(UroToday.com) The 2026 American Society of Clinical Oncology Genitourinary (ASCO) Annual Meeting held in Chicago, IL, was host to the Prostate, Testicular, and Penile Cancer - Oral Abstracts. Dr. Krishnan R. Patel presented Abstract 5000: Clinico-transcriptomic risk stratification to guide abiraterone treatment intensification in high-risk prostate cancer: A combined analysis of NRG/RTOG 9202, 9413, 9902, and 0521.
Dr. Patel began by posing a practical clinical question focused on whether a simple algorithm could help busy clinicians integrate clinical and genomic biomarker data to better inform treatment decision-making for men with high-risk prostate cancer. He emphasized the growing complexity of treatment selection in the modern era, where clinicians are increasingly challenged to synthesize traditional clinicopathologic risk factors alongside emerging genomic classifiers and molecular biomarkers in routine practice.
Dr. Patel began his presentation with a clinical case of a 70-year-old man with newly diagnosed very high-risk prostate cancer, including cT3aN0M0 disease on DRE, ISUP Grade Group 5 histology, and a PSA of 41 ng/mL. He framed the discussion around a common real-world clinical question from both physicians and patients: “Doctor, what should I do?”
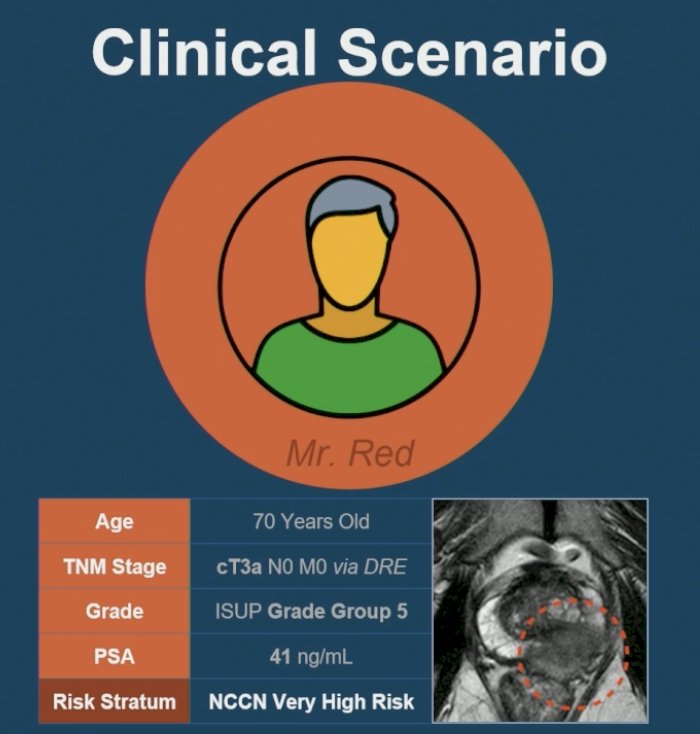
He noted that based on NCCN guidelines, this patient meets criteria for very high-risk disease, for which radiation therapy plus long-term ADT and abiraterone intensification would represent a guideline-supported standard approach, largely informed by data from the STAMPEDE platform trial.1
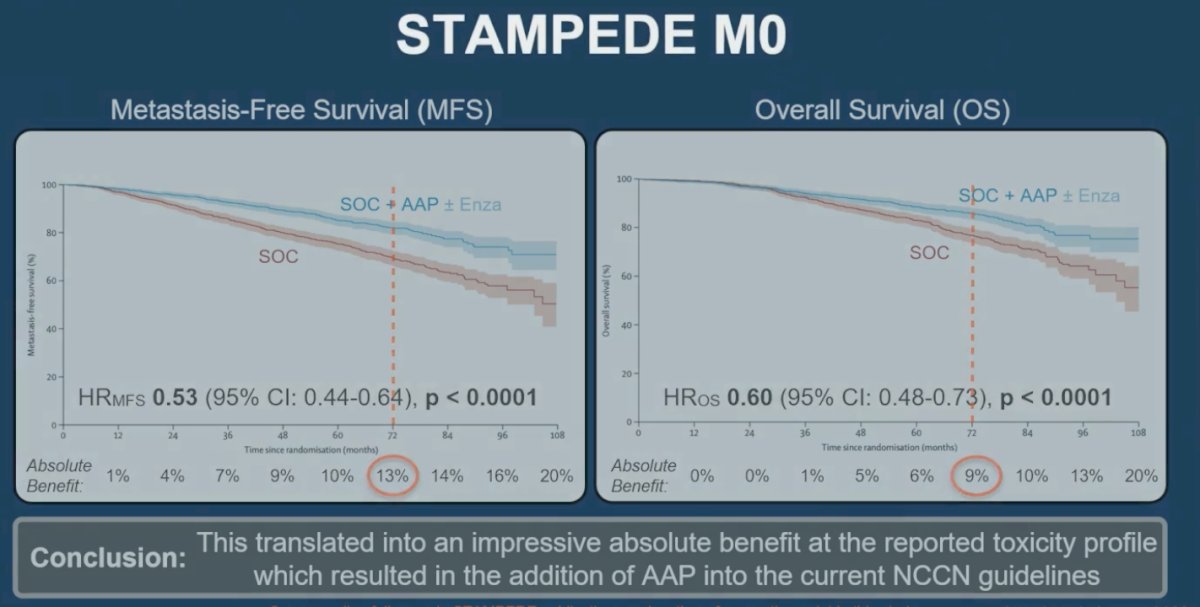
Dr. Patel noted that the rationale for treatment intensification in selected patients with non-metastatic high-risk prostate cancer is largely driven by data from the STAMPEDE M0 population. He reviewed the trial design, which included patients with node-positive disease or those with at least two high-risk features, including cT3-4 disease, Gleason score 8-10, or PSA ≥40 ng/mL, who were randomized to receive radiation therapy plus ADT with or without abiraterone-based intensification.1
He highlighted the significant improvement observed with treatment intensification across both metastasis-free survival and overall survival endpoints. In the metastasis-free survival analysis, the addition of abiraterone with or without enzalutamide to SOC resulted in a 47% reduction in the risk of metastasis or death (HR 0.53, 95% CI 0.44-0.64; p<0.0001). Importantly, the red-highlighted area on the Kaplan-Meier curve demonstrated an absolute metastasis-free survival benefit of 13% at approximately 72 months. Similarly, in the overall survival analysis, intensified therapy was associated with a 40% reduction in the risk of death compared with SOC alone (HR 0.60, 95% CI 0.48-0.73; p<0.0001). The red-highlighted portion of the curve illustrated an absolute overall survival benefit of 9% at 72 months.1 Dr. Patel emphasized that these clinically meaningful benefits ultimately led to the incorporation of abiraterone-based intensification into current NCCN guideline recommendations for selected patients with very high-risk localized disease.
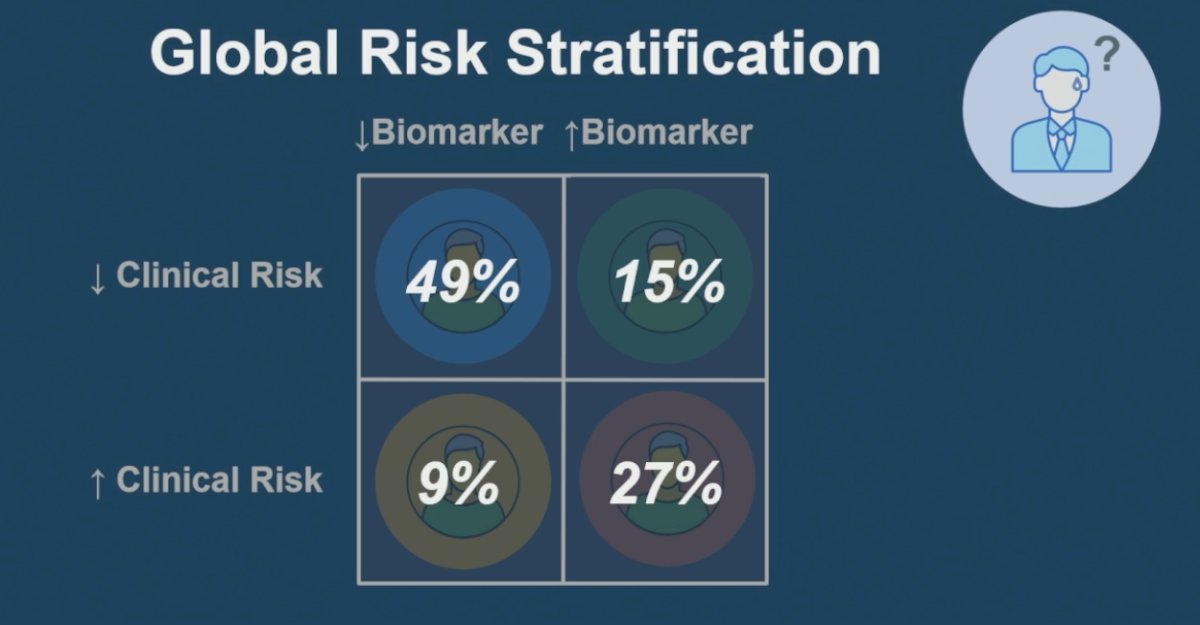
Dr. Patel then highlighted a common real-world dilemma in treatment selection by presenting a similar patient with clinically very high-risk disease who would traditionally be recommended treatment intensification, but whose genomic classifier testing demonstrated an even more concerning biology with a GC score of 0.94. He acknowledged that in many of these scenarios, “we do not really know what the right answer is,” particularly when attempting to integrate genomic information into established clinical risk models. To conceptualize this challenge, he introduced a simple 2x2 global risk stratification framework combining clinical and biomarker risk. He noted that decision-making is generally more straightforward when clinical and genomic risk are concordant, whereas the greatest uncertainty arises in discordant cases, including patients with high clinical risk but low biomarker risk or low clinical risk with high genomic risk, which increasingly represent the major challenge in personalized prostate cancer treatment decision-making.

Dr. Patel subsequently framed the central study objective, which was to determine whether clinical and genomic classifier-based risk stratification could be combined to better guide selection of patients for abiraterone acetate plus prednisone (AAP) intensification using data derived from four mature phase III randomized clinical trials. He outlined three key study questions:
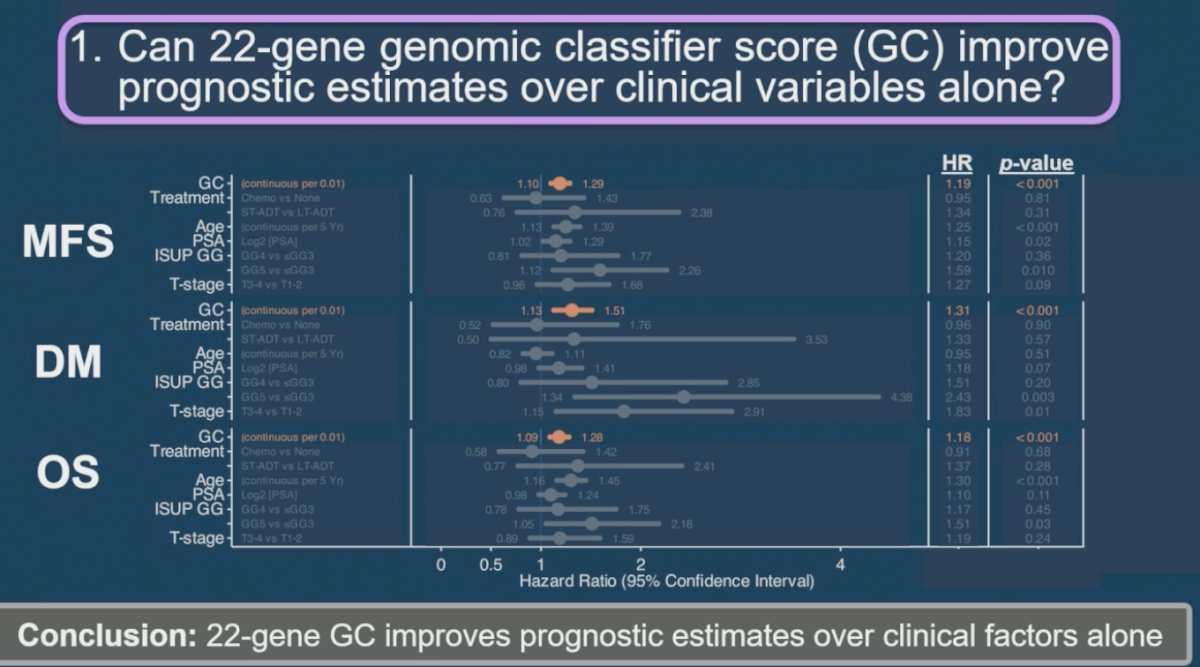
- Can the 22-gene genomic classifier (GC) improve prognostic estimates beyond clinical variables alone?
- Is there a clinically meaningful proportion of patients with discordant clinical and biomarker risk to justify further study?
- Can a simple and clinically parsimonious system be developed to help clinicians integrate clinical and genomic data into treatment recommendations?
To address the first study question, Dr. Patel demonstrated that the 22-gene genomic classifier independently improved prognostic estimates beyond clinical variables alone across multiple clinically relevant endpoints. Specifically, higher GC scores were significantly associated with worse metastasis-free survival (MFS; HR 1.19, p<0.001), distant metastasis (DM; HR 1.31, p<0.001), and overall survival (OS; HR 1.18, p<0.001). He concluded that incorporation of the genomic classifier meaningfully enhanced risk stratification beyond standard clinicopathologic factors alone.
Addressing the second study question, Dr. Patel demonstrated that a substantial proportion of patients exhibited discordance between clinical and genomic biomarker risk stratification. Using the proposed global risk framework, 15% of patients had low clinical risk but high biomarker risk, while 9% demonstrated high clinical risk despite low biomarker risk. Overall, approximately one-quarter of patients had discordant clinical and genomic features, supporting the clinical relevance of this population and justifying further study of integrated risk-adapted treatment strategies.
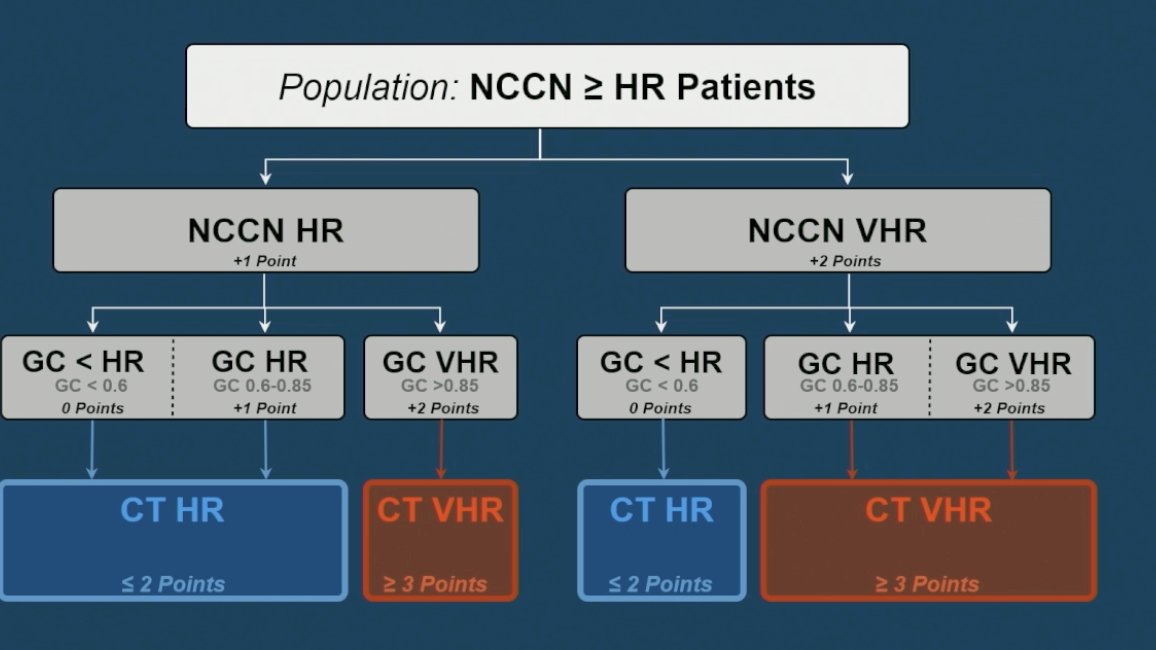
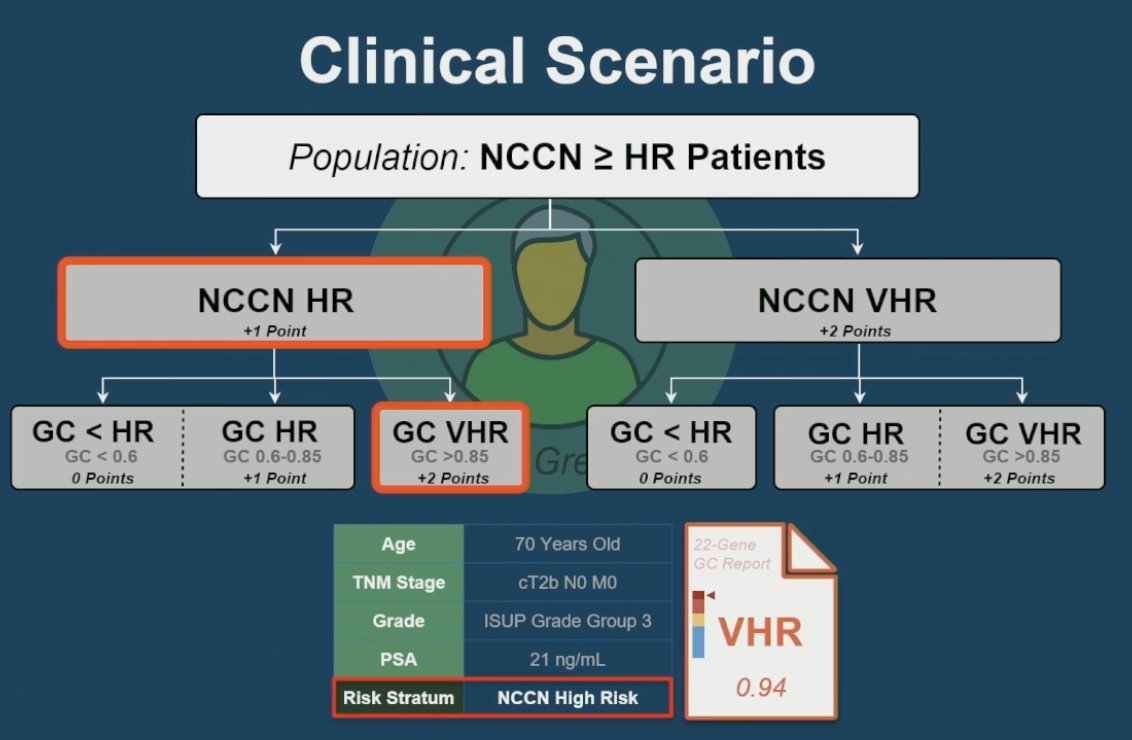
Lastly, Dr. Patel presented a simple integrated clinical-genomic algorithm designed to help clinicians incorporate both NCCN clinical risk stratification and genomic classifier (GC) results into treatment decision-making for patients with high-risk localized prostate cancer. Within this framework, patients with NCCN high-risk disease were assigned 1 point, whereas patients with NCCN very high-risk disease were assigned 2 points. Similarly, genomic classifier categories were stratified according to GC score, with GC <0.6 assigned 0 points, GC 0.6-0.85 assigned 1 point, and GC >0.85 assigned 2 points.
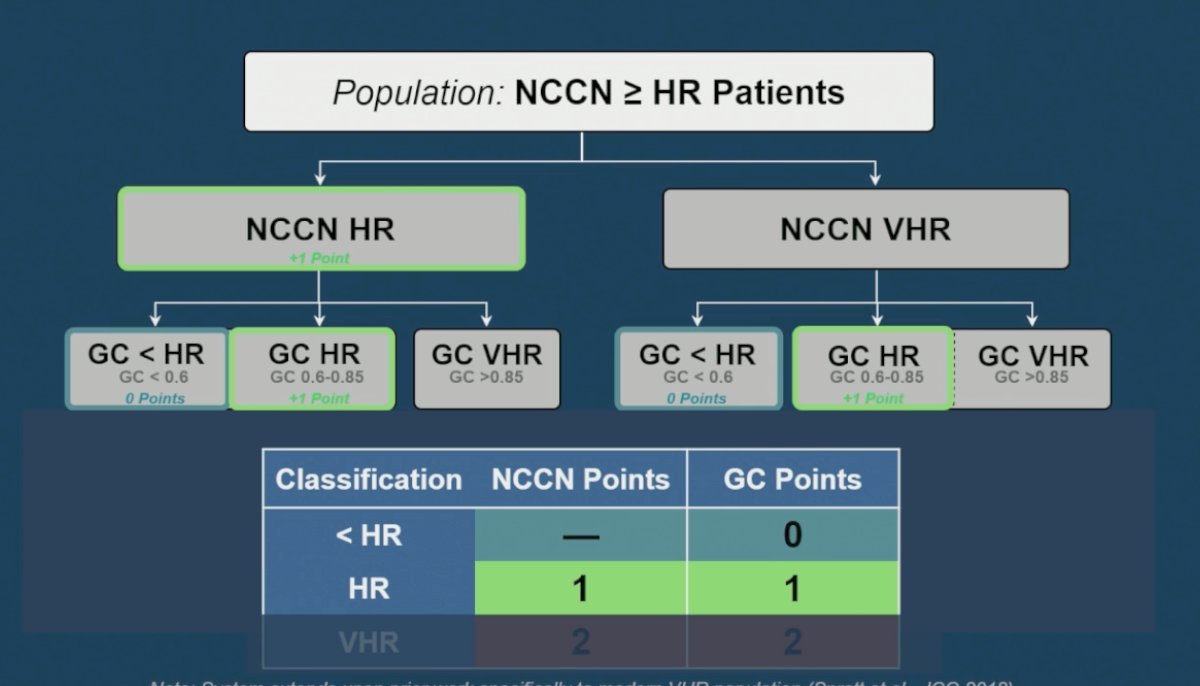
The combined score was then used to generate a clinical-transcriptomic (CT) risk classification system, in which patients with ≤2 total points were categorized as CT high-risk, while those with ≥3 points were classified as CT very high-risk. Dr. Patel emphasized that this parsimonious model may help better clarify risk among patients with discordant clinical and genomic features and provide a more practical framework for identifying patients most likely to benefit from treatment intensification strategies.
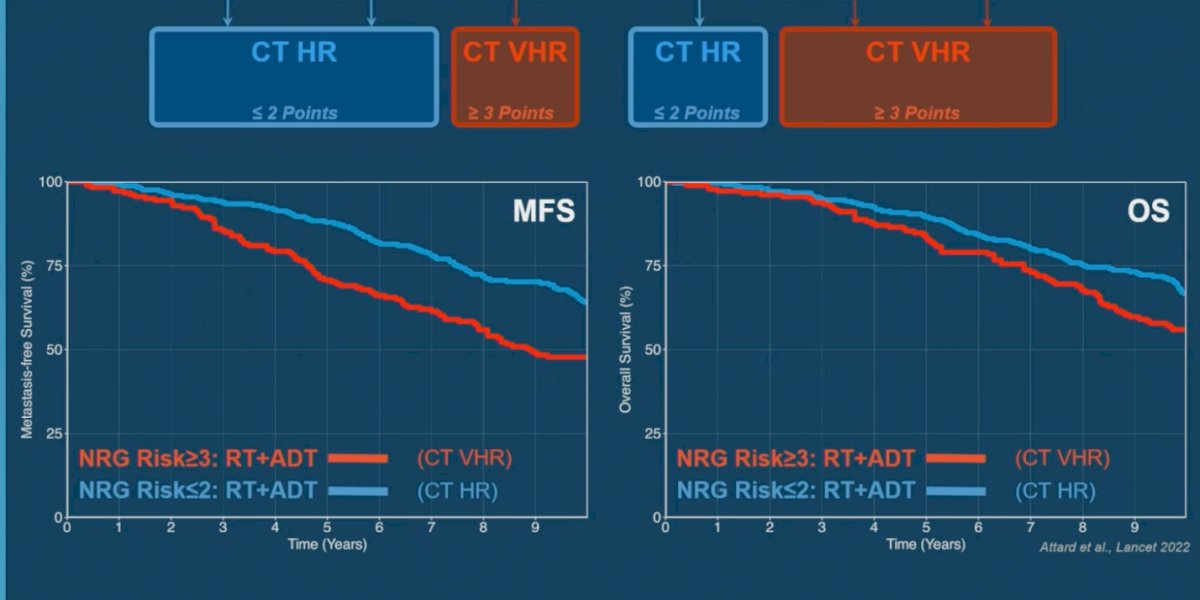
Using this integrated clinical-transcriptomic model, Dr. Patel demonstrated improved separation of patient outcomes across both metastasis-free survival and overall survival. Patients classified as CT very high-risk (CT VHR; ≥3 points) had substantially worse outcomes compared with those categorized as CT high-risk (CT HR; ≤2 points), despite all patients receiving RT plus ADT. The Kaplan-Meier curves showed clear stratification for both metastasis-free survival and overall survival, supporting the ability of the combined clinical-genomic framework to refine prognostication beyond traditional clinical risk groups alone and potentially identify patients who may derive greater benefit from treatment intensification strategies.
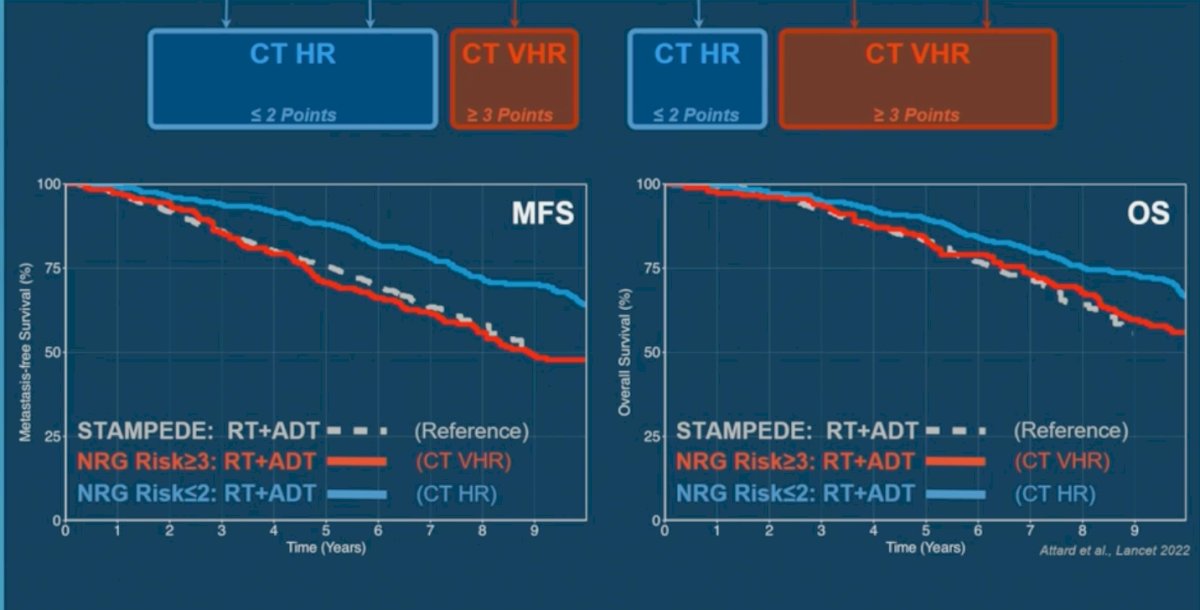
Moreover, Dr. Patel compared outcomes from this integrated clinical-transcriptomic model with the STAMPEDE benchmark population receiving RT plus ADT alone, which served as a reference cohort. Notably, patients classified as CT very high-risk (CT VHR; ≥3 risk points) demonstrated remarkably similar metastasis-free survival and overall survival outcomes compared with the STAMPEDE/NCCN very high-risk reference population. He concluded that the CT VHR classification may identify a subgroup of patients with particularly aggressive disease biology who could represent the population most likely to benefit from treatment intensification approaches such as the addition of abiraterone-based therapy.
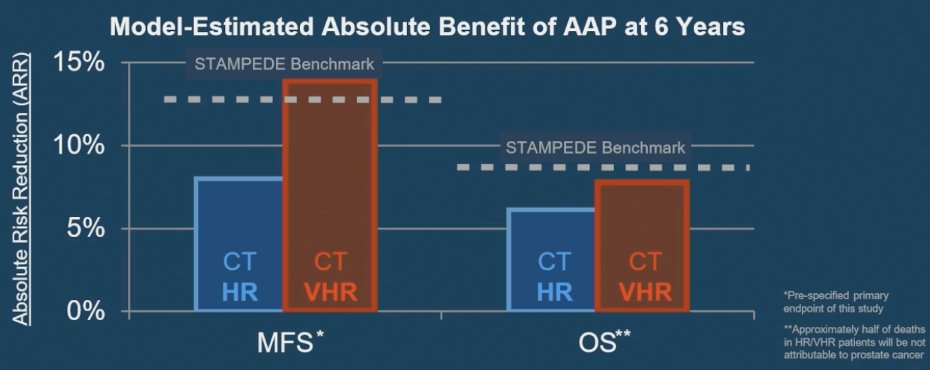
To further evaluate the clinical utility of this framework, Dr. Patel presented a model estimating the absolute benefit of AAP intensification at 6 years across the integrated clinical-transcriptomic risk groups. Patients classified as CT very high-risk demonstrated an estimated absolute metastasis-free survival benefit approaching 13% and an overall survival benefit of approximately 8%, closely mirroring the magnitude of benefit observed in the STAMPEDE/NCCN very high-risk population benchmark. In contrast, patients categorized as CT high-risk appeared to derive a more modest absolute benefit from treatment intensification. Dr. Patel concluded that the absolute benefit-to-risk ratio of AAP intensification in CT very high-risk disease is similar to that observed in the STAMPEDE/NCCN very high-risk population, further supporting the potential utility of this integrated model for treatment selection.
Dr. Patel then returned to the original clinical scenario and demonstrated how this integrated framework could directly inform treatment recommendations in practice. Although the patient met NCCN high-risk criteria clinically, the addition of a very high-risk genomic classifier result (GC 0.94) reclassified him into the clinical-transcriptomic very high-risk group. Based on this integrated risk assessment, Dr. Patel emphasized that this patient would likely represent an appropriate candidate for treatment intensification with ADT, abiraterone, and radiation therapy.
Dr. Patel concluded his presentation with the following key takeaway messages:
- The 22-gene genomic classifier improved prognostic estimates beyond clinical variables alone across metastasis-free survival, distant metastasis, and overall survival endpoints.
- Approximately one-quarter of patients demonstrated discordance between clinical and genomic classifier risk stratification, supporting the clinical relevance of integrated risk assessment approaches.
- A simple and clinically parsimonious integrated clinical-transcriptomic framework may help guide treatment intensification decisions in patients with high-risk localized prostate cancer.
- Within this proposed model, patients classified as CT high-risk (≤2 points) may be appropriately managed with radiation therapy plus ADT alone.
- In contrast, patients classified as CT very high-risk (≥3 points) may represent candidates for treatment intensification with radiation therapy, ADT, and abiraterone-based therapy.
Presented by: Krishnan R. Patel, MD, Radiation Oncology at MD Anderson Cancer Center, TX, United States.
Written by: Julian Chavarriaga, MD, Clinical Assistant Professor, Urologic Oncologist, Department of Urology at Penn State Health @chavarriagaj on X during the American Society of Clinical Oncology Genitourinary (ASCO) Annual Meeting held in Chicago, IL between May 29th and June 1st, 2026
Related content: Integrating Clinical and Genomic Risk to Guide Abiraterone Use in High-Risk Prostate Cancer - Krishnan Patel
- Attard G, Murphy L, Clarke NW, Cross W, Jones RJ, Parker CC, Gillessen S, Cook A, Brawley C, Amos CL, Atako N, Pugh C, Buckner M, Chowdhury S, Malik Z, Russell JM, Gilson C, Rush H, Bowen J, Lydon A, Pedley I, O'Sullivan JM, Birtle A, Gale J, Srihari N, Thomas C, Tanguay J, Wagstaff J, Das P, Gray E, Alzoueb M, Parikh O, Robinson A, Syndikus I, Wylie J, Zarkar A, Thalmann G, de Bono JS, Dearnaley DP, Mason MD, Gilbert D, Langley RE, Millman R, Matheson D, Sydes MR, Brown LC, Parmar MKB, James ND; Systemic Therapy in Advancing or Metastatic Prostate cancer: Evaluation of Drug Efficacy (STAMPEDE) investigators. Abiraterone acetate and prednisolone with or without enzalutamide for high-risk non-metastatic prostate cancer: a meta-analysis of primary results from two randomised controlled phase 3 trials of the STAMPEDE platform protocol. Lancet. 2022 Jan 29;399(10323):447-460. doi: 10.1016/S0140-6736(21)02437-5. Epub 2021 Dec 23. PMID: 34953525; PMCID: PMC8811484.