(UroToday.com) The 2026 American Society of Clinical Oncology Genitourinary (ASCO) Annual Meeting held in Chicago, IL, was host to the Prostate, Testicular, and Penile Cancer - Oral Abstracts. Dr. Joshua M. Lang discussed how to apply new biomarkers in clinical practice.
Dr. Lang began his presentation with the following key takeaway messages from the three trials that he is going to discuss:
- Risk stratification in newly diagnosed prostate cancer continues to evolve through the integration of both genomic classifiers and germline genetic testing approaches.
- Circulating miRNAs represent a promising emerging opportunity in germ cell tumors, with the ability to be identified in plasma and associated with recurrence risk.
- Additional prospective biomarker-driven clinical trials are critically needed to better define and validate the clinical utility of these biomarkers in routine practice.
Dr. Lang began by highlighting the revolutionary therapeutic advances that have transformed the management landscape for newly diagnosed prostate cancer over the last decade. He emphasized that treatment paradigms for hormone-sensitive prostate or now androgen pathway-sensitive metastatic prostate cancer (HSPC/APMS) have rapidly evolved from androgen deprivation therapy (ADT) alone toward increasingly intensified multimodal strategies. In patients with locally advanced disease, combination approaches incorporating radiation therapy with ADT and androgen receptor pathway inhibitors (ARPIs) have become increasingly integrated into clinical practice, while the metastatic setting has seen the emergence of both doublet and triplet therapy approaches that significantly improve clinical outcomes.
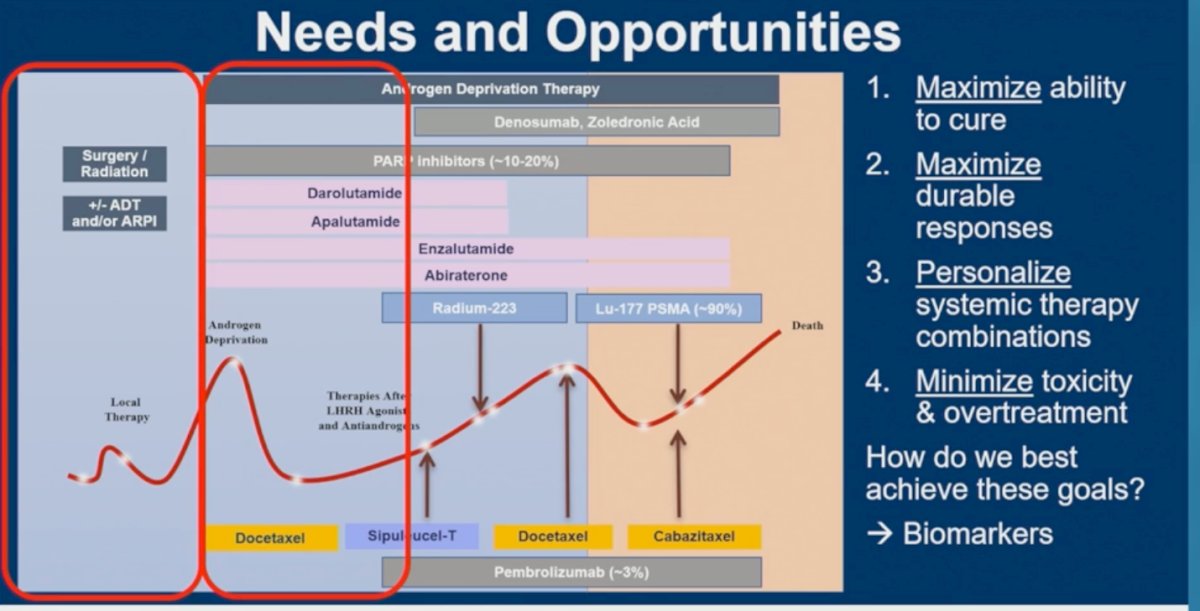
He subsequently reviewed the projected treatment landscape for 2026, emphasizing the growing complexity of therapeutic sequencing across the disease continuum. Current management now incorporates multiple androgen receptor pathway inhibitors, docetaxel, PARP inhibitors in selected patients, radioligand therapies such as Lu-177 PSMA, immunotherapy, bone-targeted agents, and other emerging systemic therapies. Dr. Lang noted that clinicians often have only one opportunity to deliver the optimal therapy early in the disease course, underscoring the critical need for improved biomarker-driven treatment selection. He also stressed that genomics alone should not be conflated with broader genetic testing strategies, while tissue-based panel testing for homologous recombination repair alterations and tumor suppressor loss is increasingly becoming part of standard-of-care evaluation.
Dr. Lang subsequently outlined four major needs and opportunities shaping the future management of HSPC/APMC. These included maximizing the potential for cure through earlier and more effective integration of local and systemic therapies, maximizing the durability of treatment responses across the disease continuum, personalizing systemic therapy combinations using biologically informed approaches, and minimizing treatment-related toxicity and overtreatment. He emphasized that achieving these goals will require the development and integration of more effective biomarkers capable of guiding therapeutic decision-making throughout the course of disease.
He emphasized that when uncertainty exists regarding the clinical utility of biomarkers, clinicians should listen carefully to the questions patients themselves are asking. These discussions frequently center on whether a biomarker can provide prognostic information, identify the most effective therapy, guide surveillance strategies, or potentially lead to inappropriate treatment decisions. He highlighted common patient concerns, including whether a test can predict survival, determine the optimal treatment approach, monitor for recurrence, and clarify how clinicians would act upon a positive result.
He subsequently noted that these same questions are increasingly shaping regulatory expectations for biomarker development. In particular, the FDA framework now focuses on defining biomarkers according to their intended clinical role, including prognostic, predictive, and monitoring applications, while also emphasizing the importance of rigorous clinical validation, diagnostic accuracy, and clinically meaningful negative and positive predictive values.
Abstract 5000: Clinico-transcriptomic risk stratification to guide abiraterone treatment intensification in high-risk prostate cancer: A combined analysis of NRG/RTOG 9202, 9413, 9902, and 0521He subsequently discussed Dr. Patel’s presentation and the use of the Decipher Prostate Classifier as an integrated genomic risk stratification tool in prostate cancer. He explained that the assay is based on a 22-mRNA feature signature using a GLMNET algorithm to generate a genomic classifier score ranging from 0 to 1.0 from formalin-fixed paraffin-embedded tissue, incorporating analysis of more than 25,000 genes. He noted that higher Decipher scores correlate with progression from localized to non-localized disease and are prognostic for relapse and overall survival across both localized and metastatic settings. Additionally, the classifier has been associated with multiple KEGG biological pathways involved in cellular growth, replication, repair, transcriptional signaling, and metabolic processes, supporting its biological relevance in aggressive prostate cancer behavior.
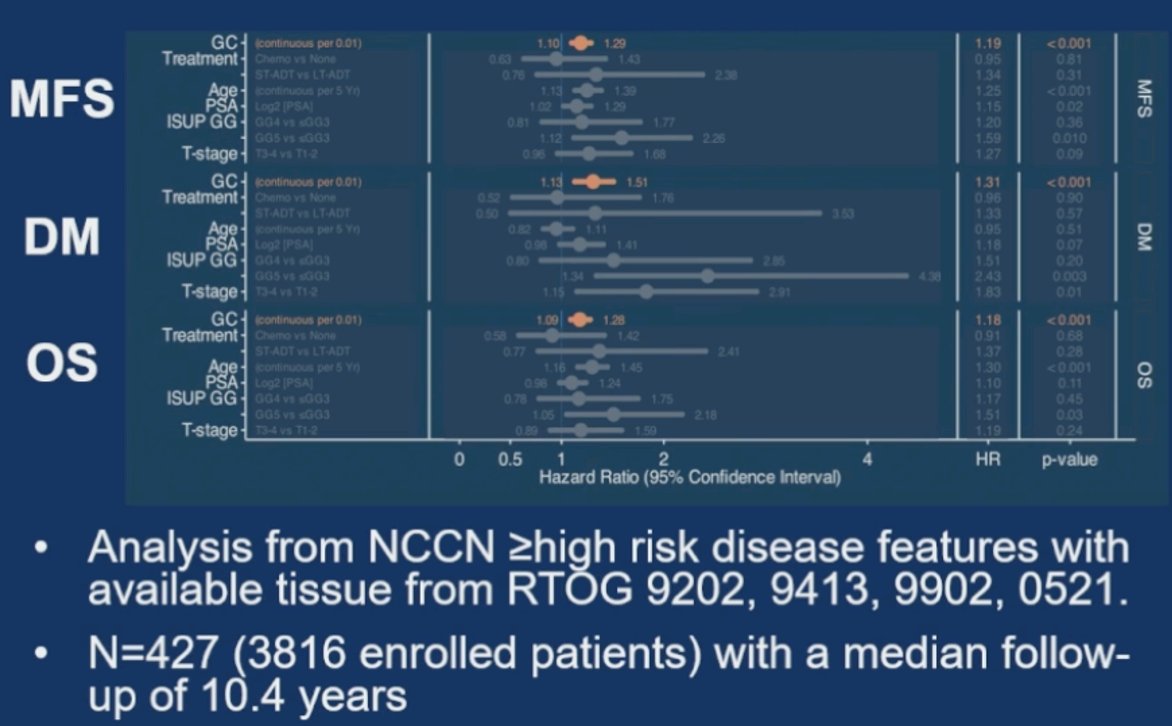
He highlighted that across multiple RTOG studies involving patients with NCCN high-risk localized prostate cancer, the Decipher genomic classifier consistently demonstrated prognostic utility across key oncologic endpoints, including metastasis-free survival, distant metastasis, and overall survival. This analysis included patients from RTOG 9202, 9413, 9902, and 0521 with available tissue specimens, representing 427 patients from a total enrollment population of 3,816 patients and a median follow-up of 10.4 years.1
However, he also emphasized several important limitations of these analyses. Notably, only approximately 11% of enrolled patients had tissue available for genomic analysis, raising concerns regarding significant loss of statistical power and potential selection bias related to sites that retained tissue specimens. He additionally questioned whether these findings should be interpreted as truly predictive for abiraterone benefit, given that these historical trials predated current standards of care and did not administer contemporary treatment intensification approaches.
He emphasized that these are critically important questions for the field and specifically applauded the investigators for thoughtfully acknowledging these limitations and uncertainties within their own analyses. In particular, he highlighted that discordant clinical and biomarker results emerged in approximately 24% of patients included in the report, raising important questions regarding whether this rate is truly representative of the broader trial population or instead reflects the smaller subset of patients with available tissue specimens. He further noted that these historical trials did not incorporate androgen receptor pathway inhibitors, limiting direct applicability to current standards of care that increasingly rely on treatment intensification strategies. As such, he cautioned against overextending the interpretation of models trained on older therapeutic paradigms and distinct patient populations outside their intended context of use.
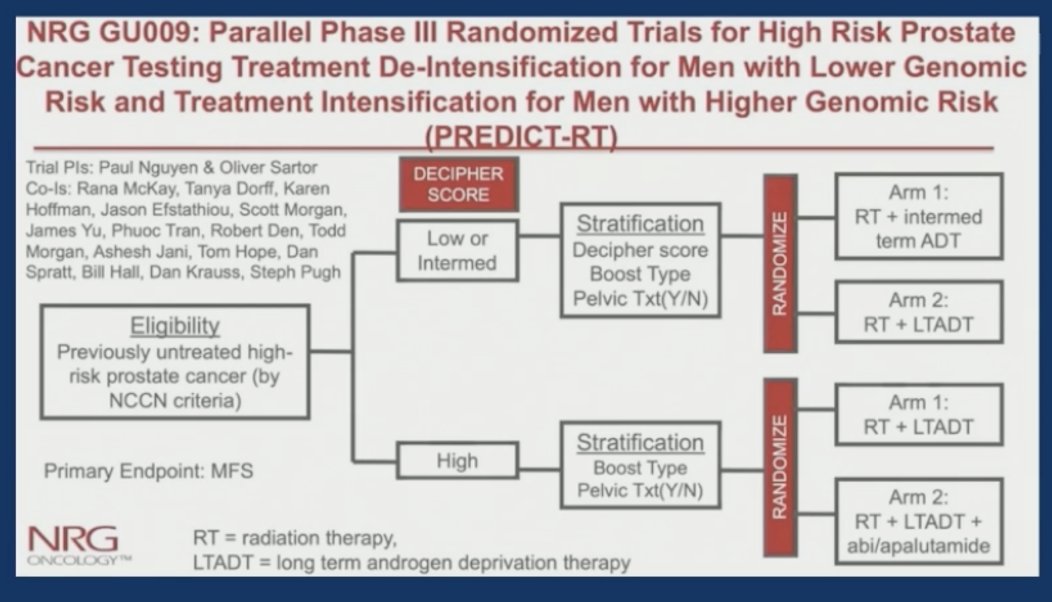
He also highlighted the importance of the ongoing NRG-GU009 (PREDICT-RT) trial as a critical next step in defining the true clinical utility of genomic classifiers in high-risk prostate cancer. He noted that while current clinical decision support tools can integrate prognostic biomarkers and statistical modeling may suggest potential treatment strategies, these approaches alone do not establish clinical utility or actionability. Importantly, PREDICT-RT prospectively randomizes patients according to Decipher genomic classifier risk groups and evaluates different therapeutic intensification or de-intensification strategies based on biomarker status. Patients with low or intermediate genomic risk undergo randomization between radiation therapy plus intermediate-term ADT versus radiation therapy plus long-term ADT, whereas patients with high genomic risk are randomized to radiation therapy plus long-term ADT with or without additional abiraterone/apalutamide intensification. He emphasized that randomized prospective validation through studies such as NRG-GU009 will ultimately determine how these biomarker-driven approaches should be incorporated into routine clinical practice.
Dr. Patel transitioned to discuss the presentation evaluating AI-inferred spatial gene expression from routine H&E pathology slides to predict docetaxel benefit in metastatic hormone-sensitive prostate cancer within the CHAARTED/E3805 dataset. He described this as a fascinating and rapidly evolving technology, emphasizing that only a few years ago many of these analyses would have seemed aspirational, whereas they are now becoming technically feasible and clinically relevant. The investigators developed an artificial intelligence platform capable of inferring spatial gene expression directly from routine H&E images and subsequently trained and validated the model using samples from the CHAARTED trial.2
He noted that these approaches have the potential to dramatically expand access to biologically informed treatment selection without requiring costly or tissue-intensive genomic assays. However, he also emphasized the importance of carefully evaluating the broader generalizability of these models, particularly when algorithms are trained on specific clinical trial populations and historical treatment paradigms that may differ from contemporary practice.
Dr Patel discussed the statistical and methodological framework used for feature selection within the CHAARTED training cohort. The model was trained specifically in patients receiving ADT alone and incorporated low-variance feature filtering, univariate Cox screening for overall survival, correlation pruning, and bootstrap LASSO-Cox stability selection to identify the 10 most informative features incorporated into the final model. Importantly, feature filtering, model selection, and threshold determination were locked prior to external evaluation in the validation cohort treated with ADT plus docetaxel. He emphasized that while this approach evaluated numerous biologically relevant prostate cancer genes and generated granular biologic information across multiple gene sets, important questions remain regarding limited assessment of proliferation signatures and the broader generalizability of the model to patients with high-volume or high-risk disease outside the original CHAARTED population.
He then reviewed what he described as one of the most clinically relevant findings from the study, namely the ability of the ST-DoxPCa biomarker to identify patients most likely to benefit from the addition of docetaxel. Among biomarker-positive patients, the addition of docetaxel to ADT was associated with a significant improvement in survival outcomes, with a hazard ratio of 0.526 (95% CI 0.307-0.902; p=0.018). In contrast, biomarker-negative patients did not appear to derive meaningful benefit from docetaxel intensification, with no significant survival improvement observed (HR 1.319, 95% CI 0.743-2.342; p=0.343).
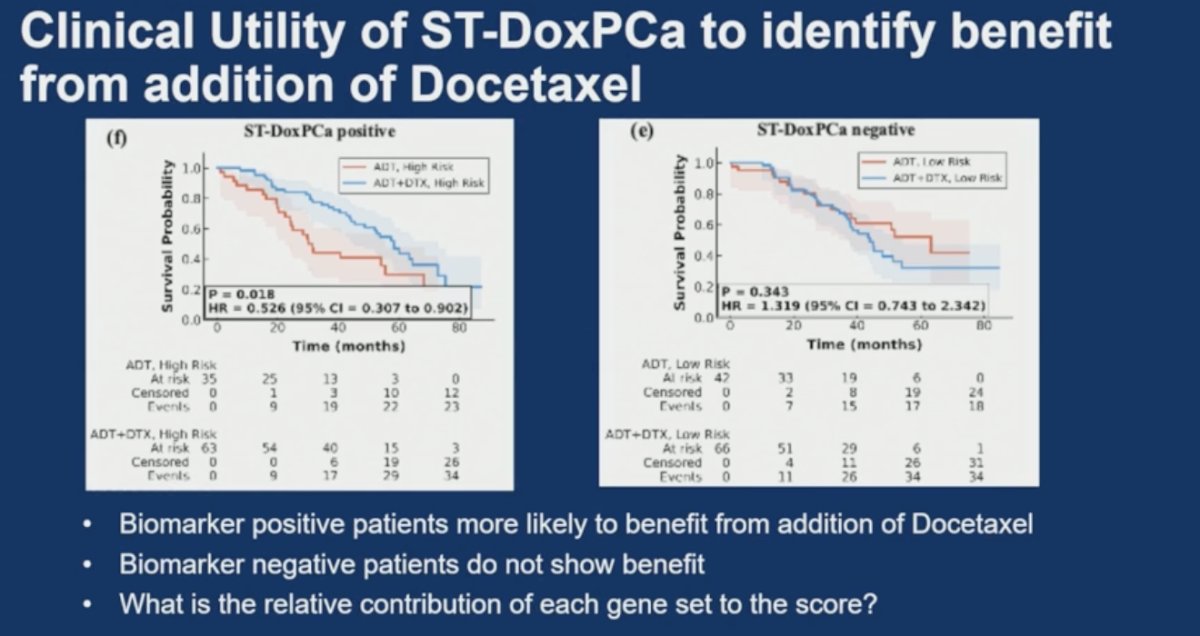
He emphasized that these findings highlight the potential clinical utility of AI-derived spatial transcriptomic biomarkers to guide treatment selection and potentially spare selected patients from unnecessary chemotherapy-related toxicity. At the same time, he raised important biologic questions regarding the relative contribution of each individual gene set and pathway to the final composite biomarker score, underscoring the need for additional mechanistic validation and prospective clinical testing.
Dr Lang concluded, discussing this abstract with the following thoughts:
- What is the absolute clinical benefit required to reliably predict response, and how do we appropriately transition biomarkers from prognostic tools to truly predictive assays?
- A positive interaction test in a retrospective study supports the potential predictive utility of the biomarker, but does not definitively establish or confirm predictive capability.
- Pathology slides were available for only approximately 36% of patients enrolled in CHAARTED, raising concerns regarding selection bias and broader applicability.
- Disease volume was not prognostic within this analyzed subset, differing from the findings observed in the overall CHAARTED study population.
- ADT plus docetaxel is no longer the contemporary standard of care in metastatic hormone-sensitive prostate cancer, emphasizing the importance of validating these findings within modern treatment intensification paradigms and other clinical contexts.
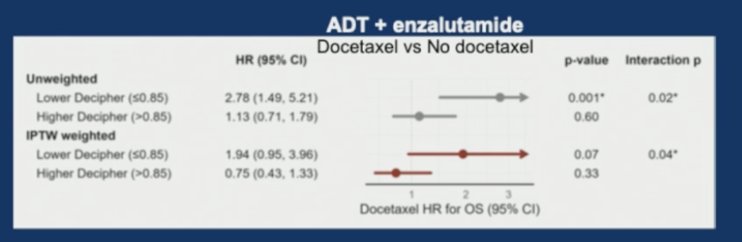
Dr. Lang then discussed the abstract presented by Dr. Sweeney, evaluating the ability of the Decipher Prostate Metastatic Classifier to identify patients who may benefit from the addition of docetaxel to androgen deprivation therapy plus enzalutamide within the ENZAMET study.3 The ENZAMET study schema and biomarker analysis are shown below.
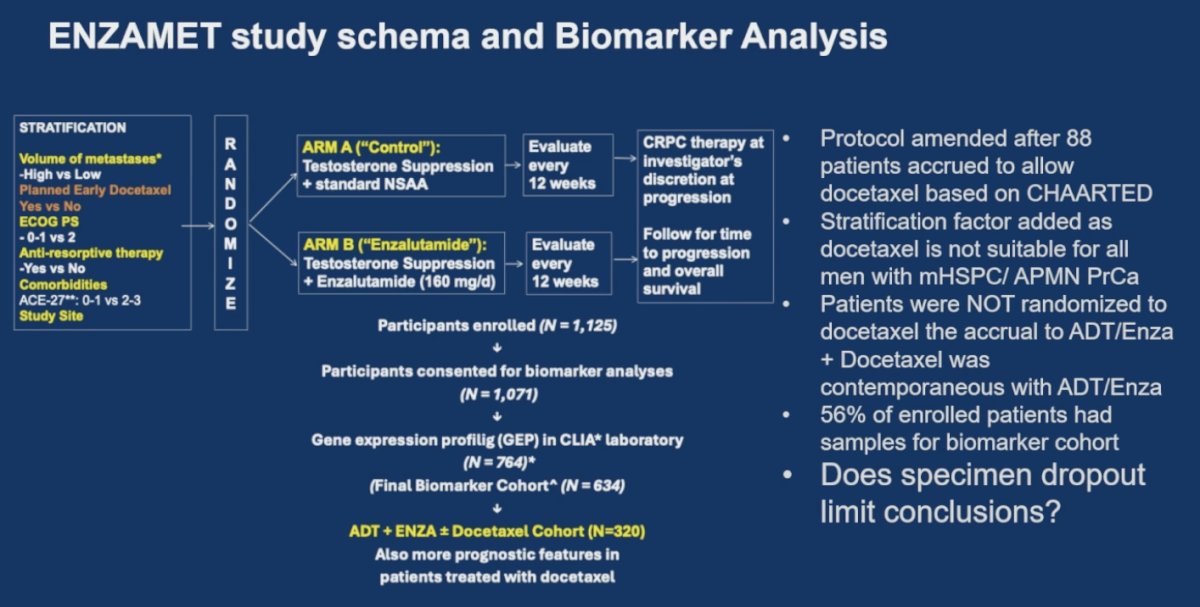
He highlighted several important considerations regarding the interpretation of the study. Notably, the protocol was amended after 88 patients had accrued in order to allow docetaxel administration based on emerging CHAARTED data. A stratification factor was subsequently added, recognizing that docetaxel may not be suitable for all men with metastatic hormone-sensitive prostate cancer. Importantly, patients were not randomized specifically to docetaxel, and the accrual of patients receiving ADT plus enzalutamide with docetaxel occurred contemporaneously rather than through a dedicated randomized comparison. He also emphasized that only 56% of enrolled patients had available samples for the biomarker cohort analysis, raising important concerns regarding specimen dropout and the extent to which this may limit the strength and generalizability of the study conclusions.
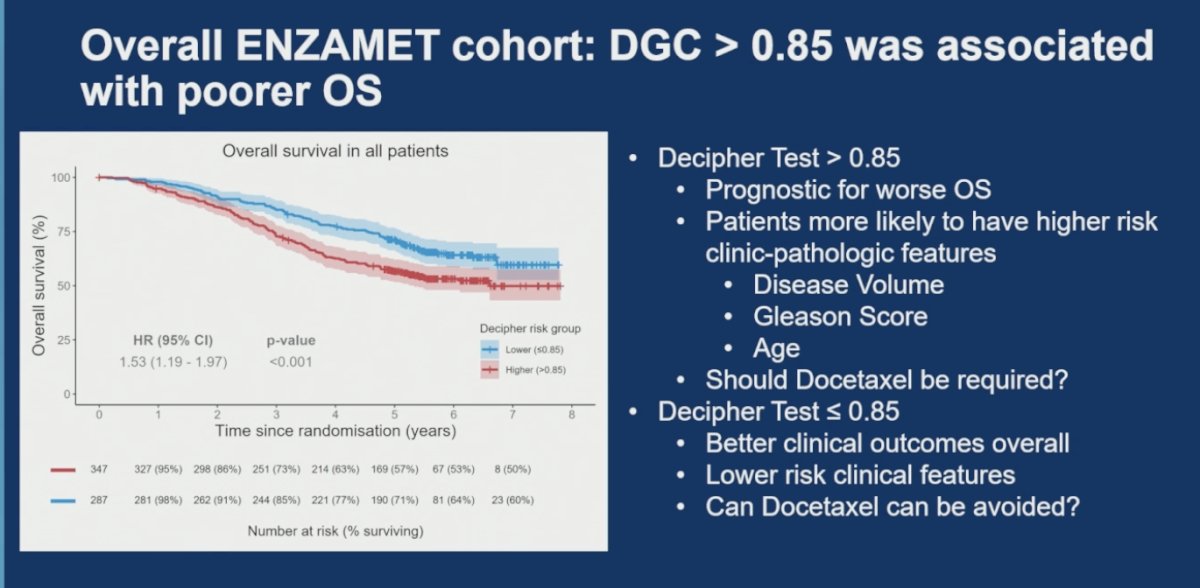
Dr. Lang emphasized the importance of these findings, noting that the ENZAMET analysis further confirms the prognostic utility of the Decipher Genomic Classifier in advanced prostate cancer. Specifically, patients with a Decipher score >0.85 demonstrated significantly worse overall survival compared with patients with lower scores (HR 1.53, 95% CI 1.19-1.97; p<0.001). He also highlighted that patients with high Decipher scores were more likely to harbor adverse clinicopathologic features, including higher disease volume, higher Gleason score, and older age. Conversely, patients with Decipher scores ≤0.85 demonstrated more favorable clinical outcomes and lower-risk disease characteristics overall. He noted that these findings raise important clinical questions regarding which patients truly require docetaxel intensification and whether some lower-risk patients may potentially avoid chemotherapy.
Moreover, he highlighted a particularly unexpected observation from the ENZAMET biomarker analysis. Among patients with lower Decipher scores (≤0.85), those treated with intensified triplet therapy consisting of ADT, enzalutamide, and docetaxel demonstrated worse overall survival compared with patients treated with ADT plus enzalutamide alone (HR 3.02, 95% CI 1.59-5.76; p<0.001). He noted that patients receiving triplet therapy within this subgroup were more likely to have high-volume disease and older age, raising the possibility of important selection bias within the cohort.
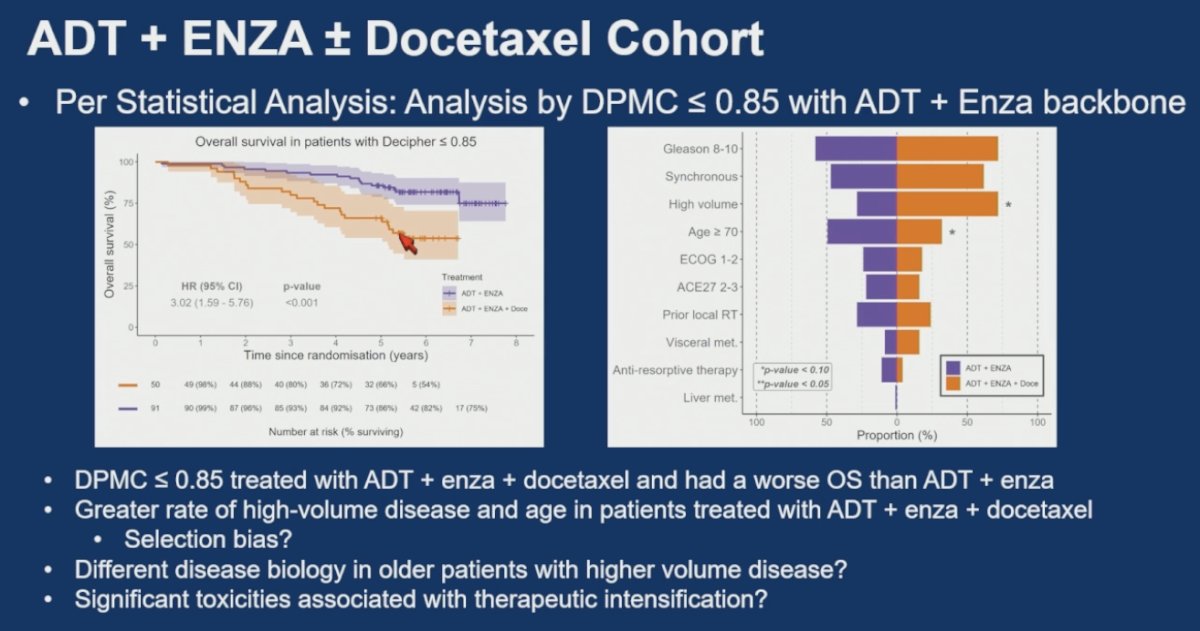
He further questioned whether these findings may reflect differences in underlying disease biology among older patients with higher-volume disease rather than a true detrimental effect of docetaxel itself. Additionally, he raised the possibility that the observed outcomes may partially reflect treatment-related toxicity associated with therapeutic intensification. Overall, he emphasized that these data reinforce the complexity of distinguishing prognostic from truly predictive biomarker information in advanced prostate cancer.
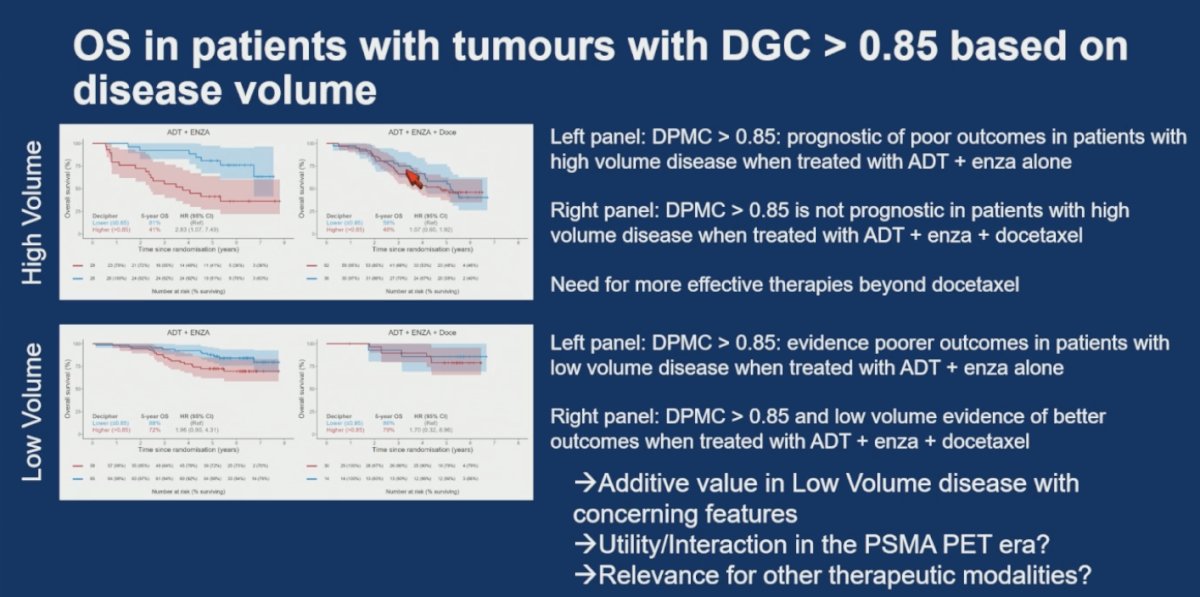
He then discussed the disease volume subgroup analyses, emphasizing both the potential utility and limitations of docetaxel intensification. In patients with high-volume disease and DPMC >0.85, the classifier remained prognostic for poor outcomes when patients received ADT plus enzalutamide alone, whereas this adverse prognostic effect was less apparent among those treated with docetaxel. However, he noted that approximately 20% of patients still progressed to CRPC within less than 2 years, highlighting the limitations of docetaxel itself and the need for more effective therapeutic strategies beyond chemotherapy.
He also highlighted the potential additive value of DPMC in patients traditionally categorized as low-volume disease. In this subgroup, DPMC >0.85 appeared to identify patients with poorer outcomes when treated with ADT plus enzalutamide alone, suggesting that genomic risk may help identify clinically concerning biology even among patients otherwise considered low volume. He raised several important questions, including whether these findings remain relevant in the PSMA PET era, whether similar interactions apply to other therapeutic modalities, and how best to identify low-volume patients whose clinical or genomic features should prompt treatment intensification.
Lastly, Dr. Lang emphasized the importance of carefully interpreting the statistical methodology used in the ENZAMET biomarker analyses. He highlighted that the investigators performed multiple statistical adjustments, including multivariable analyses (MVA) and inverse probability of treatment weighting (IPTW), in an effort to account for the contribution of known clinical factors influencing outcomes. However, rather than focusing solely on traditional p-values, he stressed the importance of understanding the interaction p-value, as this is more relevant when evaluating whether a biomarker may truly predict differential treatment benefit.
He further cautioned that population-level statistical corrections do not automatically translate into actionable patient-level decisions in clinical practice. Importantly, he noted that even sophisticated statistical adjustments cannot substitute for prospective randomized clinical trials specifically designed to test biomarker-guided treatment strategies.
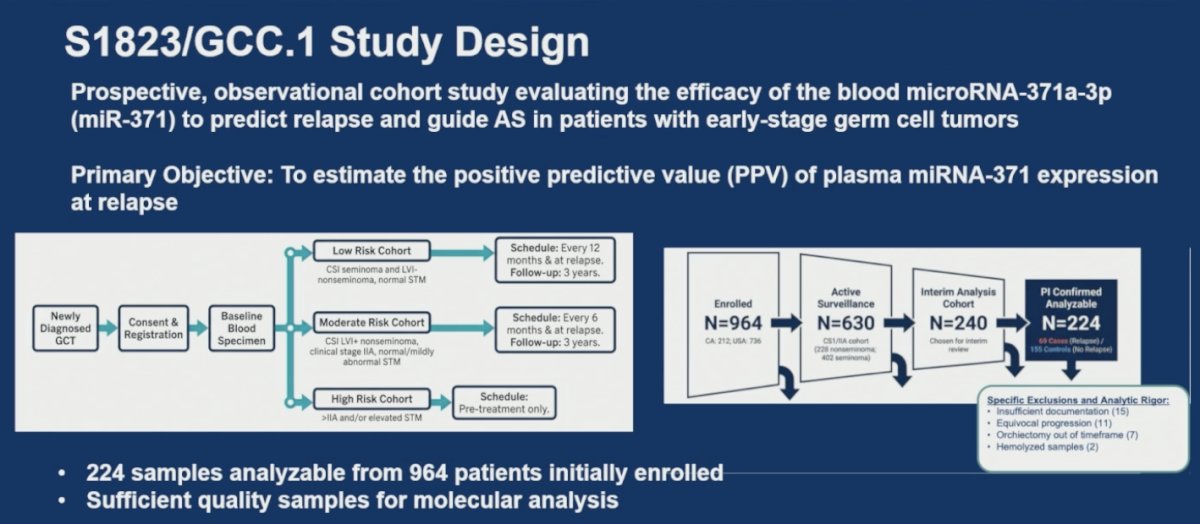
Dr. Lang also reviewed the SWOG S1823/GCC.1 study presented by Dr. Nappi, a prospective observational cohort study evaluating plasma microRNA-371a-3p (miR-371) as a biomarker to predict relapse and potentially guide active surveillance strategies in patients with early-stage germ cell tumors. The primary objective of the study was to estimate the positive predictive value of plasma miR-371 expression at the time of relapse. He highlighted the prospective and real-world nature of the study, which enrolled patients across both Canada and the United States.
The study stratified patients into low-, moderate-, and high-risk cohorts based on their pre-test probability of relapse, with different surveillance schedules and sample acquisition protocols across groups. Importantly, only the low- and moderate-risk cohorts contributed to the primary endpoint analysis. Among the 964 patients initially enrolled, 630 patients underwent active surveillance, and an interim analysis cohort of 240 patients was selected for review. Ultimately, 224 samples were deemed PI-confirmed and analyzable, including 69 relapse cases and 155 controls without relapse. He emphasized that adequate sample quality and rigorous molecular analysis were critical aspects of the study design, with exclusions occurring due to insufficient documentation, equivocal progression, orchiectomy timing issues, and hemolyzed samples.
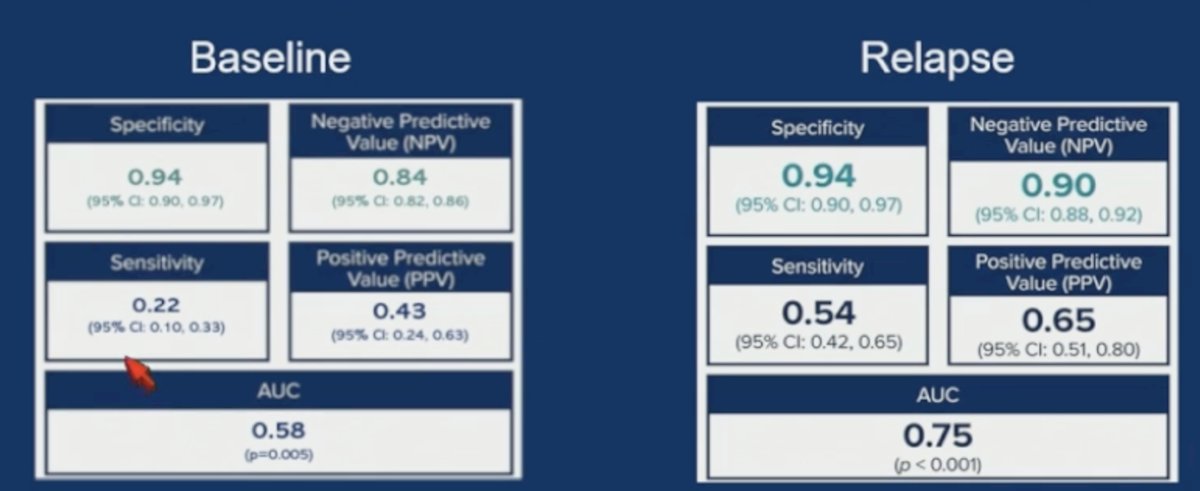
He noted that one of the most important observations from the study was the relatively low sensitivity of miR371 at baseline, although performance improved substantially at the time of relapse. Specifically, baseline sensitivity was 22% with an AUC of 0.58, whereas at relapse, sensitivity increased to 54% with an AUC of 0.75. Despite this, specificity remained impressively high at both baseline and relapse (94%), with a false-positive rate of only 6% (10/155 controls), the majority of whom were low-risk patients.
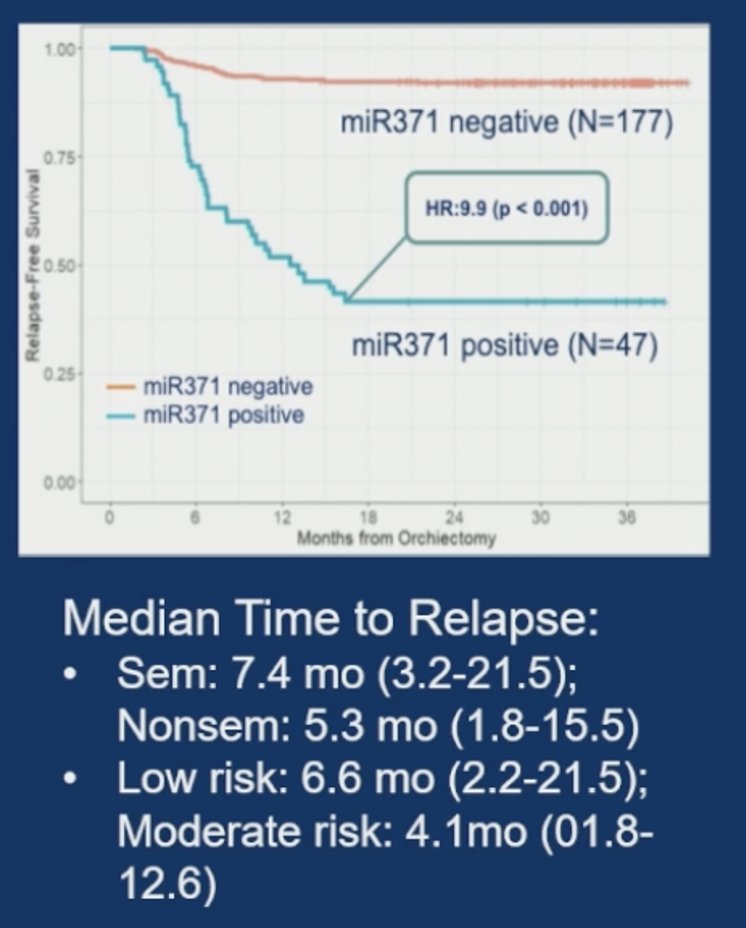
He also highlighted the significant difference in relapse-free survival according to baseline miR371 status, with miR371-positive patients experiencing markedly worse outcomes (HR 9.9; p<0.001).
Dr. Lang emphasized several important clinical questions raised by these findings. While the high specificity and NPV are encouraging, he questioned whether the observed NPV is sufficient to guide treatment-level decisions in routine practice. He also discussed the potential role of miR371 in scenarios with equivocal imaging findings, where additional biomarker information may aid clinical interpretation. Importantly, he stressed that prospective clinical trials remain essential to determine which specific clinical decisions this biomarker is best suited to address, including surveillance imaging frequency, treatment escalation, or therapeutic intervention strategies.
Lastly, Dr. Lang concluded by returning to the key questions his patients commonly ask regarding biomarker testing and personalized treatment selection in prostate cancer. He noted that current biomarkers clearly provide strong prognostic information and can help estimate clinical outcomes. However, he emphasized that these assays are not yet definitively predictive for selecting the optimal therapy for individual patients.
He further discussed the ongoing uncertainty surrounding how biomarkers should influence recurrence monitoring and subsequent treatment decisions. While these tests may eventually help guide imaging strategies or identify patients who could benefit from newer therapies, these applications remain incompletely defined. Finally, he acknowledged an important concern frequently raised by patients: whether biomarker-guided decision-making could potentially lead to the wrong treatment choice. He emphasized that this question remains unresolved and highlights the continued need for prospective biomarker-driven clinical trials.
Presented by: Joshua M. Lang, MD, MS, Vice Chair for Biomedical Research, Department of Medicine, Carbone Cancer Center, The University of Wisconsin
Written by: Julian Chavarriaga, MD, Clinical Assistant Professor, Urologic Oncologist, Department of Urology at Penn State Health @chavarriagaj on X during the American Society of Clinical Oncology Genitourinary (ASCO) Annual Meeting held in Chicago, IL between May 29th and June 1st, 2026
References:- Nguyen PL, Huang HR, Spratt DE, Davicioni E, Sandler HM, Shipley WU, Efstathiou JA, Simko JP, Pollack A, Dicker AP, Roach M, Rosenthal SA, Zeitzer KL, Mendez LC, Hartford AC, Hall WA, Desai AB, Rabinovitch RA, Peters CA, Rodgers JP, Tran P, Feng FY. Analysis of a Biopsy-Based Genomic Classifier in High-Risk Prostate Cancer: Meta-Analysis of the NRG Oncology/Radiation Therapy Oncology Group 9202, 9413, and 9902 Phase 3 Randomized Trials. Int J Radiat Oncol Biol Phys. 2023 Jul 1;116(3):521-529. doi: 10.1016/j.ijrobp.2022.12.035. Epub 2022 Dec 31. PMID: 36596347; PMCID: PMC10281690.
- Sweeney CJ, Chen YH, Carducci M, Liu G, Jarrard DF, Eisenberger M, Wong YN, Hahn N, Kohli M, Cooney MM, Dreicer R, Vogelzang NJ, Picus J, Shevrin D, Hussain M, Garcia JA, DiPaola RS. Chemohormonal Therapy in Metastatic Hormone-Sensitive Prostate Cancer. N Engl J Med. 2015 Aug 20;373(8):737-46. doi: 10.1056/NEJMoa1503747. Epub 2015 Aug 5. PMID: 26244877; PMCID: PMC4562797.
- Sweeney CJ, Martin AJ, Stockler MR, Begbie S, Cheung L, Chi KN, Chowdhury S, Frydenberg M, Horvath LG, Joshua AM, Lawrence NJ, Marx G, McCaffrey J, McDermott R, McJannett M, North SA, Parnis F, Parulekar W, Pook DW, Reaume MN, Sandhu SK, Tan A, Tan TH, Thomson A, Vera-Badillo F, Williams SG, Winter D, Yip S, Zhang AY, Zielinski RR, Davis ID; ENZAMET trial investigators and Australian and New Zealand Urogenital and Prostate Cancer Trials Group. Testosterone suppression plus enzalutamide versus testosterone suppression plus standard antiandrogen therapy for metastatic hormone-sensitive prostate cancer (ENZAMET): an international, open-label, randomised, phase 3 trial. Lancet Oncol. 2023 Apr;24(4):323-334. doi: 10.1016/S1470-2045(23)00063-3. PMID: 36990608.