(UroToday.com) The 2026 American Society of Clinical Oncology Genitourinary (ASCO) Annual Meeting held in Chicago, IL, was host to the Prostate, Testicular, and Penile Cancer - Oral Abstracts. Dr. Dingwei Ye presented Abstract 5008: Fuzuloparib combined with abiraterone acetate and prednisone as first-line treatment for mCRPC: Interim results from the FUZUPRO trial.
Dr. Ye began by noting that abiraterone acetate plus prednisone remains a standard first-line treatment option for patients with metastatic castration-resistant prostate cancer.1 He highlighted that recent studies have also demonstrated meaningful antitumor activity with PARP inhibitors in patients harboring homologous recombination repair defects, raising interest in combined AR pathway and DNA damage response targeting strategies.1,2
Emerging evidence has suggested that combining PARP inhibition with standard abiraterone acetate plus prednisone may enhance antitumor activity compared with either approach alone. Dr. Ye explained that fuzuloparib is a novel, potent, orally available PARP inhibitor with established efficacy across multiple tumor types. He further noted that a prior phase I study evaluating fuzuloparib plus abiraterone acetate plus prednisone in metastatic castration-resistant prostate cancer demonstrated favorable safety, encouraging antitumor activity, and no significant drug-drug interactions between agents.3 Based on these findings, investigators developed the FUZUPRO study, an international, randomized, double-blind, placebo-controlled phase III trial evaluating fuzuloparib plus abiraterone acetate plus prednisone versus abiraterone acetate plus prednisone alone as first-line treatment for metastatic castration-resistant prostate cancer.
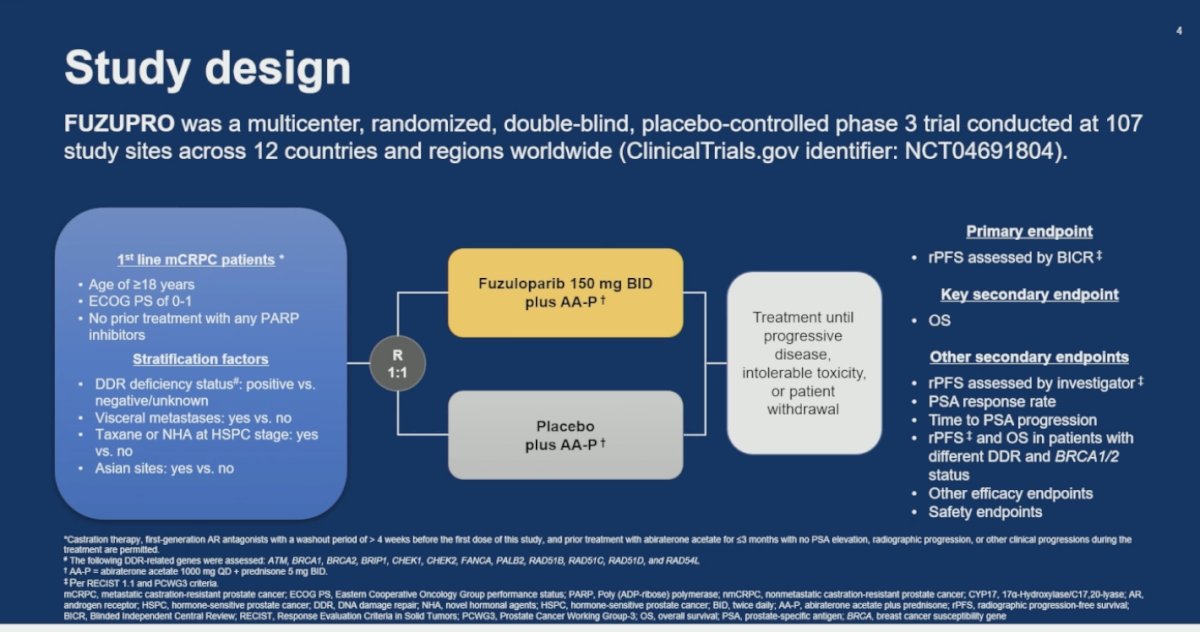
FUZUPRO was an international, multicenter, randomized, double-blind, placebo-controlled phase III trial conducted across 107 study sites in 12 countries and regions worldwide, including China, the United States, South Korea, and several European countries. The study enrolled patients with first-line metastatic castration-resistant prostate cancer who were at least 18 years old, had ECOG performance status 0–1, and had not previously received PARP inhibitors. Patients were randomized in a 1:1 fashion to receive fuzuloparib 150 mg twice daily plus abiraterone acetate and prednisone versus placebo plus abiraterone acetate and prednisone, with treatment continued until disease progression, intolerable toxicity, or withdrawal. (Study design shown below)
Stratification factors included DDR deficiency status (positive versus negative/unknown), presence of visceral metastases, prior taxane exposure in the hormone-sensitive setting, and Asian versus non-Asian study sites. The primary endpoint was blinded, independent central review-assessed radiographic progression-free survival, while overall survival served as the key secondary endpoint. Additional secondary endpoints included investigator-assessed radiographic progression-free survival, PSA response rate, time to PSA progression, radiographic progression-free survival according to DDR and BRCA1/2 status, additional efficacy outcomes, and safety endpoints.
Dr. Ye reviewed the statistical design of FUZUPRO, which planned to enroll 466 patients. Assuming a one-sided type I error of 0.025, the study required 303 radiographic progression-free survival events by blinded independent central review to provide 85.8% power to detect a hazard ratio of 0.70 for fuzuloparib plus abiraterone acetate and prednisone versus placebo plus abiraterone acetate and prednisone.
An interim efficacy analysis was planned after 258 radiographic progression-free survival events, representing 85% of the total expected events, or after the last patient had completed 24 months of follow-up. At the March 23, 2025, data cutoff, the median time from randomization to cutoff was 33.3 months, with 259 radiographic progression-free survival events observed by blinded independent central review. The Lan-DeMets O’Brien-Fleming alpha-spending function was used to determine the efficacy boundary.
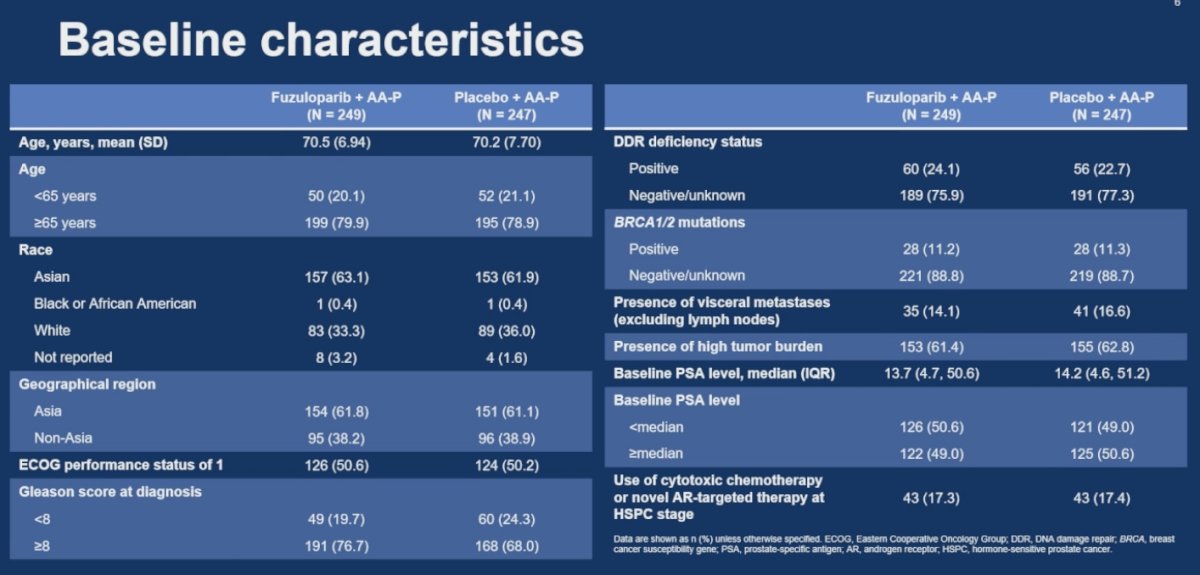
Baseline characteristics were generally well balanced between treatment arms. Dr. Ye highlighted that Gleason score ≥8 disease was slightly more common in the fuzuloparib plus abiraterone acetate and prednisone arm compared with the placebo-containing arm (76.7% versus 68.0%). BRCA1/2 mutations were similarly distributed between groups, occurring in 11.2% and 11.3% of patients, respectively. The prevalence of visceral metastases was also comparable between treatment arms, observed in 14.1% of patients receiving fuzuloparib plus AA-P and 16.6% receiving placebo plus AA-P.
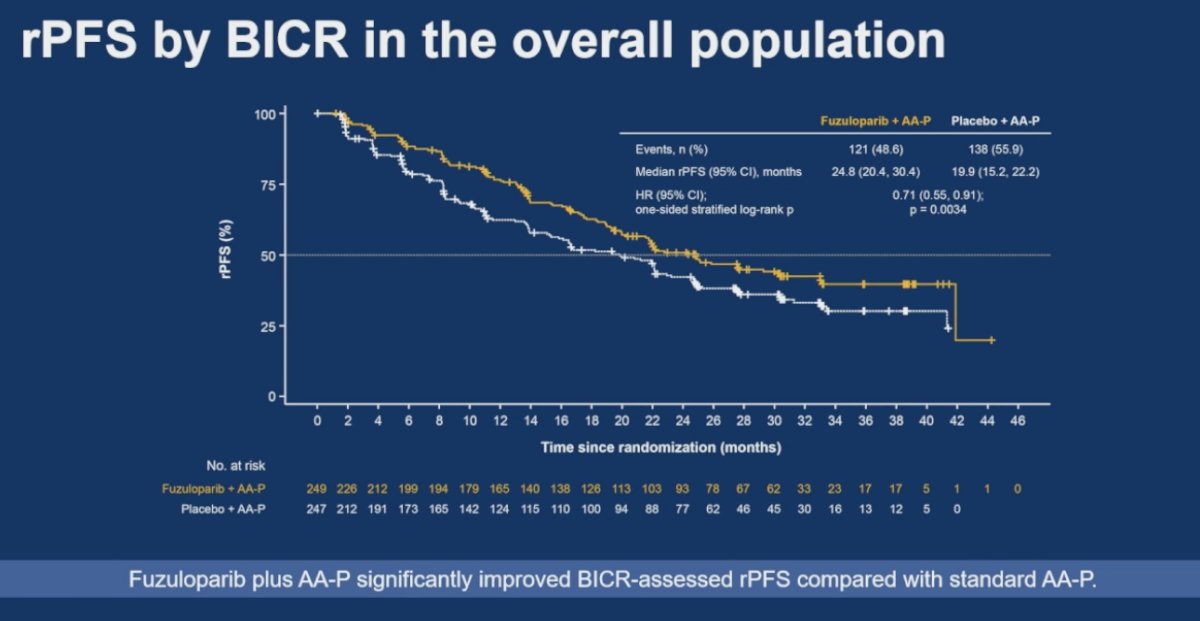
The FUZUPRO trial met its primary endpoint, demonstrating a significant improvement in blinded independent central review-assessed radiographic progression-free survival with fuzuloparib plus abiraterone acetate and prednisone compared with placebo plus abiraterone acetate and prednisone in the overall study population. Median radiographic progression-free survival was 24.8 months in the fuzuloparib arm versus 19.9 months in the control arm, corresponding to a hazard ratio of 0.71 (95% CI 0.55–0.91; p=0.0034).
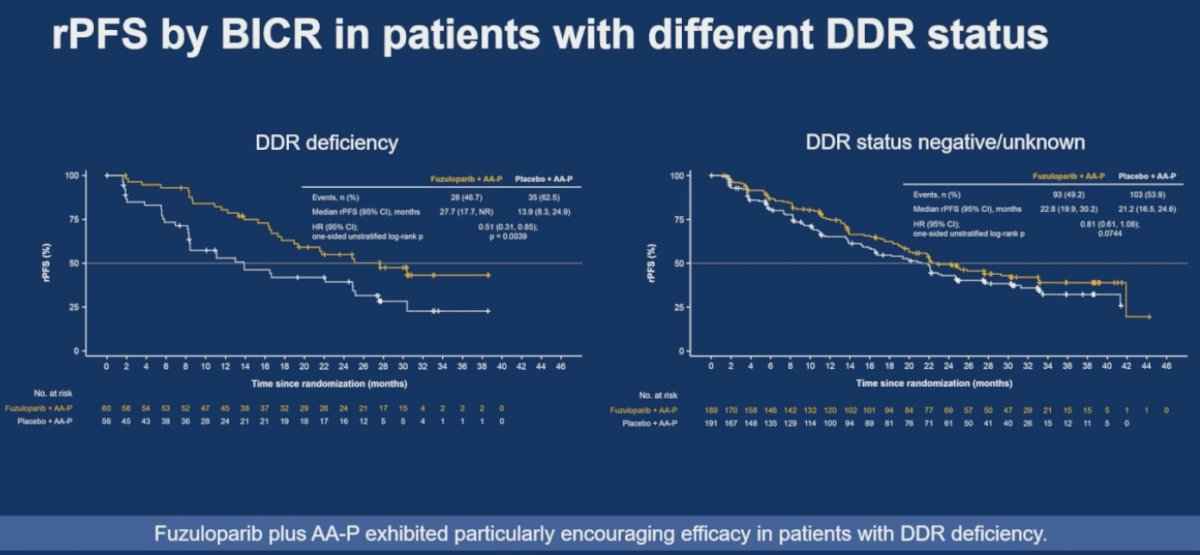
Fuzuloparib plus abiraterone acetate and prednisone demonstrated particularly encouraging activity among patients with DDR deficiency. In this subgroup, median radiographic progression-free survival by blinded independent central review was 27.7 months with fuzuloparib plus AA-P versus 13.9 months with placebo plus AA-P, corresponding to a hazard ratio of 0.51 (95% CI 0.31–0.83; p=0.0039).
In contrast, among patients with DDR-negative or unknown status, outcomes numerically favored the fuzuloparib-containing arm, although the magnitude of benefit was more modest and did not demonstrate the same degree of separation observed in the DDR-deficient population (HR 0.81; 95% CI 0.61–1.08; p=0.0744).
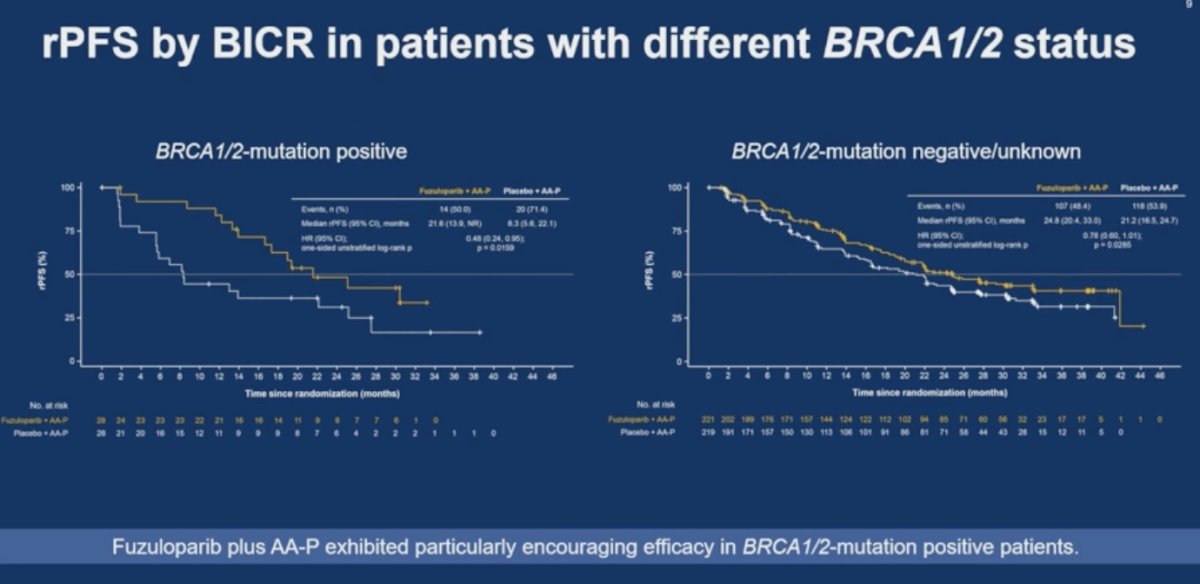
Among patients harboring BRCA1/2 alterations, fuzuloparib plus abiraterone acetate and prednisone demonstrated substantial improvement in radiographic progression-free survival compared with placebo plus AA-P. Median radiographic progression-free survival was 21.8 months in the fuzuloparib arm versus 8.3 months in the control arm, corresponding to a hazard ratio of 0.48 (95% CI 0.24–0.95; p=0.0159), with clear separation of the Kaplan-Meier curves favoring the combination strategy.
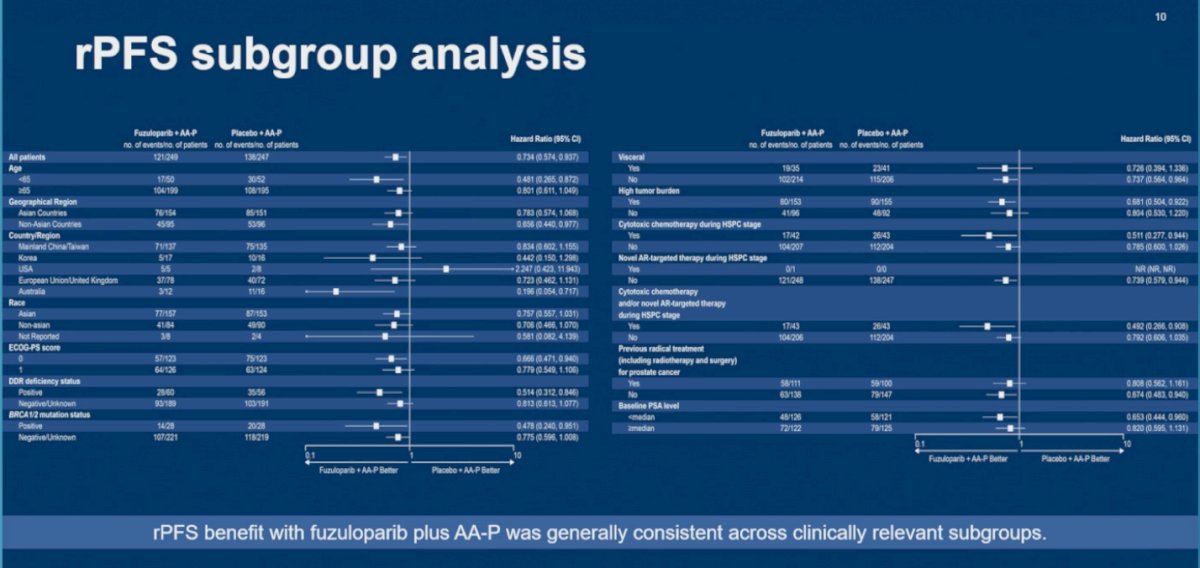
Subgroup analyses demonstrated that the radiographic progression-free survival benefit with fuzuloparib plus abiraterone acetate and prednisone was generally consistent across clinically relevant patient populations, including age, geographic region, ECOG performance status, DDR status, BRCA1/2 status, disease burden, visceral metastases, prior therapy exposure, and baseline PSA level. Dr. Ye noted, however, that some subgroup analyses, particularly those from the United States and certain non-Asian regions, included very small sample sizes, resulting in wide confidence intervals and limiting definitive interpretation of treatment effect within those subsets.
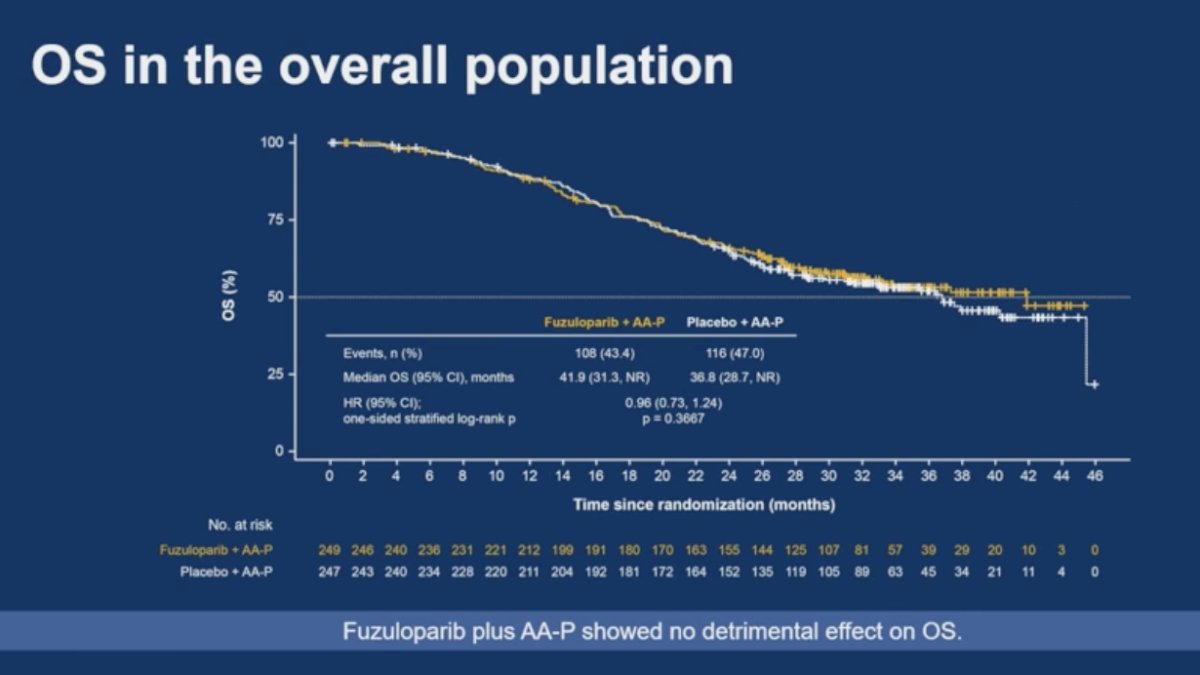
Overall survival analyses did not demonstrate a detrimental effect with the addition of fuzuloparib to abiraterone acetate and prednisone. In the overall study population, median overall survival was 41.9 months in the fuzuloparib arm versus 36.8 months in the placebo arm, with a hazard ratio of 0.96 (95% CI 0.73–1.24; p=0.3667).
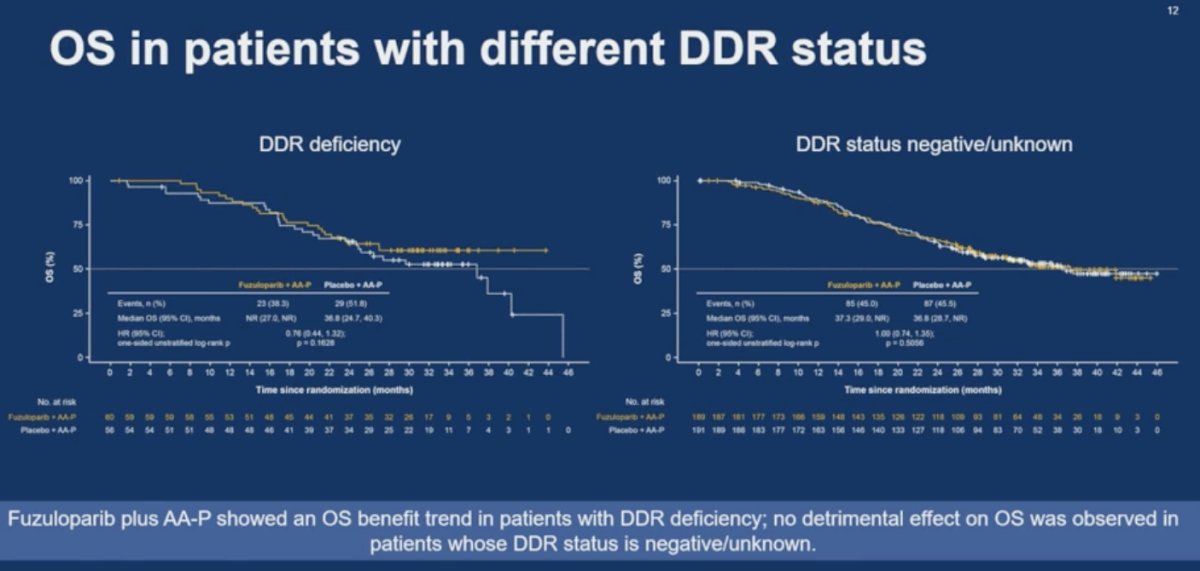
In exploratory subgroup analyses according to DDR status, patients with DDR deficiency demonstrated a numerical trend toward improved overall survival with fuzuloparib plus AA-P (HR 0.76), whereas patients with DDR-negative or unknown status showed no benefit with the combination strategy (HR 1.00).
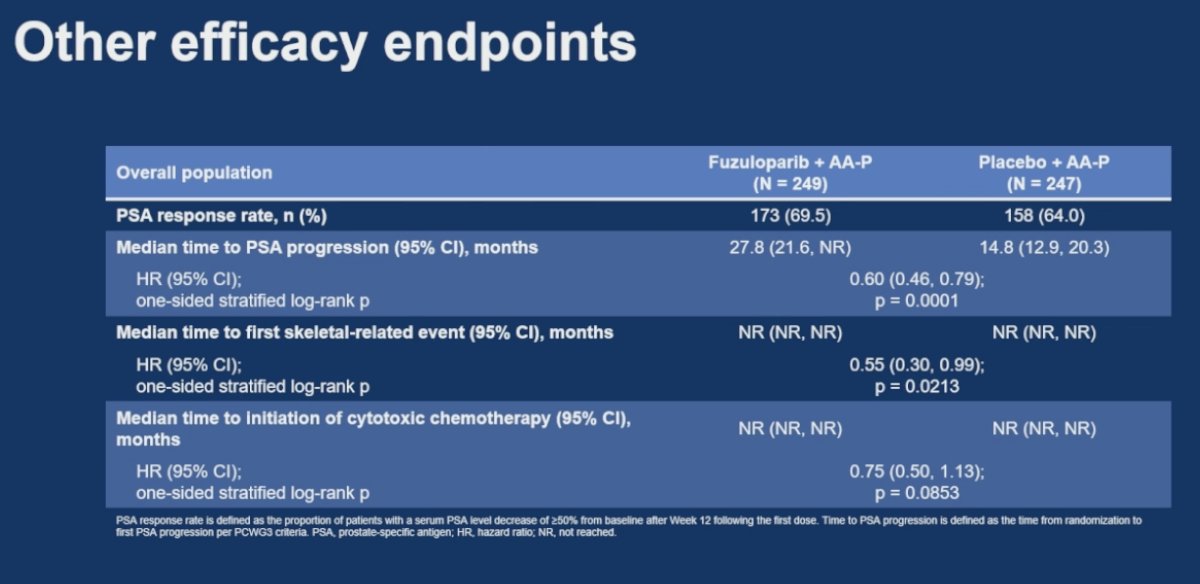
Additional efficacy endpoints also favored the fuzuloparib-containing regimen. PSA response rates were numerically higher with fuzuloparib plus abiraterone acetate and prednisone compared with placebo plus AA-P (69.5% versus 64.0%). Median time to PSA progression was significantly prolonged at 27.8 months versus 14.8 months, corresponding to a hazard ratio of 0.60 (95% CI 0.46–0.79; p=0.0001). Furthermore, fuzuloparib plus AA-P significantly delayed time to first skeletal-related event (HR 0.55; 95% CI 0.30–0.99; p=0.0213). A numerical trend toward delayed initiation of cytotoxic chemotherapy was also observed with the combination arm, although this did not reach statistical significance (HR 0.75; 95% CI 0.50–1.13; p=0.0853).
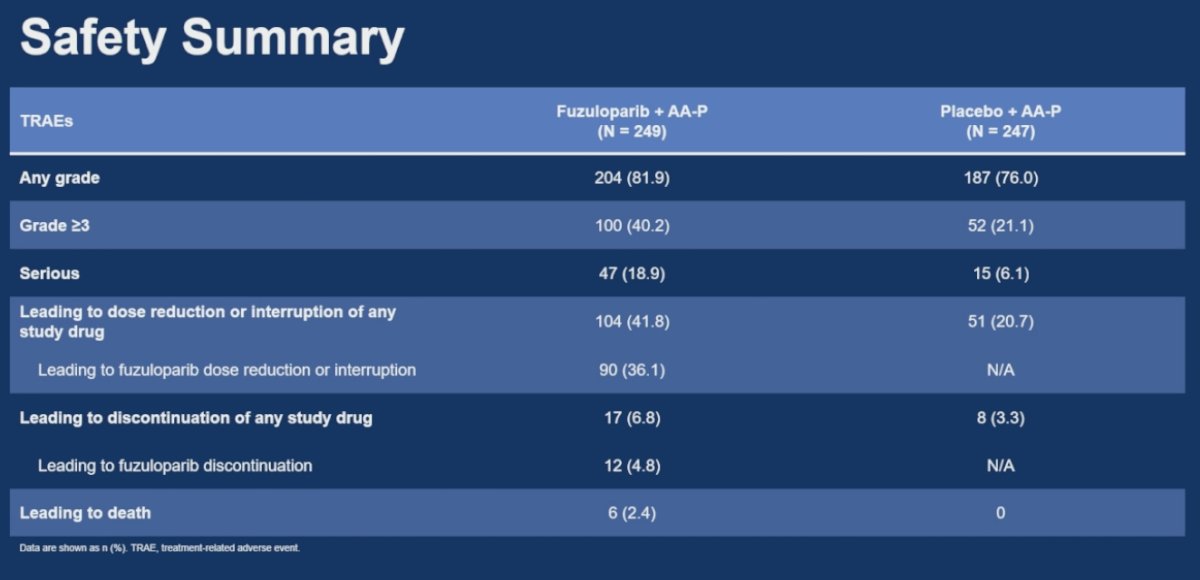
Lastly, Dr. Ye reviewed the safety profile of the combination regimen. Treatment-related adverse events of any grade occurred in 81.9% of patients treated with fuzuloparib plus abiraterone acetate and prednisone compared with 76% in the placebo arm, while grade ≥3 treatment-related adverse events occurred in 40.2% versus 21.1%, respectively Treatment-related adverse events leading to dose reduction or interruption of any study drug occurred in 41.8% of patients receiving fuzuloparib plus AA-P compared with 20.7% in the placebo arm, while treatment discontinuation rates remained relatively low at 6.8% versus 3.3%, respectively. Anemia, thrombocytopenia, and alanine aminotransferase elevation were among the most common adverse events observed with the combination regimen.
Dr Ye wrapped up his presentation with the following key take home points:
- FUZUPRO met its primary endpoint, demonstrating significantly improved radiographic progression-free survival with fuzuloparib plus AA-P versus placebo plus AA-P.
- Benefit was particularly pronounced in patients with DDR deficiency and BRCA1/2 alterations.
- No detrimental effect on overall survival was observed with the addition of fuzuloparib.
- Time to PSA progression and time to first skeletal-related event also favored the fuzuloparib-containing regimen.
- The safety profile was manageable and generally consistent with known PARP inhibitor toxicities.
Presented by: Dingwei Ye, Fudan University Shanghai Cancer Center, Shanghai, China
Written by: Julian Chavarriaga, MD, Clinical Assistant Professor, Urologic Oncologist, Department of Urology at Penn State Health @chavarriagaj on X during the American Society of Clinical Oncology Genitourinary (ASCO) Annual Meeting held in Chicago, IL between May 29th and June 1st, 2026
References:- Saad F, Clarke NW, Oya M, Shore N, Procopio G, Guedes JD, Arslan C, Mehra N, Parnis F, Brown E, Schlürmann F, Joung JY, Sugimoto M, Sartor O, Liu YZ, Poehlein C, Barker L, Del Rosario PM, Armstrong AJ. Olaparib plus abiraterone versus placebo plus abiraterone in metastatic castration-resistant prostate cancer (PROpel): final prespecified overall survival results of a randomised, double-blind, phase 3 trial. Lancet Oncol. 2023 Oct;24(10):1094-1108. doi: 10.1016/S1470-2045(23)00382-0. Epub 2023 Sep 12. Erratum in: Lancet Oncol. 2024 May;25(5):e180. doi: 10.1016/S1470-2045(24)00209-2. PMID: 37714168.
- Agarwal N, Azad AA, Carles J, Fay AP, Matsubara N, Szczylik C, De Giorgi U, Young Joung J, Fong PCC, Voog E, Jones RJ, Shore ND, Saad F, Dunshee C, Zschäbitz S, Oldenburg J, Lin X, Healy CG, Kalac M, Kennedy D, Fizazi K. Talazoparib plus enzalutamide in men with metastatic castration-resistant prostate cancer: final overall survival results from the randomised, placebo-controlled, phase 3 TALAPRO-2 trial. Lancet. 2025 Aug 2;406(10502):447-460. doi: 10.1016/S0140-6736(25)00684-1. Epub 2025 Jul 16. PMID: 40683290.
- Zhang T, Wang B, Wei Y, Gan H, Fang B, Li X, Wu J, Bian X, Wang J, Freedland SJ, Huang S, Ye D, Zhu Y. Neoadjuvant fuzuloparib combined with abiraterone for localized high-risk prostate cancer (FAST-PC): A single-arm phase 2 study. Cell Rep Med. 2025 Mar 18;6(3):102018. doi: 10.1016/j.xcrm.2025.102018. Epub 2025 Mar 7. PMID: 40056906; PMCID: PMC11970390.