(UroToday.com) The 2026 American Society of Clinical Oncology Genitourinary (ASCO) Annual Meeting held in Chicago, IL, was host to the Prostate, Testicular, and Penile Cancer - Oral Abstracts. Dr. Alicia K. Morgans presented Abstract 5005: Cognitive effects of darolutamide vs enzalutamide: Results of ARACOG (AFT-47), a randomized clinical trial from the Alliance for Clinical Trials in Oncology.
Dr. Morgans began by emphasizing that preservation of cognitive function remains a major priority for patients undergoing treatment for advanced prostate cancer. She noted that despite the widespread use of hormonal therapies and ARPIs, high-quality data describing their effects on cognition remain limited, with many prior studies lacking methodological rigor or prospective evaluation. She further highlighted that prospective comparisons assessing cognitive changes across distinct ARPIs are particularly scarce, especially within United States patient populations. To address this important clinical gap, the AFT-47 (ARACOG) study was designed as a prospective trial comparing both objective and subjective (patient-perceived) cognitive function among patients treated with darolutamide versus enzalutamide in a US population.
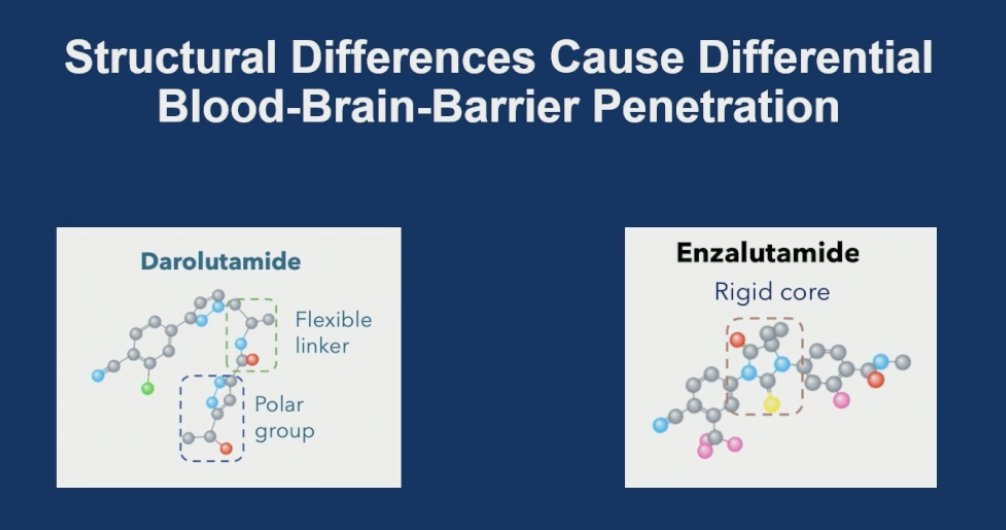
She noted that there are important structural differences between ARPIs that may influence central nervous system exposure and cognitive toxicity profiles. Preclinical studies have suggested that darolutamide has substantially lower blood-brain barrier penetration compared with enzalutamide, potentially related to its more flexible molecular structure and polar groups, whereas enzalutamide contains a more rigid core structure that may facilitate greater CNS penetration. These biologic differences provided part of the rationale for prospectively evaluating cognitive outcomes between these agents in the AFT-47 study.
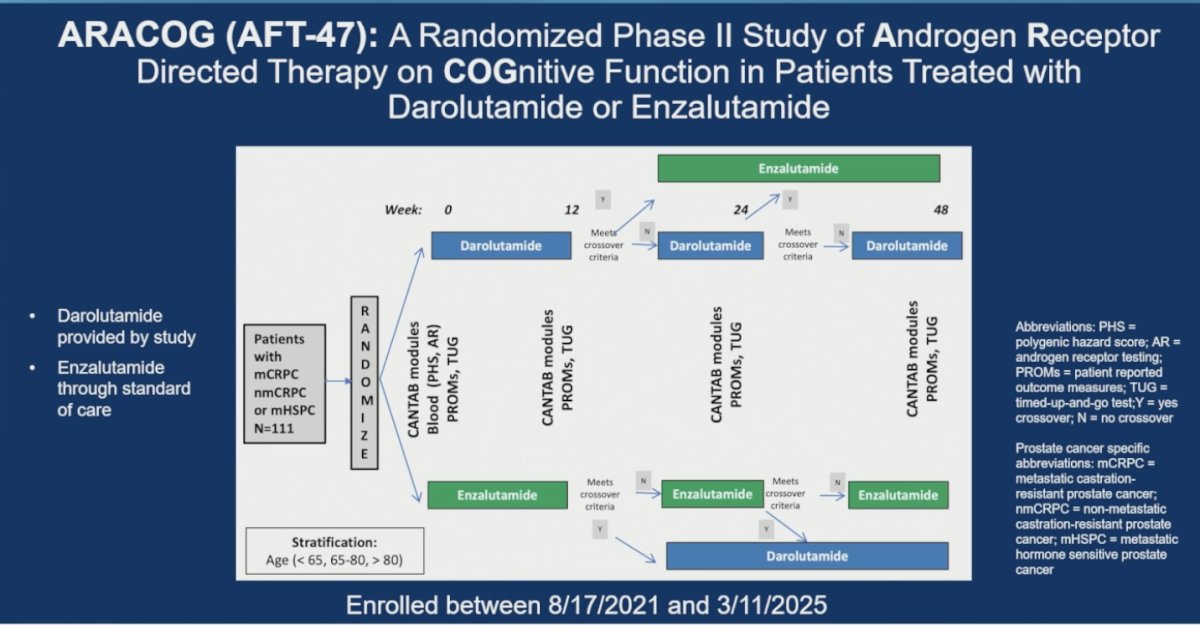
The phase II ARACOG (AFT-47) study was a randomized trial evaluating cognitive function in patients with metastatic castration-resistant, non-metastatic castration-resistant, or metastatic hormone-sensitive prostate cancer treated with darolutamide or enzalutamide. A total of 111 patients were randomized, with stratification by age (<65, 65–80, and >80 years). Cognitive and patient-reported assessments were performed at baseline and at 12, 24, and 48 weeks using CANTAB cognitive modules and PROMIS/TUG evaluations. Patients were allowed to cross over between treatments if predefined crossover criteria were met during the study. Darolutamide was provided through the clinical trial, whereas enzalutamide was administered according to standard of care. Importantly, all enrolled patients were required to meet eligibility criteria, ensuring a reasonable copayment burden prior to participation.
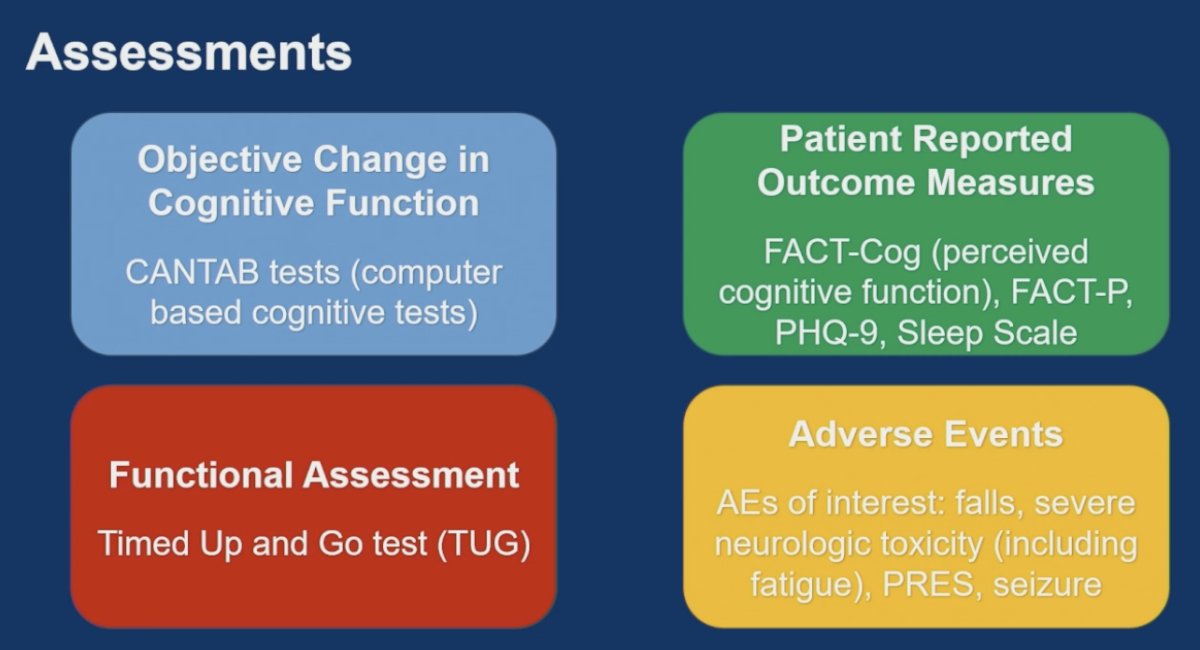
Patients underwent a comprehensive series of assessments (summarized below) evaluating both objective and subjective cognitive outcomes throughout the study. Objective cognitive function was assessed using CANTAB, a computerized cognitive testing platform. Patient-reported outcome measures included FACT-Cog for perceived cognitive function, FACT-P, PHQ-9, and sleep scale assessments. Functional status was evaluated using the Timed Up and Go (TUG) test. In addition, adverse events of special interest were prospectively monitored, including falls, severe neurologic toxicities such as fatigue, posterior reversible encephalopathy syndrome (PRES), and seizures.
The primary endpoint of ARACOG was the comparison between treatment arms in percent change from baseline to 24 weeks in the Maximally Changed Cognitive Domain (MCCD), a composite cognitive assessment derived from CANTAB testing. The endpoint was evaluated using five remotely deliverable computerized CANTAB modules assessing key cognitive domains, including executive function, visual memory, attention, and working memory. Because individual CANTAB tests assess overlapping cognitive domains, the investigators developed the MCCD approach as a more comprehensive method to capture the complexity of cognitive changes associated with ARPI therapy.
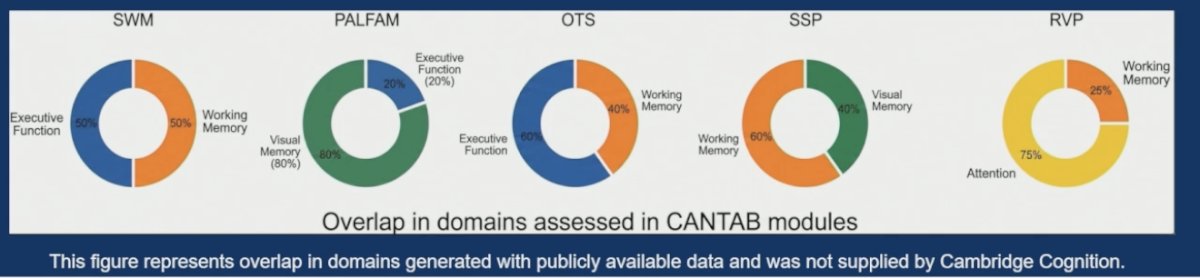
The graphic below further highlights the contribution of individual CANTAB modules across cognitive domains, including spatial working memory (SWM), paired associates learning (PALFAM), one-touch stockings (OTS), spatial span (SSP), and rapid visual processing (RVP). Importantly, the investigators emphasized that CANTAB modules are validated research tools designed for cognitive assessment in clinical trials rather than instruments intended for clinical diagnosis.
Moreover, Dr. Morgans highlighted that the selected CANTAB modules specifically targeted cognitive domains previously identified as being vulnerable during ADT treatment. Executive function assessments evaluated tasks such as planning schedules and breaking complex activities into discrete steps. Visual memory testing reflected real-world situations such as misplacing objects or becoming disoriented in familiar environments. Working memory assessments captured challenges such as losing track of conversations or forgetting names mid-discussion, while attention testing evaluated multitasking ability, including shifting between tasks or simultaneously responding to competing demands. Importantly, all CANTAB modules used in the study were clinically validated for remote completion, supporting the feasibility of longitudinal cognitive assessment in a multicenter setting.
Secondary endpoints included predefined crossover criteria designed to protect patients experiencing clinically meaningful cognitive or neurologic decline while on therapy. Crossover between treatment arms could occur at 12 or 24 weeks if patients experienced any qualifying event and elected to switch therapies. These criteria included a ≥30% decline in any CANTAB cognitive module, a ≥10-point decline in FACT-Cog scores, falls or increased fall risk as determined by the investigator, or development of a grade ≥2 neurologic toxicity event. The investigators also noted that patients who experienced falls, seizures, or posterior reversible encephalopathy syndrome (PRES) while receiving darolutamide would discontinue study participation rather than cross over to enzalutamide to avoid the risk of recurrent neurologic toxicity. Additionally, crossover outside the scheduled 12- and 24-week windows was permitted in the setting of severe neurocognitive adverse events.
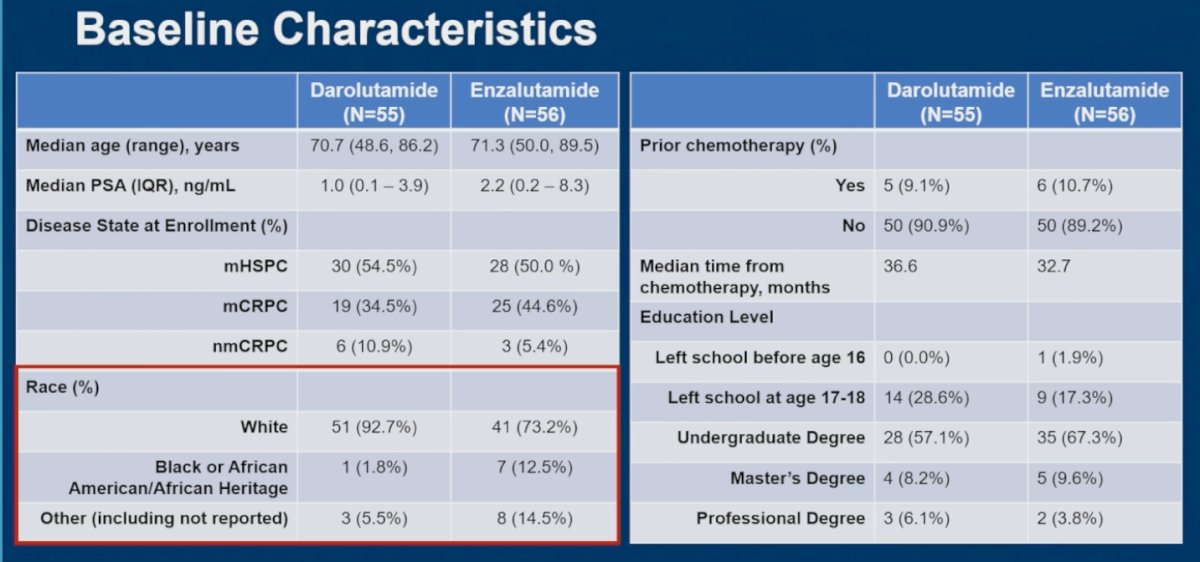
Dr. Morgans highlighted that baseline characteristics were generally balanced between treatment arms, although some notable differences were observed. The enzalutamide arm included a greater proportion of patients with metastatic castration-resistant prostate cancer compared with the darolutamide arm (44.6% vs 34.5%), suggesting a somewhat higher-risk population in the enzalutamide cohort. Additionally, a larger proportion of Black or African American patients were randomized to enzalutamide (12.5% vs 1.8%).
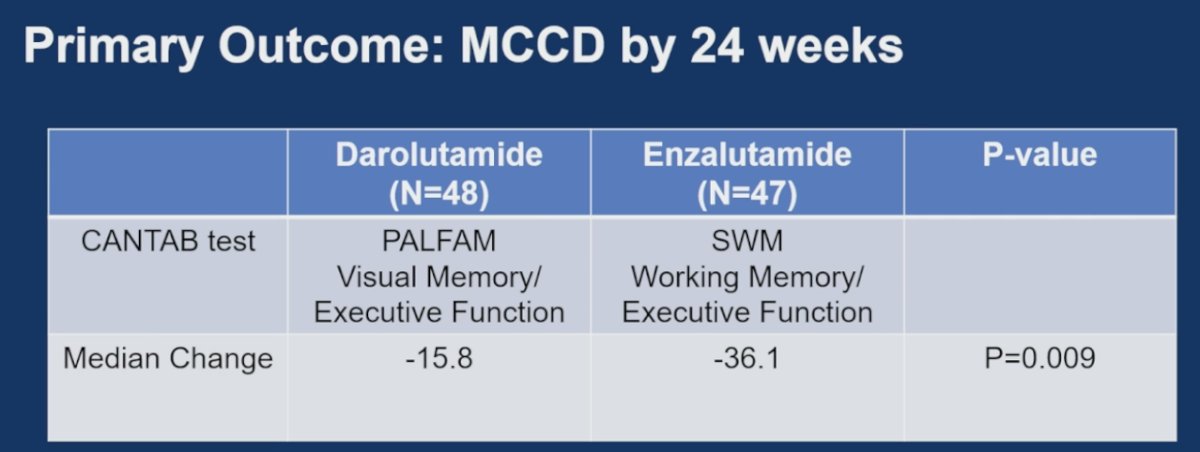
The primary endpoint analysis demonstrated a significantly greater decline in cognitive performance with enzalutamide compared with darolutamide by 24 weeks. In the darolutamide arm, the maximally changed cognitive domain was visual memory/executive function assessed through the PALFAM CANTAB module, with a median change of -15.8. In contrast, patients receiving enzalutamide experienced a substantially larger decline in working memory/executive function measured through the SWM module, with a median change of -36.1 (p=0.009). Overall, treatment with enzalutamide was associated with significantly greater deterioration in cognitive function compared with darolutamide. The investigators also noted that patients who crossed over prior to 24 weeks were analyzed according to their cognitive score at the time of crossover within their originally randomized treatment arm.
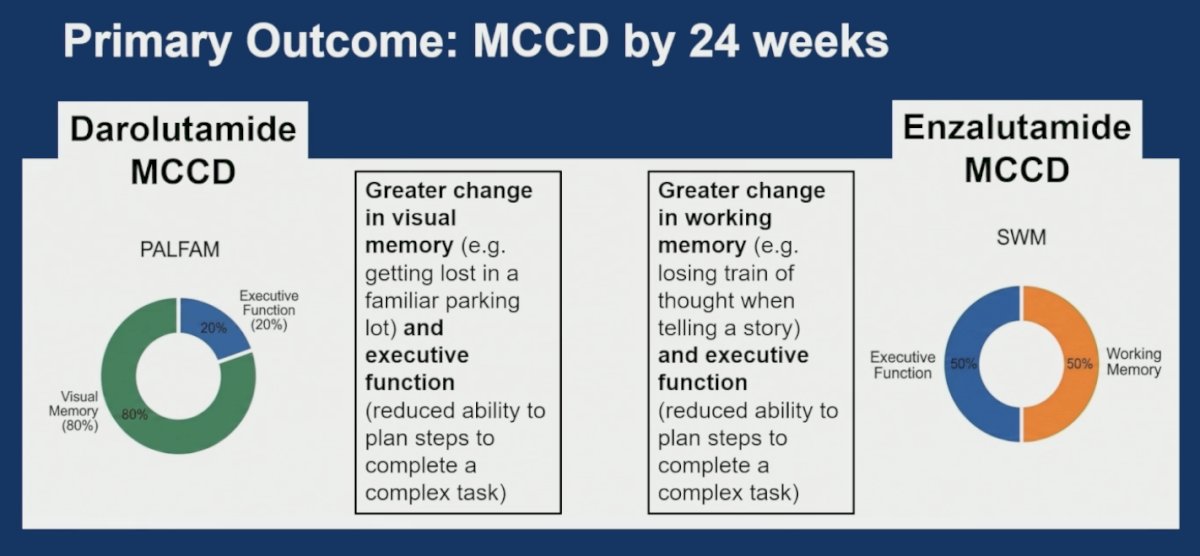
Moreover, Dr. Morgans highlighted that the cognitive domains most affected differed between treatment arms. In patients receiving darolutamide, the maximally changed cognitive domain was primarily visual memory with some contribution from executive function, reflecting challenges such as becoming disoriented in familiar environments or difficulty organizing and planning complex tasks. In contrast, patients treated with enzalutamide experienced greater changes in working memory and executive function, including difficulty maintaining a train of thought during conversation or reduced ability to sequentially complete complex tasks. These findings further supported distinct neurocognitive profiles between the two ARPIs.
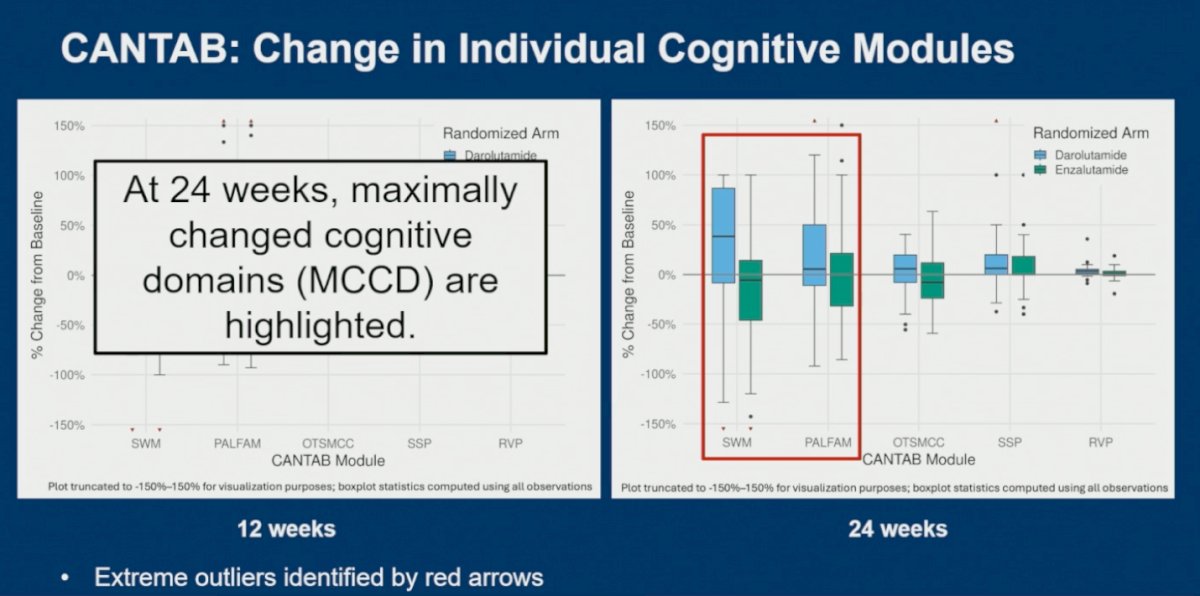
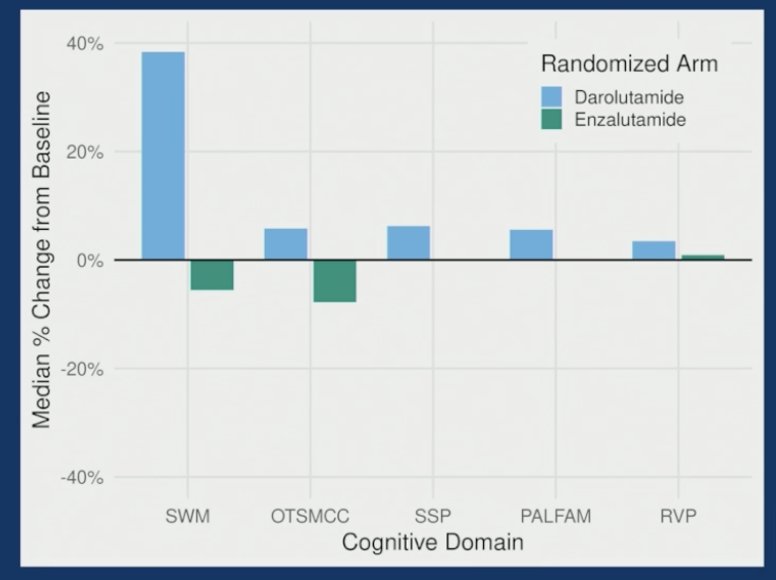
Analysis of individual CANTAB cognitive modules at both 12 and 24 weeks demonstrated consistent differences between treatment arms favoring darolutamide across several domains. By 24 weeks, the maximally changed cognitive domains became more clearly apparent, particularly within the SWM and PALFAM modules highlighted on the slide, corresponding to working memory, visual memory, and executive function domains. Patients receiving enzalutamide generally experienced larger declines from baseline across these domains, with the differences becoming more pronounced over time, suggesting cumulative neurocognitive effects. The investigators also highlighted several extreme outliers, marked by red arrows, emphasizing the substantial interpatient variability in cognitive responses to ARPI therapy.
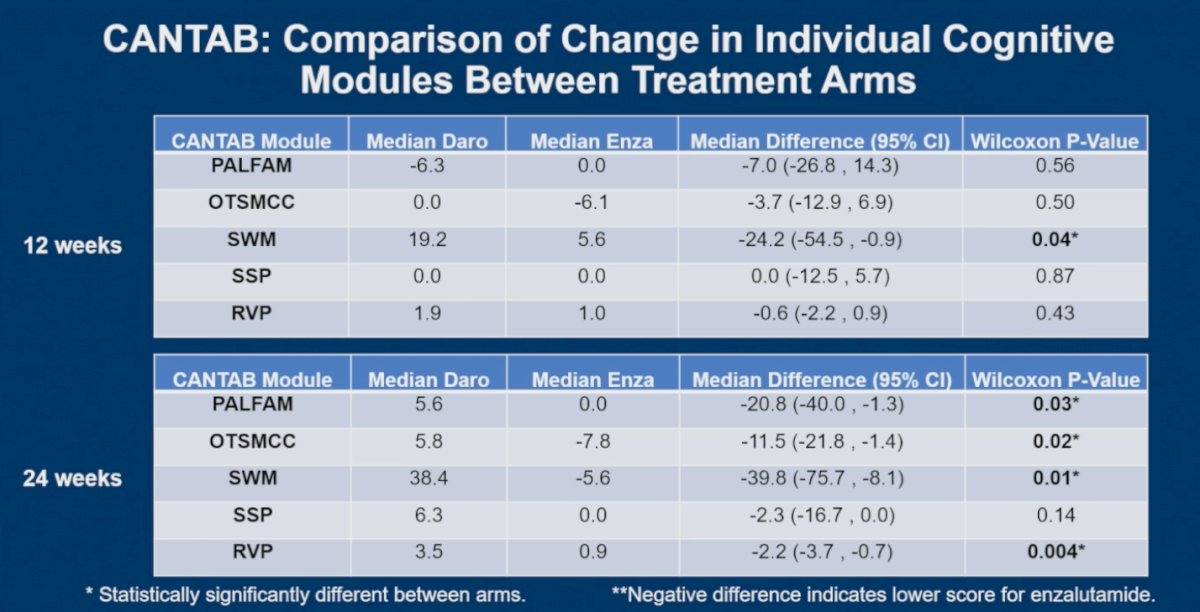
Numeric comparisons across individual CANTAB modules demonstrated progressively greater cognitive differences between treatment arms over time. At 12 weeks, statistically significant differences were primarily observed in the SWM module, assessing working memory and executive function, favoring darolutamide (median difference -24.2, p=0.04). By 24 weeks, these differences became substantially more pronounced, with 4 of the 5 evaluated CANTAB modules demonstrating statistically significant differences favoring the darolutamide arm. Significant improvements with darolutamide were observed in PALFAM (visual memory/executive function, p=0.03), OTSMCC (executive function/planning, p=0.02), SWM (working memory/executive function, p=0.01), and RVP (attention, p=0.004). Negative median differences consistently reflected worse cognitive performance in the enzalutamide arm, further supporting a differential neurocognitive effect between these ARPIs.
Furthermore, Dr. Morgans discussed the important concept of the “learning effect” in serial cognitive testing. She explained that with repeated exposure to the same cognitive assessments over time, patients with stable cognitive function are generally expected to perform better simply because they become more familiar with the testing process, not because they are becoming cognitively “smarter.” As a result, stable test scores during repeated testing may actually represent subtle cognitive decline, since patients without impairment would typically demonstrate some degree of improvement from practice effects alone.
Dr. Morgans further highlighted differences in the expected learning effect between treatment arms at 24 weeks. Patients treated with darolutamide demonstrated increased median test scores across multiple CANTAB domains between baseline and 24 weeks, consistent with preservation of the normal learning effect and stable cognitive function over time. In contrast, patients receiving enzalutamide showed stable or decreased median test scores across several domains, suggesting loss of the expected learning effect and potential decline in cognitive performance. The most pronounced differences were observed in the SWM domain, with smaller but consistent trends across executive function, visual memory, and attention-related modules.
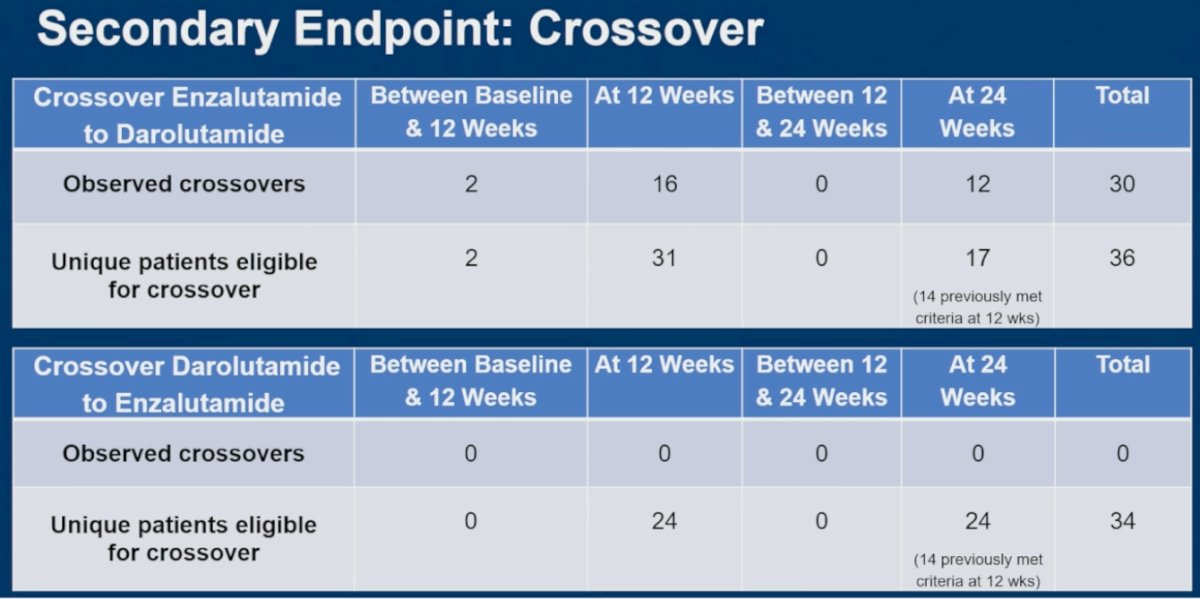
Although a relatively similar number of patients in both treatment arms met eligibility criteria for crossover, crossover behavior differed substantially between therapies. A total of 36 patients receiving enzalutamide became eligible to cross over to darolutamide, and 30 ultimately did so, including 16 at the 12-week assessment and 12 at 24 weeks. In contrast, while 34 patients receiving darolutamide met eligibility criteria for crossover to enzalutamide, no patients elected to switch therapies. These findings suggest that patients treated with enzalutamide were considerably more likely to experience cognitive or neurologic changes significant enough to motivate treatment crossover.
Lastly, Dr. Morgans acknowledged several important limitations of the ARACOG study. She noted that enzalutamide was provided through standard-of-care pathways rather than directly through the trial, which may have influenced crossover behavior and treatment decisions. In addition, eligibility criteria required that all patients have acceptable copayment amounts for enzalutamide, highlighting the real-world financial barriers that frequently impact treatment access and patient participation but are often difficult to fully account for in clinical research.
She further emphasized that the study was conducted exclusively at United States academic medical centers, although regional and satellite sites operating under academic center IRBs also enrolled patients. The overall study population was predominantly White, limiting broader generalizability. Importantly, most Black patients and patients reporting other racial backgrounds, including Asian or not reported categories, were randomized to the enzalutamide arm, introducing potential imbalance between treatment groups.
Dr. Morgans concluded her presentation with the following key takeaway points:
- This randomized phase 2 trial investigated a primary endpoint of change in cognitive testing scores between patients receiving enzalutamide versus darolutamide for advanced prostate cancer.
- There was a significantly greater decline in objectively assessed cognitive function for patients treated with enzalutamide when compared with darolutamide over 24 weeks.
- Although a similar number of patients were eligible for crossover by 24 weeks, only patients treated with enzalutamide crossed to the other treatment.
Presented by: Alicia K. Morgans, MD, MPH, Dana Farber Cancer Institute, Boston, MA
Written by: Julian Chavarriaga, MD, Clinical Assistant Professor, Urologic Oncologist, Department of Urology at Penn State Health @chavarriagaj on X during the American Society of Clinical Oncology Genitourinary (ASCO) Annual Meeting held in Chicago, IL between May 29th and June 1st, 2026
Related content: Comparing Cognitive Change on Enzalutamide and Darolutamide in the ARACOG Trial - Alicia Morgans