(UroToday.com) The 2026 American Society of Clinical Oncology Genitourinary (ASCO) Annual Meeting held in Chicago, IL, was host to the Prostate, Testicular, and Penile Cancer - Oral Abstracts. Dr. Catherine H. Marshall discussed how to Minimize toxicity and maximize patient benefit in prostate cancer.
Dr. Marshall began with a common contemporary clinical scenario: a 72-year-old man with a rising PSA following prior local therapy whose imaging demonstrated lymphadenopathy greater than 3 cm both above and below the diaphragm, consistent with metastatic disease. She noted that this represents androgen-pathway modulation naïve disease (APMN), formerly referred to as metastatic hormone-sensitive prostate cancer (mHSPC).
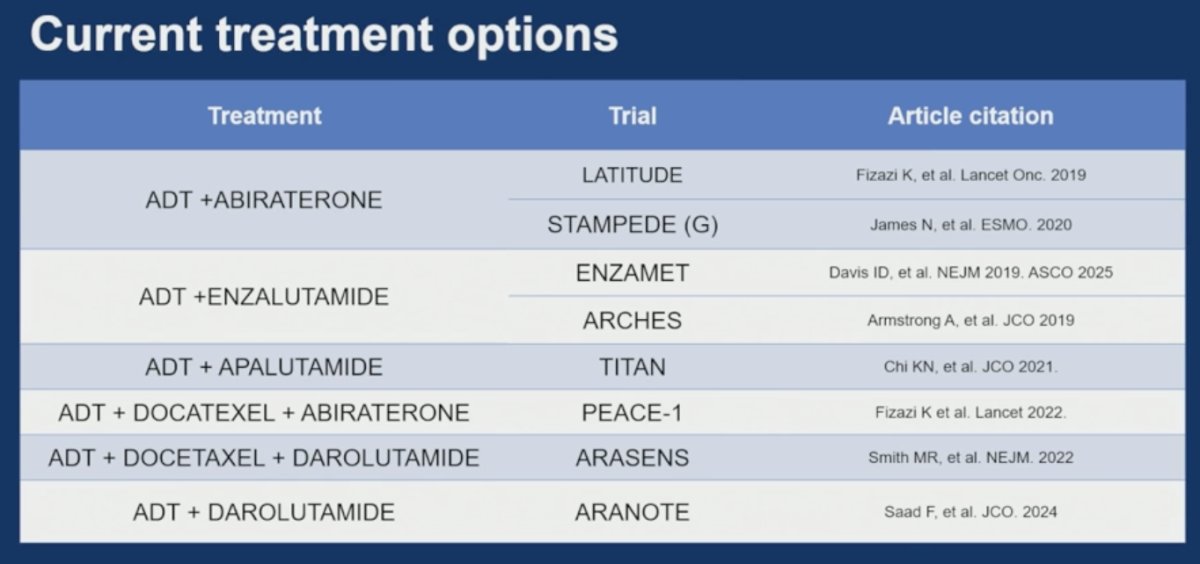
She emphasized that the therapeutic landscape for these patients has evolved dramatically over the last decade, with multiple treatment intensification strategies now available beyond ADT alone. Current treatment options include doublet therapy with ADT plus an ARPI such as abiraterone, enzalutamide, apalutamide, or darolutamide, as well as triplet therapy approaches incorporating docetaxel in selected patients with higher-volume or more aggressive disease. She noted that this expanding therapeutic landscape (presented below) raises increasingly important questions regarding optimal patient selection, treatment sequencing, toxicity mitigation, and biomarker-driven personalization of therapy. The key question remains how do we choose among all of these options?
She highlighted three key clinical questions that increasingly arise when treating patients with androgen-pathway modulation naïve metastatic prostate cancer in the modern era. First, should chemotherapy be incorporated into upfront treatment intensification strategies or avoided in selected patients? Second, when choosing hormonal intensification, should clinicians favor abiraterone or an androgen receptor inhibitor (“-amide” agent)? Finally, among the available ARPIs, how should clinicians decide which specific “-amide” to use for an individual patient based on efficacy, toxicity profile, comorbidities, and patient preferences?
For the question of whether to incorporate chemotherapy, Dr. Marshall emphasized that treatment decisions should be individualized and guided by multiple disease- and patient-specific factors rather than a one-size-fits-all approach. She highlighted several key considerations that influence chemotherapy selection, including tumor genomics, overall volume of disease, timing of metastatic presentation, symptom burden and comorbidities such as pain, as well as the specific location of metastatic involvement. She underscored that these clinical variables increasingly help determine which patients may derive the greatest benefit from treatment intensification strategies involving docetaxel.
When considering abiraterone versus an “-amide”, Dr. Marshall emphasized the importance of individual patient characteristics and comorbidities in treatment selection. For patients being considered for abiraterone, she highlighted several key factors that influence decision-making, including age, cardiovascular risk factors, the need for chronic steroid administration, seizure risk, cognitive frailty, and underlying liver disease. She noted that these variables can significantly impact both tolerability and safety, underscoring the importance of tailoring therapy to the individual patient rather than relying solely on efficacy data alone.
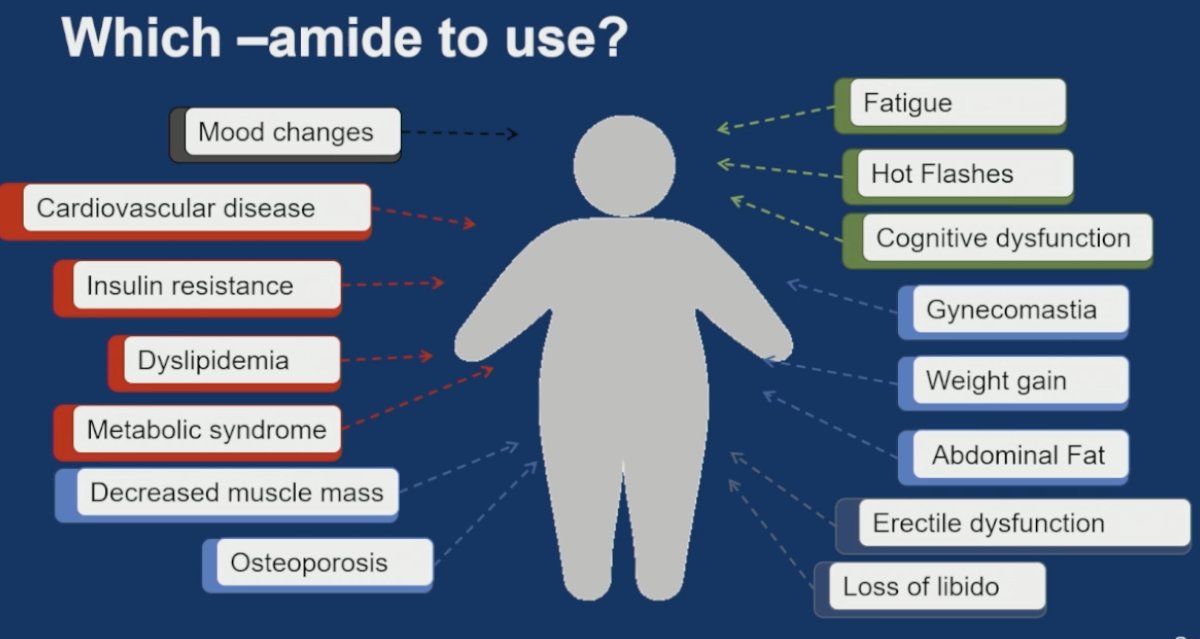
For the third key clinical question — which “-amide” to use — Dr. Marshall noted that clinicians currently have three major ARPI options available across clinical scenarios: enzalutamide, apalutamide, and darolutamide. She emphasized that although these agents demonstrate broadly similar efficacy in many settings, treatment selection is often driven by differences in toxicity profiles, comorbidities, drug-drug interactions, cognitive effects, seizure risk, tolerability, and patient preferences, making individualized treatment decisions increasingly important in contemporary practice.
Dr. Marshall emphasized that treatment selection in advanced prostate cancer increasingly requires balancing efficacy with the cumulative burden of treatment-related toxicities associated with both ADT and ARPIs. She reviewed the broad spectrum of adverse effects patients may experience, including cardiovascular disease, insulin resistance, dyslipidemia, metabolic syndrome, decreased muscle mass, osteoporosis, fatigue, hot flashes, gynecomastia, weight gain, abdominal fat accumulation, erectile dysfunction, loss of libido, mood changes, and cognitive dysfunction. She noted that while clinicians have long recognized many of the metabolic and systemic complications associated with hormonal therapy, emerging data are now providing a better understanding of treatment-related cognitive dysfunction, which has become an increasingly important consideration when selecting among available ARPIs. Ultimately, she emphasized that clinicians now have a growing “menu” of effective treatment options, making individualized therapy selection based on toxicity profiles and patient-specific factors more important than ever.
Dr. Marshall also discussed the ARACOG trial presented earlier, noting the striking crossover findings, with substantially more patients switching from enzalutamide to darolutamide than vice versa. She emphasized, however, that several important limitations should be acknowledged when interpreting these data. The study included a heterogeneous mix of disease states, including nmCRPC/nmAPMR, mCRPC/APMR, and mHSPC populations, and the duration of prior ADT exposure in some cohorts remained unclear. In addition, darolutamide was provided free of charge through the trial, which may have influenced crossover decisions and patient preferences. She further noted that the extensive cognitive testing performed in the study is not routinely incorporated into standard clinical practice, limiting immediate real-world applicability.
Nevertheless, she emphasized that the trial meaningfully informs patient-clinician discussions regarding cognitive risks associated with ARPI therapy. While the study may not immediately change routine management algorithms, it provides increasingly relevant information as clinicians seek to personalize therapy selection based not only on efficacy, but also on quality-of-life considerations and neurocognitive toxicity profiles.
Returning to the clinical case, Dr. Marshall described the 72-year-old man with metastatic androgen pathway naïve disease who was started on ADT plus an ARPI and subsequently achieved a deep response, with a PSA <0.1 ng/mL after 18 months of therapy. She then posed an increasingly relevant clinical question in contemporary practice: does ADT truly need to continue indefinitely in patients with prolonged and profound responses?
She noted that, based on the current level of evidence, continuous therapy remains the standard approach and is what clinicians should continue to recommend today. In support of this, she referenced prior intermittent versus continuous ADT data from Hussain et al., where intermittent therapy did not demonstrate noninferiority in the metastatic setting, particularly among patients with metastatic disease.1 However, Dr. Marshall emphasized that several important caveats must be considered when interpreting the historical intermittent versus continuous ADT data that currently support indefinite therapy. She noted that the landmark study was originally designed in 1993, enrolled patients between May 1995 and September 2008, and was ultimately published in 2013 well before the contemporary era of ARPI intensification.
In that trial, median overall survival was 5.8 years with continuous ADT compared with 5.1 years with intermittent ADT, corresponding to an approximate 10% relative increase in the risk of death with intermittent therapy. Although the study hypothesized that the hazard ratio for death would remain below 1.20 to establish noninferiority, the upper limit of the 95% confidence interval ultimately reached 1.23.1 As a result, the investigators concluded that they were unable to demonstrate that intermittent therapy was non-inferior to continuous therapy with respect to overall survival. Dr. Marshall highlighted that these findings continue to support ongoing continuous ADT today, although the applicability of these older data in the setting of modern ADT plus ARPI combinations remains an active area of investigation.
Dr. Marshall then discussed what the A-DREAM study adds to the current treatment landscape and whether clinicians should reconsider intermittent ADT strategies in the era of intensified upfront therapy with ADT plus ARPIs. She stated that the answer to this question is definitively yes, emphasizing that A-DREAM reopens an important clinical conversation that had largely been considered settled following older intermittent ADT studies. However, she cautioned that these findings are not yet practice changing.
She acknowledged several important limitations, including that enrollment appeared skewed toward lower-risk patients and that larger randomized prospective studies are still needed before treatment interruption strategies can be routinely adopted. Nevertheless, the study raises critical questions for the field: do patients truly require lifelong testosterone suppression in the era of deep responses achieved with modern intensified therapy? When and how can treatment safely be interrupted? Which patient and disease characteristics are most appropriate for treatment interruption approaches?
Importantly, she emphasized that while these data should not yet change standard management, they do change the nature of discussions clinicians can have with patients regarding long-term treatment planning, cumulative toxicities, quality of life, and emerging clinical trials exploring intermittent intensified therapy strategies that may ultimately redefine future standards of care.
Dr. Marshall concluded her presentation with the following key takeaway messages:
- Precision oncology and patient-centered care in advanced prostate cancer must focus not only on maximizing efficacy, but also on minimizing toxicity and thoughtfully considering opportunities for treatment discontinuation when appropriate.
- Comparative studies evaluating toxicity profiles across prostate cancer therapies provide clinically meaningful information that may help guide treatment selection, sequencing strategies, and individualized patient management.
- Additional prospective clinical trials are critically needed to evaluate intermittent treatment strategies and safe discontinuation approaches for long-term androgen pathway modulation in the modern era of intensified systemic therapy.
Presented by: Catherine H. Marshall, MD, MPH, Sidney Kimmel Comprehensive Cancer Center at Johns Hopkins University, Baltimore, MD
Written by: Julian Chavarriaga, MD, Clinical Assistant Professor, Urologic Oncologist, Department of Urology at Penn State Health @chavarriagaj on X during the American Society of Clinical Oncology Genitourinary (ASCO) Annual Meeting held in Chicago, IL between May 29th and June 1st, 2026
References:- Hussain M, Tangen CM, Berry DL, Higano CS, Crawford ED, Liu G, Wilding G, Prescott S, Kanaga Sundaram S, Small EJ, Dawson NA, Donnelly BJ, Venner PM, Vaishampayan UN, Schellhammer PF, Quinn DI, Raghavan D, Ely B, Moinpour CM, Vogelzang NJ, Thompson IM Jr. Intermittent versus continuous androgen deprivation in prostate cancer. N Engl J Med. 2013 Apr 4;368(14):1314-25. doi: 10.1056/NEJMoa1212299. PMID: 23550669; PMCID: PMC3682658.