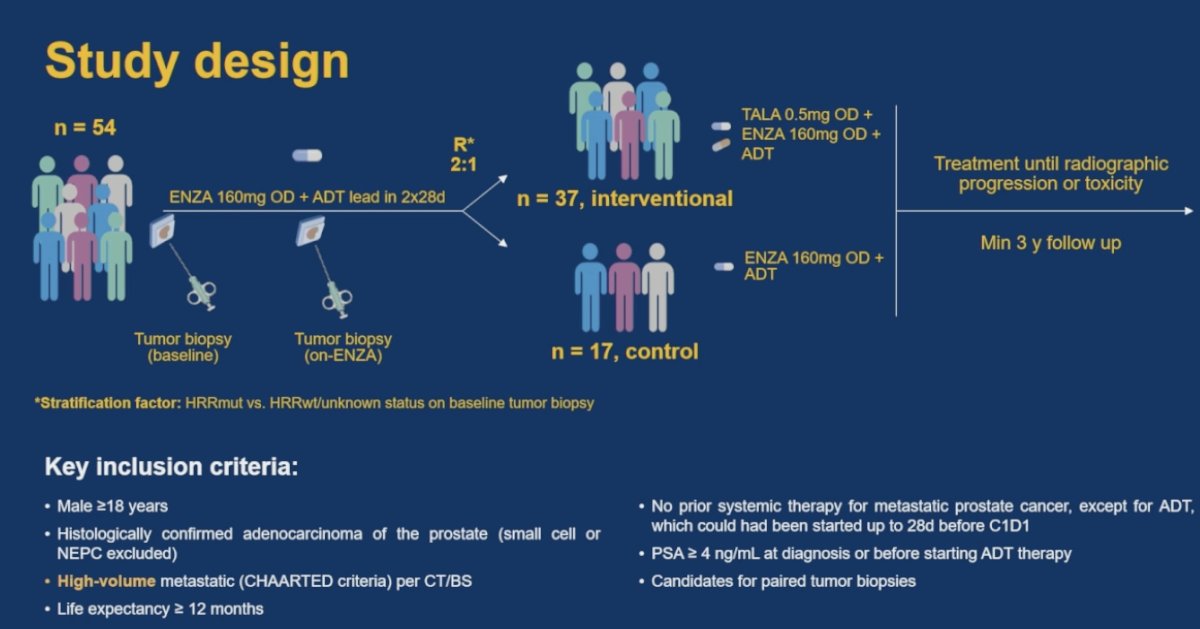
The primary endpoint of ZZFIRST was the proportion of patients achieving a PSA <0.2 ng/mL at 12 months. Secondary and exploratory endpoints included 7-month PSA <0.2 response rates, 7- and 12-month PSA nadir <4 ng/mL, PSA progression-free survival according to PCWG3 criteria, radiographic progression-free survival by RECIST v1.1 criteria, and PCWG3 criteria for bone disease, time to castration resistance, overall survival, and incidence and severity of adverse events graded according to NCI-CTCAE v5.0. Time to castration resistance was defined as PSA progression-free survival, and/or radiographic progression-free survival, and/or unequivocal clinical progression.
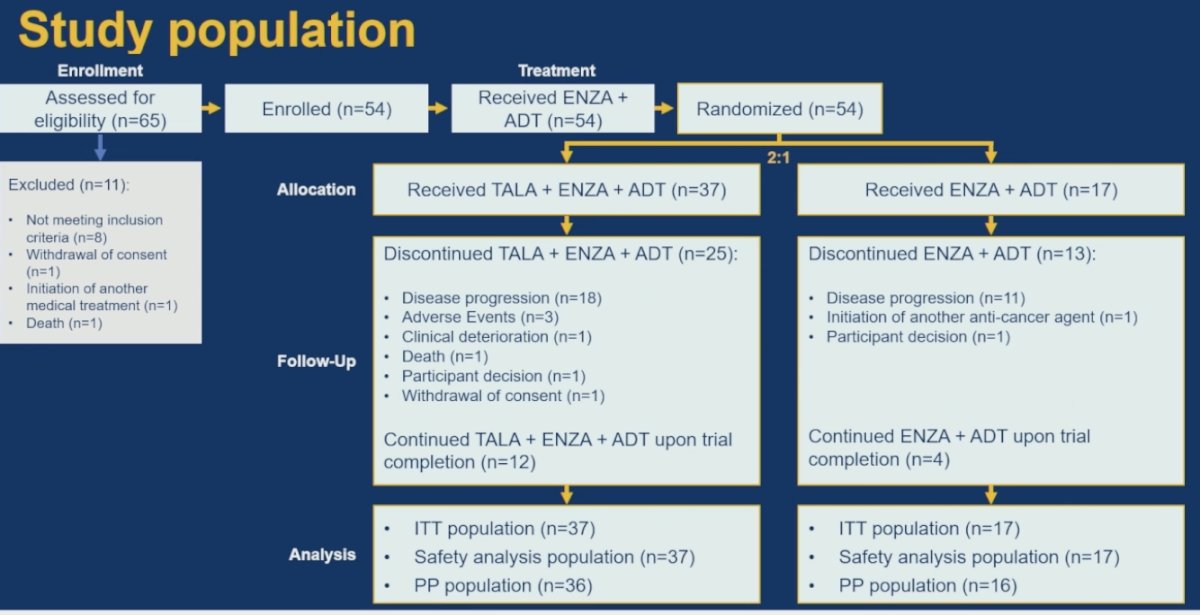
A total of 65 patients were assessed for eligibility, of whom 54 met inclusion criteria, enrolled, and initiated treatment with enzalutamide plus ADT. All 54 patients subsequently underwent randomization in a 2:1 fashion, with 37 patients assigned to talazoparib plus enzalutamide and ADT and 17 assigned to enzalutamide plus ADT alone. During follow-up, treatment discontinuation in both arms was primarily driven by disease progression, although adverse events, clinical deterioration, patient decision, withdrawal of consent, and death also contributed in smaller numbers. At trial completion, 12 patients in the talazoparib-containing arm and 4 patients in the control arm remained on study treatment.
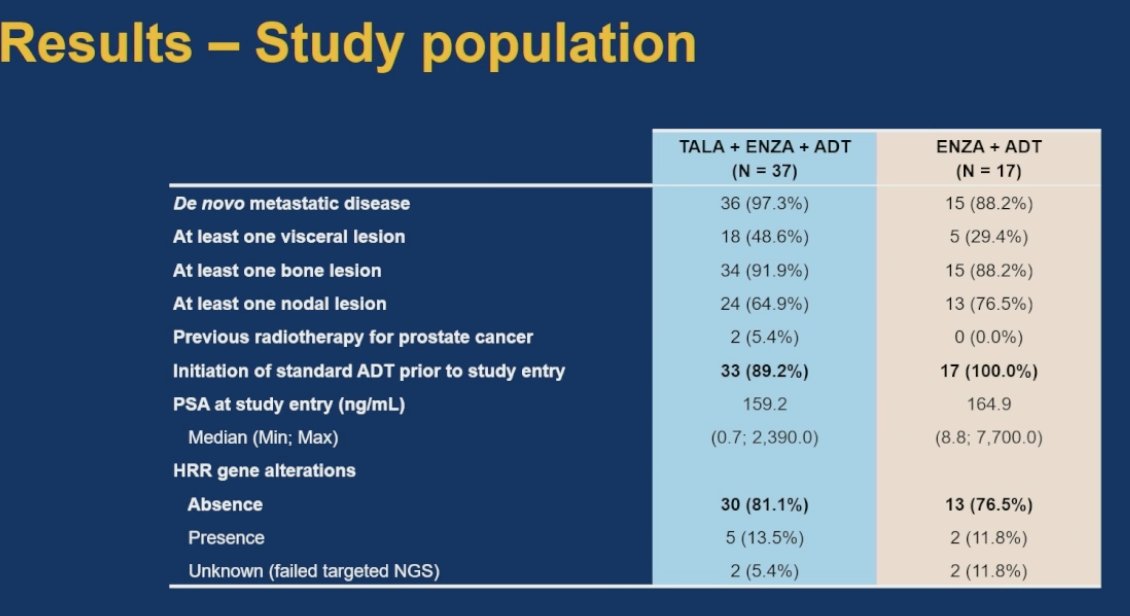
Dr. Mateo reviewed the baseline study population characteristics and highlighted that the majority of patients in both treatment arms presented with de novo metastatic disease and extensive metastatic involvement. Notably, patients randomized to the talazoparib plus enzalutamide and ADT arm had a higher prevalence of visceral metastases compared with the control arm (48.6% versus 29.4%). Importantly, most patients enrolled did not harbor homologous recombination repair alterations, with absence of HRR gene alterations observed in 81.1% of patients treated with talazoparib plus enzalutamide and ADT and 76.5% of those treated with enzalutamide plus ADT alone.
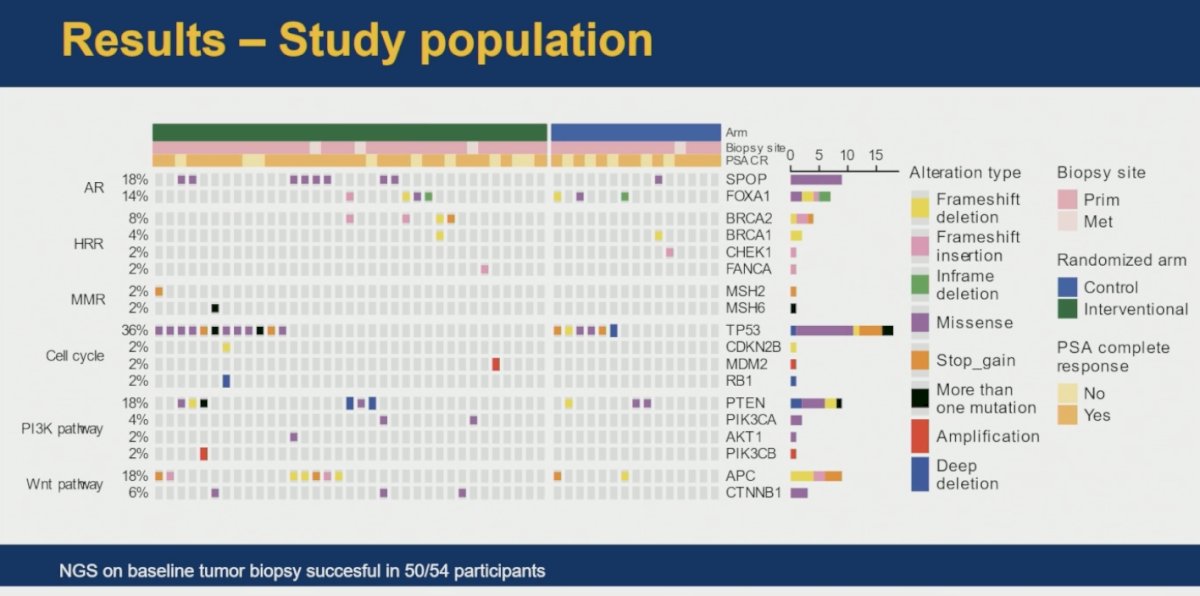
Next-generation sequencing from baseline tumor biopsies was successfully completed in 50 of the 54 enrolled participants. Dr. Mateo noted that the remaining 4 patients did not have sufficient tumor material available for successful molecular analysis. The genomic landscape demonstrated alterations across multiple biologic pathways, including androgen receptor signaling, homologous recombination repair, mismatch repair, cell cycle regulation, PI3K pathway alterations, and Wnt pathway alterations, further highlighting the molecular heterogeneity of high-volume metastatic hormone-naïve prostate cancer.
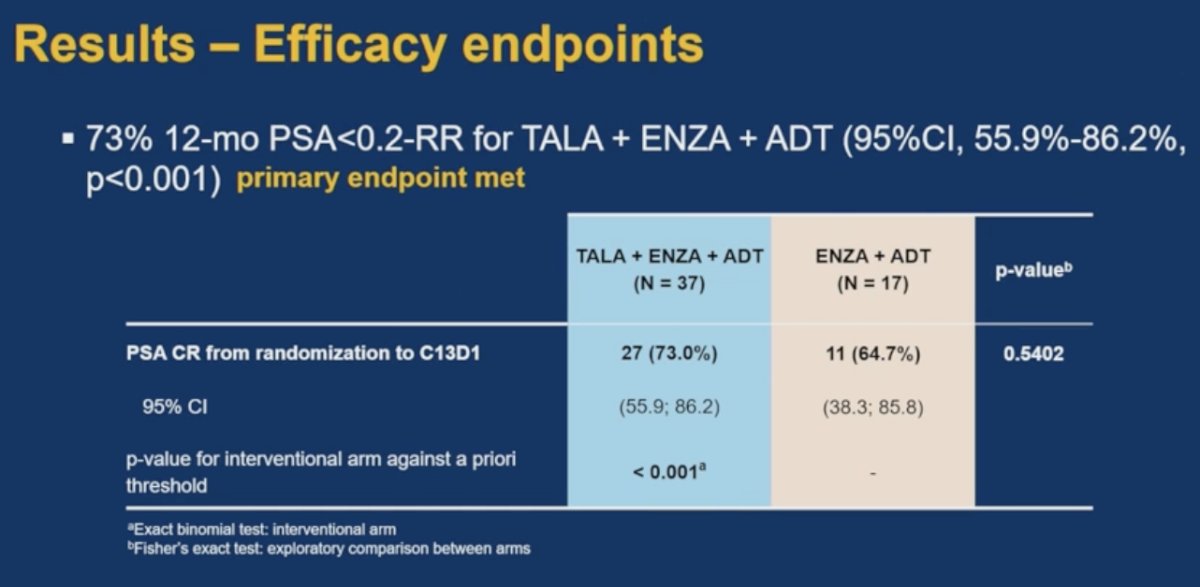
The ZZFIRST trial met its primary endpoint, with 73% of patients treated with talazoparib plus enzalutamide and ADT achieving a PSA <0.2 ng/mL at 12 months (95% CI 55.9%-86.2%; p<0.001). Dr. Mateo highlighted, however, that response rates were also notably high in the control arm, where 64.7% of patients treated with enzalutamide plus ADT achieved a PSA complete response by cycle 13 day 1. Importantly, there was no statistically significant difference between treatment arms in this exploratory comparison (p=0.5402), despite the numerically higher response rate observed with the talazoparib-containing combination.
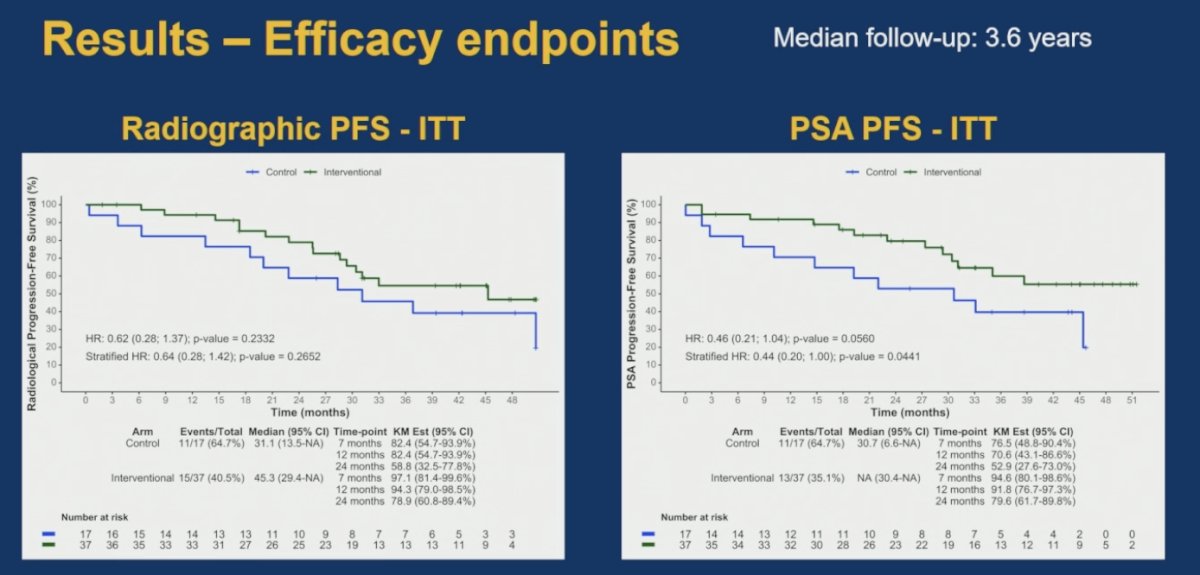
With a median follow-up of 3.6 years, Dr. Mateo presented encouraging exploratory progression-free survival outcomes favoring the talazoparib-containing combination. In the intention-to-treat population, radiographic progression-free survival demonstrated a numerical improvement with talazoparib plus enzalutamide and ADT compared with enzalutamide plus ADT alone, with a stratified hazard ratio of 0.64, although this did not reach statistical significance (p=0.2652).
Similarly, PSA progression-free survival showed a stronger trend favoring the interventional arm. The stratified hazard ratio for PSA progression-free survival was 0.44 (95% CI 0.20-1.00), with a p-value of 0.0441, suggesting delayed PSA progression with the addition of talazoparib. Median PSA progression-free survival was not reached in the interventional arm compared with 30.7 months in the control group.
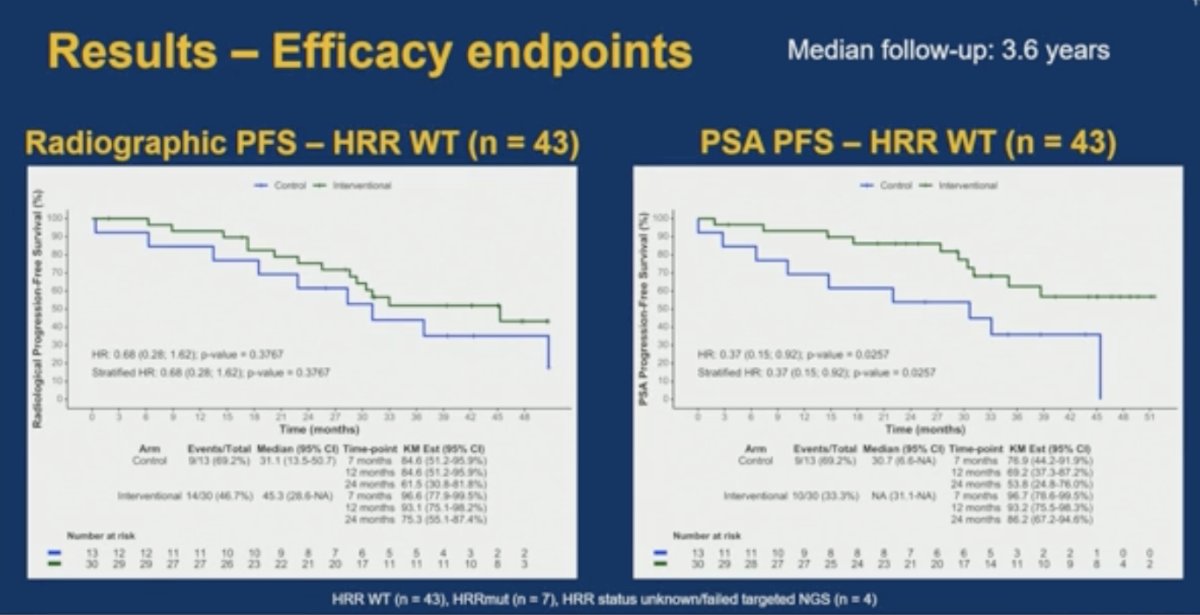
In exploratory subgroup analyses restricted to patients without homologous recombination repair alterations (HRR wild-type, n=43), similar efficacy trends were observed favoring the talazoparib-containing combination. Radiographic progression-free survival numerically favored talazoparib plus enzalutamide and ADT, although without statistical significance. More notably, PSA progression-free survival demonstrated a stronger separation between treatment arms, with a stratified hazard ratio of 0.37 and p=0.0257, suggesting delayed PSA progression even among patients without detectable HRR alterations.
Dr. Mateo next reviewed the safety and tolerability findings of the study. Dose reductions related to treatment-emergent adverse events occurred in 37.8% of patients receiving talazoparib plus enzalutamide and ADT, while enzalutamide dose reductions were required in 8.1% of patients in the interventional arm and 11.8% of those treated with enzalutamide plus ADT alone. Temporary treatment interruptions were also substantially more common in the talazoparib-containing arm (70.3% versus 17.6%), and permanent treatment discontinuation due to adverse events occurred in 32.4% of patients receiving talazoparib plus enzalutamide and ADT.
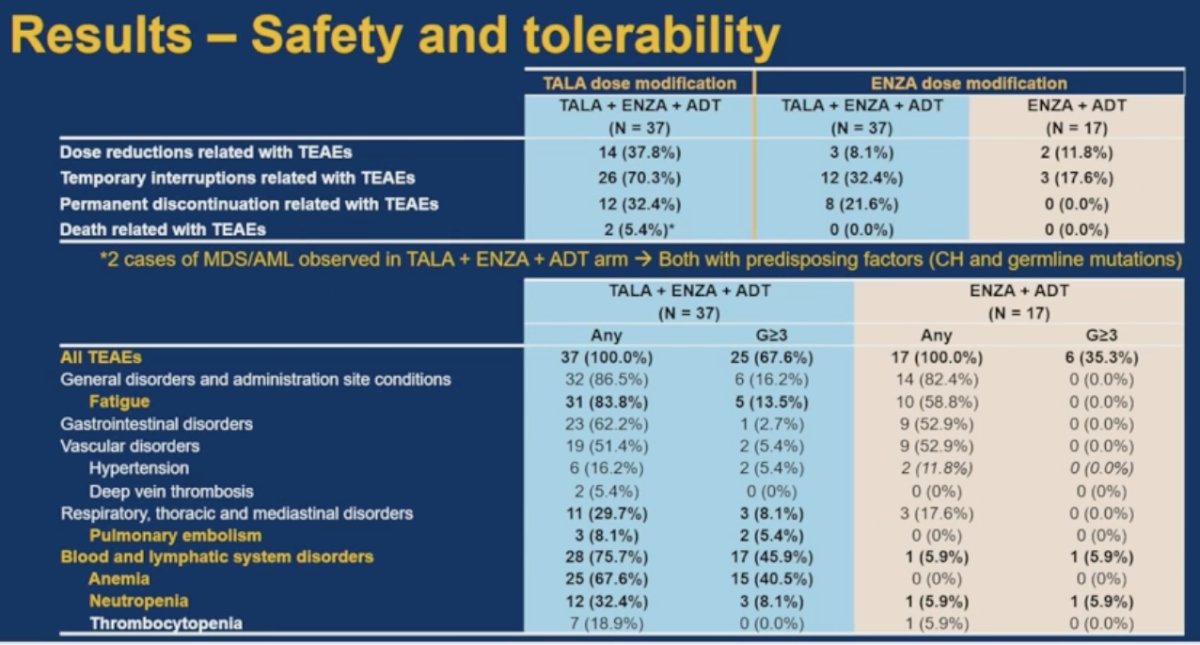
Importantly, two cases of MDS/AML were observed in the interventional arm. Dr. Mateo noted that both patients had predisposing biologic factors, including clonal hematopoiesis and germline mutations. Compared with the control arm, patients receiving talazoparib plus enzalutamide and ADT experienced higher rates of hematologic toxicities, including anemia, neutropenia, and thrombocytopenia, as well as increased thromboembolic events and fatigue.
Dr. Mateo then presented translational analyses evaluating tumor adaptation to androgen receptor signaling following treatment exposure. Paired on-treatment biopsies demonstrated upregulation of inflammatory and epithelial-to-mesenchymal transition (EMT) signatures, suggesting activation of adaptive resistance pathways during AR blockade. At the same time, enzalutamide exposure was associated with marked suppression of androgen receptor signaling pathways and proliferation-related signatures across tumor samples.
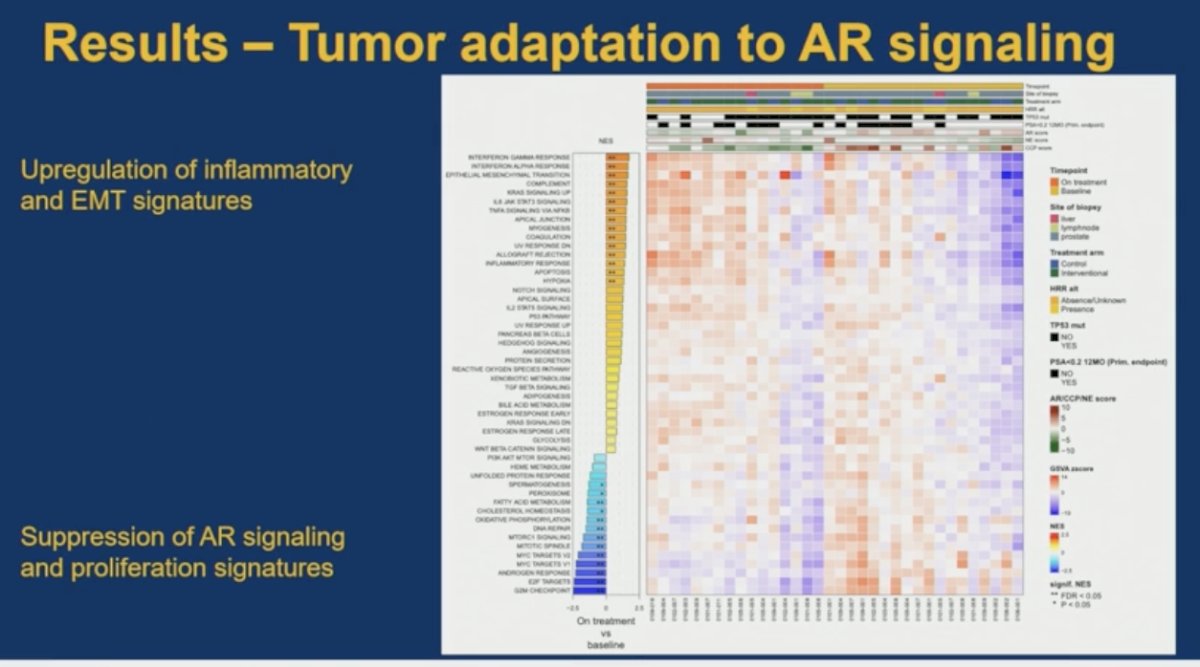
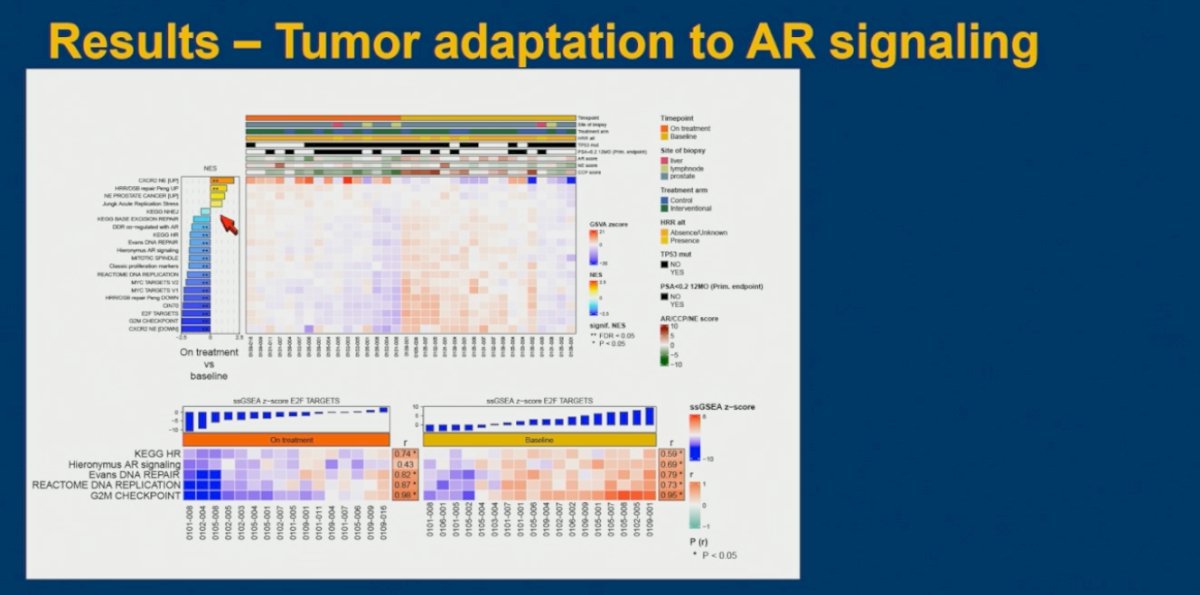
He further highlighted the presence of distinct biologic signatures within the paired biopsies, including severe downregulation of proliferation programs and cell-cycle–related pathways. Dr. Mateo noted that these findings likely reflect a biologic effect of treatment-induced proliferation arrest, with tumor cells entering a less proliferative state under potent AR inhibition. Baseline proliferation markers appeared to influence these downstream biologic adaptations, and he discussed that some of these observed molecular effects may also relate to homologous recombination repair biology and interactions between AR signaling suppression and DNA damage response pathways.
Dr. Mateo next presented exploratory analyses evaluating tumor adaptation to androgen receptor signaling through assessment of RAD51 function and DNA damage response biomarkers in paired tumor biopsies. Using immunofluorescence-based assays performed on formalin-fixed paraffin-embedded prostate cancer biopsy specimens, investigators quantified markers including γH2AX, a marker of DNA damage, and RAD51, a functional marker of homologous recombination repair activity. These analyses were performed in a smaller subset of available samples, including specimens from the ZZFIRST cohort as well as samples from MD Anderson Cancer Center (NCT01409200).
Importantly, the investigators did not observe a significant decrease in RAD51 function following treatment exposure, suggesting no clear evidence that enzalutamide induced homologous recombination deficiency or a “BRCAness” phenotype in patient tumor samples. Similarly, there was no major change in γH2AX expression between baseline and on-treatment biopsies, indicating no substantial increase in detectable DNA damage signaling. Dr. Mateo noted that interpretation of these findings is challenging given the limited number of evaluable samples and the biologic effect of treatment-induced proliferation arrest, as fewer actively dividing tumor cells may reduce the ability to detect DNA damage and repair activity within these assays.
Dr. Mateo acknowledged several important limitations of the ZZFIRST study. He emphasized that this was a relatively small, randomized phase II academic trial with a limited number of patients harboring HRR alterations, and patients were not stratified according to BRCA versus non-BRCA HRR mutations. As such, the study was not designed to definitively establish efficacy in molecularly selected subgroups, but rather to complement the efficacy data that will ultimately emerge from larger phase III studies such as TALAPRO-3.
From a translational standpoint, he noted that although this represents one of the largest series of paired on-treatment biopsies profiled in metastatic hormone-naïve prostate cancer, the number of evaluable samples remained limited because many on-treatment biopsies demonstrated insufficient residual tumor content following exposure to enzalutamide. He also highlighted that the study incorporated a 2-month enzalutamide lead-in period prior to randomization specifically to facilitate on-treatment biopsy collection, an important design feature that differs from several registration studies evaluating ARPI plus PARP inhibitor combinations. Dr. Mateo noted that these design differences may contribute to differences in biologic findings and potentially clinical outcomes across studies.
Dr Mateo concluded, emphasizing the following key takeaway points:
- Signs of clinical activity were observed with the combination of enzalutamide plus talazoparib in metastatic hormone-naïve prostate cancer, although these responses came at the expense of increased treatment-related toxicities.
- AR inhibition induced significant transcriptional reprogramming within tumor samples, including suppression of AR signaling and proliferation pathways, but without clear evidence of a functional homologous recombination deficient state.
- Biology-driven and biomarker-informed treatment approaches remain critical to maximize therapeutic benefit while minimizing unnecessary toxicity and treatment-related risk.
Presented by: Joaquin Mateo, MD, PhD, Medical Oncologist, Prostate Cancer Translational Research Group at the Vall d’Hebron Institute of Oncology (VHIO), Barcelona, Spain
Written by: Julian Chavarriaga, MD, Clinical Assistant Professor, Urologic Oncologist, Department of Urology at Penn State Health @chavarriagaj on X during the American Society of Clinical Oncology Genitourinary (ASCO) Annual Meeting held in Chicago, IL between May 29th and June 1st, 2026
References:
- Agarwal N, Azad AA, Carles J, Fay AP, Matsubara N, Szczylik C, De Giorgi U, Young Joung J, Fong PCC, Voog E, Jones RJ, Shore ND, Saad F, Dunshee C, Zschäbitz S, Oldenburg J, Lin X, Healy CG, Kalac M, Kennedy D, Fizazi K. Talazoparib plus enzalutamide in men with metastatic castration-resistant prostate cancer: final overall survival results from the randomised, placebo-controlled, phase 3 TALAPRO-2 trial. Lancet. 2025 Aug 2;406(10502):447-460. doi: 10.1016/S0140-6736(25)00684-1. Epub 2025 Jul 16. PMID: 40683290.
- Saad F, Clarke NW, Oya M, Shore N, Procopio G, Guedes JD, Arslan C, Mehra N, Parnis F, Brown E, Schlürmann F, Joung JY, Sugimoto M, Sartor O, Liu YZ, Poehlein C, Barker L, Del Rosario PM, Armstrong AJ. Olaparib plus abiraterone versus placebo plus abiraterone in metastatic castration-resistant prostate cancer (PROpel): final prespecified overall survival results of a randomised, double-blind, phase 3 trial. Lancet Oncol. 2023 Oct;24(10):1094-1108. doi: 10.1016/S1470-2045(23)00382-0. Epub 2023 Sep 12. Erratum in: Lancet Oncol. 2024 May;25(5):e180. doi: 10.1016/S1470-2045(24)00209-2. PMID: 37714168.
- Agarwal N, Matsubara N, et al. PARP and androgen-signaling inhibition plus ADT in metastatic prostate cancer. N Engl J Med. 2026. doi:10.1056/NEJMoa2604126.