(UroToday.com) The 2026 American Society of Clinical Oncology Genitourinary (ASCO) Annual Meeting held in Chicago, IL, between Fri, May 29 – Tues, Jun 2, 2026, was host to the Prostate, Testicular, and Penile Cancer - Oral Abstracts. Dr. Christopher Sweeney presented Abstract 5001: Assessment of the ability of Decipher Prostate Genomic Classifier >0.85 to identify patients who benefit from adding docetaxel to ADT + enzalutamide: Level 1B evidence from the ENZAMET study.
Dr. Sweeney began his presentation by noting that major advances in treatment intensification have significantly improved survival outcomes in metastatic hormone-sensitive prostate cancer over the past decade. He highlighted that the addition of docetaxel to ADT initially demonstrated overall survival benefit primarily in patients with poorer prognostic disease, followed by subsequent studies showing that androgen receptor pathway inhibitors improved outcomes across all prognostic subgroups. More recently, further intensification strategies incorporating abiraterone or darolutamide with ADT plus docetaxel have continued to improve outcomes, with approximately 50% of men remaining alive at 8 years in the ENZAMET trial.3 However, Dr. Sweeney emphasized that despite these advances, there remain no randomized data definitively establishing the benefit of adding docetaxel to ADT plus ARPI therapy, and the value of triplet intensification in all patients remains uncertain.1,2
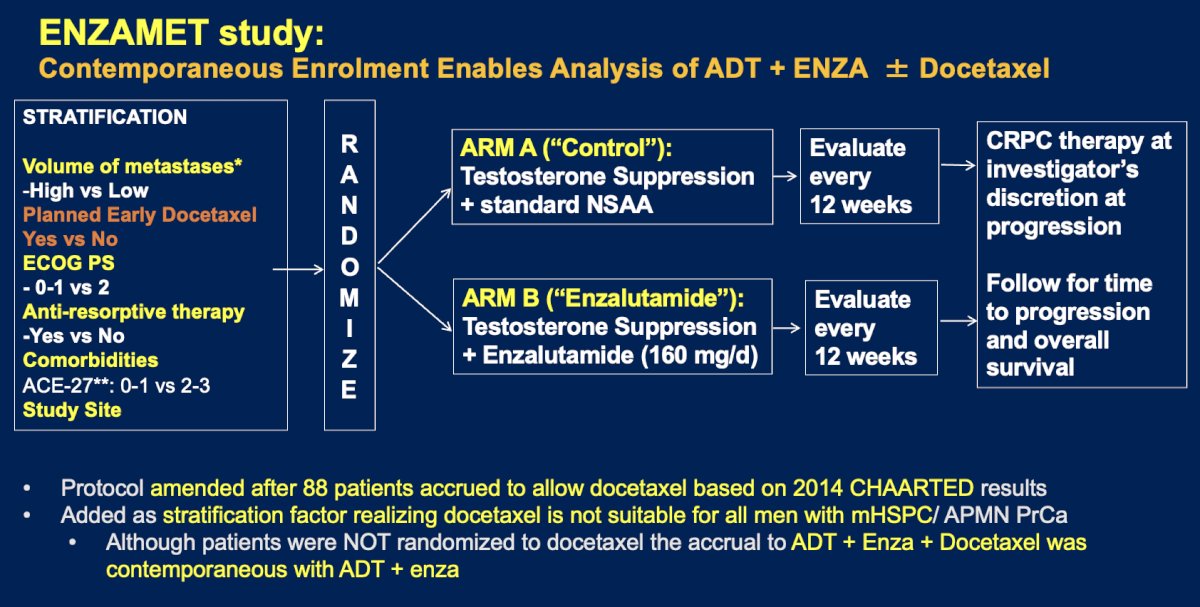
Dr. Sweeney highlighted the ENZAMET trial design, in which patients with mHSPC were randomized to receive testosterone suppression plus either a standard nonsteroidal antiandrogen or enzalutamide. The study stratified patients according to disease volume, planned early docetaxel use, ECOG performance status, antiresorptive therapy use, comorbidities, and study site. Following publication of the CHAARTED results, the protocol was amended to allow early docetaxel use, which was subsequently incorporated as a stratification factor.4 Although patients were not randomized specifically to docetaxel, the contemporaneous enrollment of patients receiving ADT plus enzalutamide with or without docetaxel enabled exploratory analyses evaluating the potential impact of triplet therapy strategies in mHSPC.
Translational analyses from CHAARTED and STAMPEDE demonstrated that the Decipher transcriptomic classifier may help identify patients most likely to benefit from treatment intensification with docetaxel. In the CHAARTED discovery cohort, patients with higher Decipher scores derived greater overall survival benefit from the addition of docetaxel to ADT (HR 0.41 for Q4), findings that were subsequently validated in the STAMPEDE cohort, where patients with high Decipher scores also experienced improved survival outcomes with ADT plus docetaxel compared with ADT alone (HR 0.64)5 as illustrated below: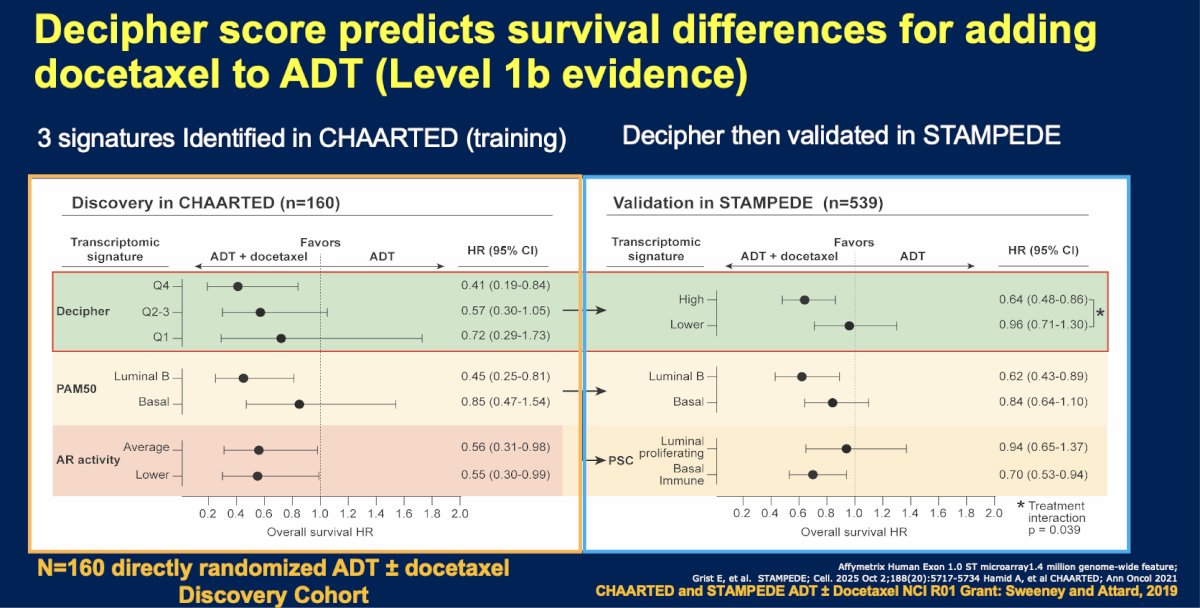
Dr. Sweeney highlighted the biological rationale behind the Decipher prostate classifier, a 22-mRNA transcriptomic signature developed using a GLMNET algorithm that generates a score ranging from 0 to 1.0 from FFPE tissue samples. Originally designed to identify aggressive biological states associated with metastatic potential, the Decipher score has been shown to increase progressively from localized to metastatic disease and to be prognostic for relapse and overall survival across disease states. Importantly, the classifier captures multiple biologic pathways implicated in prostate cancer progression, including cell growth, replication and repair, chromosomal instability, and cellular motility, supporting its potential role as both a prognostic and predictive biomarker in mHSPC.
The primary hypothesis of the study was that patients with tumors harboring a high Decipher Prostate Metastatic Classifier (DPMC >0.85) derive a survival benefit from the addition of docetaxel to ADT plus enzalutamide, independent of established clinical prognostic variables. Conversely, patients with lower-risk tumors (DPMC ≤0.85) were hypothesized to derive limited or no benefit from treatment intensification with docetaxel. Investigators also postulated that among patients treated with ADT plus enzalutamide alone, those with DPMC >0.85 would have inferior outcomes compared with those with lower DPMC scores, further supporting the prognostic and predictive role of transcriptomic risk stratification in mHSPC.
Dr. Sweeney mentioned that for the biomarker analyses, clinical and transcriptomic data from ENZAMET participants were linked through centralized tissue and RNA profiling efforts. Of the 1,125 patients enrolled in ENZAMET, 1,071 consented for biomarker analyses, with 809 samples centralized at the Chris O’Brien Lifehouse biobank for centralized H&E review. Gene expression profiling was successfully completed in a CLIA-certified laboratory for 764 samples, including 650 FFPE blocks and 114 slides, with a high average tumor content of 85.9%. The final biomarker cohort included 634 patients after exclusion of samples with poor RNA quality or insufficient tumor material.
The statistical analysis plan included a stepwise approach designed to evaluate both prognostic and predictive utility of the Decipher classifier. Initial univariable analyses were followed by multivariable modeling incorporating individual patient weighting and propensity score adjustments to account for the non-randomized use of docetaxel in ENZAMET. Investigators then tested for treatment interaction effects to assess the predictive value of the transcriptomic classifier for docetaxel benefit. Importantly, the analyses were independently designed and performed by two separate groups of statisticians to strengthen the robustness and reproducibility of the findings.
In the ENZAMET biomarker cohort, patients with high-risk tumors defined by a DPMC score >0.85 had significantly worse overall survival compared with those with lower-risk disease (HR 1.53, 95% CI 1.19–1.97; p<0.001). Clinically, patients with DPMC >0.85 were more likely to present with adverse disease characteristics, including younger age, synchronous metastatic disease, and higher Gleason grade tumors. Specifically, 75% of patients with DPMC >0.85 had synchronous metastases compared with 62% in the lower-risk group, while Gleason 8–10 disease was observed in 82% versus 59%, respectively. These findings further support the prognostic value of the Decipher metastatic classifier in patients with mHSPC as shown below: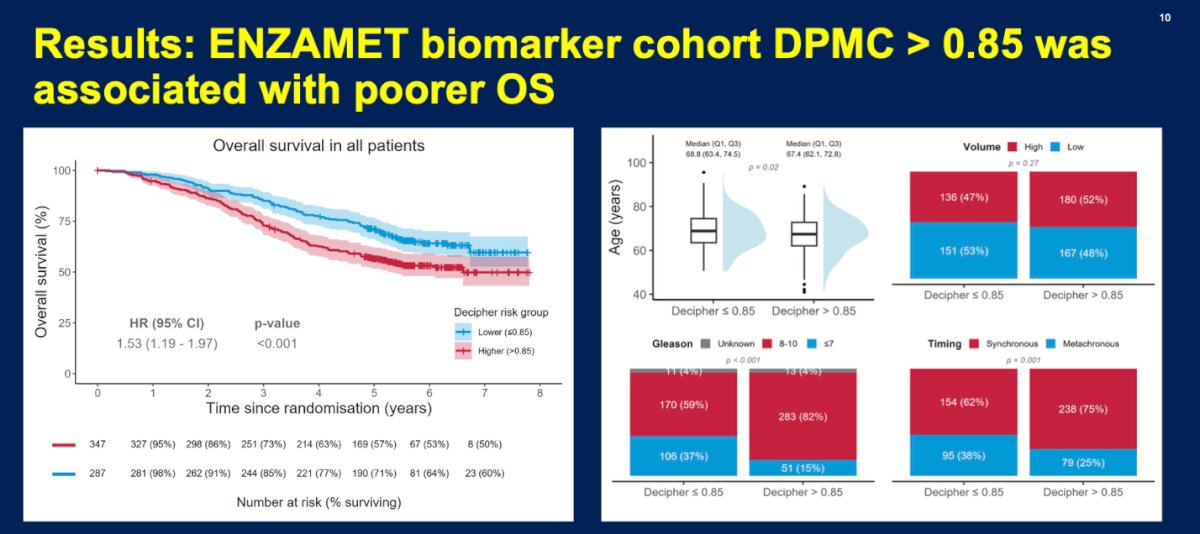
Moreover, a high DPMC score (>0.85) was consistently associated with inferior outcomes across multiple clinically relevant secondary endpoints. Patients with high-risk transcriptomic profiles experienced significantly worse progression-free survival (HR 1.50, 95% CI 1.22–1.84; p<0.001), PSA progression-free survival (HR 1.46, 95% CI 1.20–1.80; p<0.001), and higher prostate cancer-specific mortality (HR 1.71, 95% CI 1.30–2.26; p<0.001) compared with patients with DPMC ≤0.85 as shown in the Kaplan Meier curves below.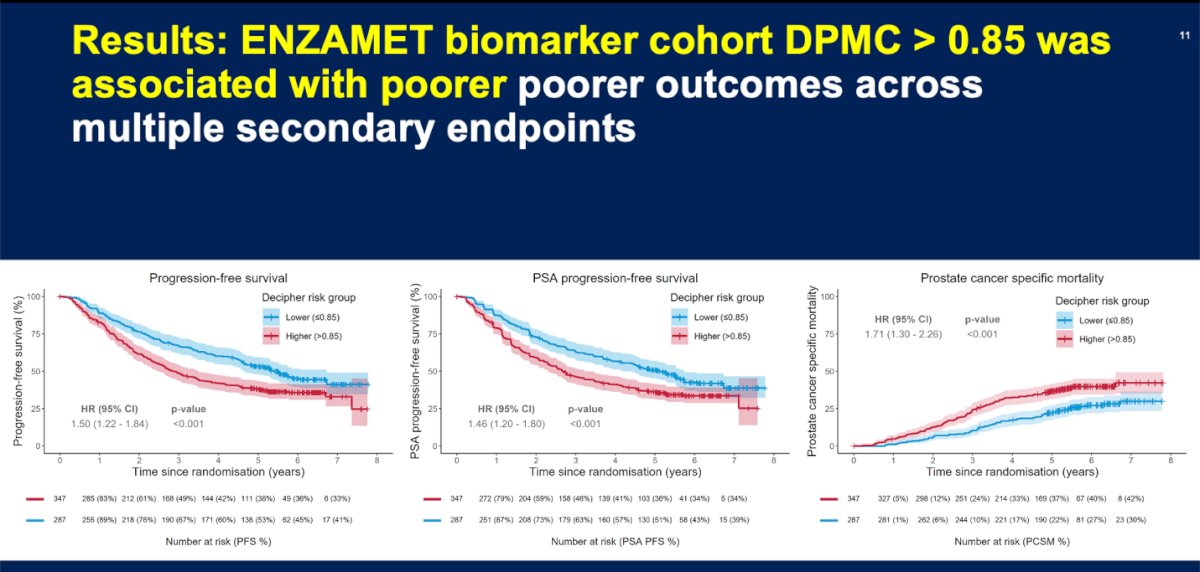
Furthermore, important baseline differences were observed between patients who received docetaxel and those who did not within the ENZAMET biomarker cohort. Patients treated with docetaxel were more likely to harbor high-risk transcriptomic disease characterized by DPMC >0.85, Gleason 8–10 tumors, synchronous metastatic presentation, and high-volume disease. They also tended to be younger, have fewer comorbidities, and were more likely to have received prior local radiotherapy and to present with visceral metastases. These imbalances further justified the use of propensity score and weighted multivariable analyses to account for treatment selection bias in evaluating the predictive role of the Decipher classifier.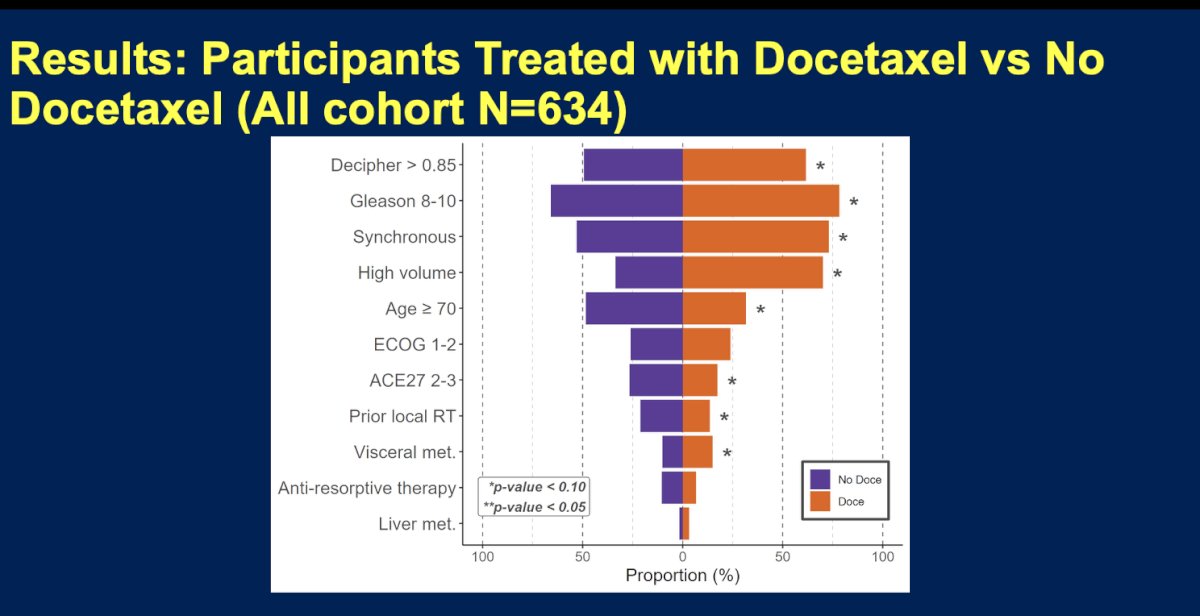
When outcomes were analyzed according to DPMC score within the ADT plus enzalutamide backbone cohort, the addition of docetaxel appeared to provide differential benefit based on transcriptomic risk. Among patients with high-risk disease (DPMC >0.85), overall survival was similar between those treated with ADT plus enzalutamide alone and those who also received docetaxel (HR 1.08, 95% CI 0.69–1.71; p=0.73), despite the fact that patients receiving docetaxel had a greater burden of poor prognostic clinical features. This suggests that docetaxel may have mitigated the adverse prognosis associated with high-risk biology. In contrast, among patients with lower-risk disease (DPMC ≤0.85), the addition of docetaxel was associated with inferior outcomes compared with ADT plus enzalutamide alone (HR 3.02, 95% CI 1.59–5.76; p<0.001). These findings support the potential predictive role of the DPMC classifier in identifying patients most likely to benefit from treatment intensification with docetaxel.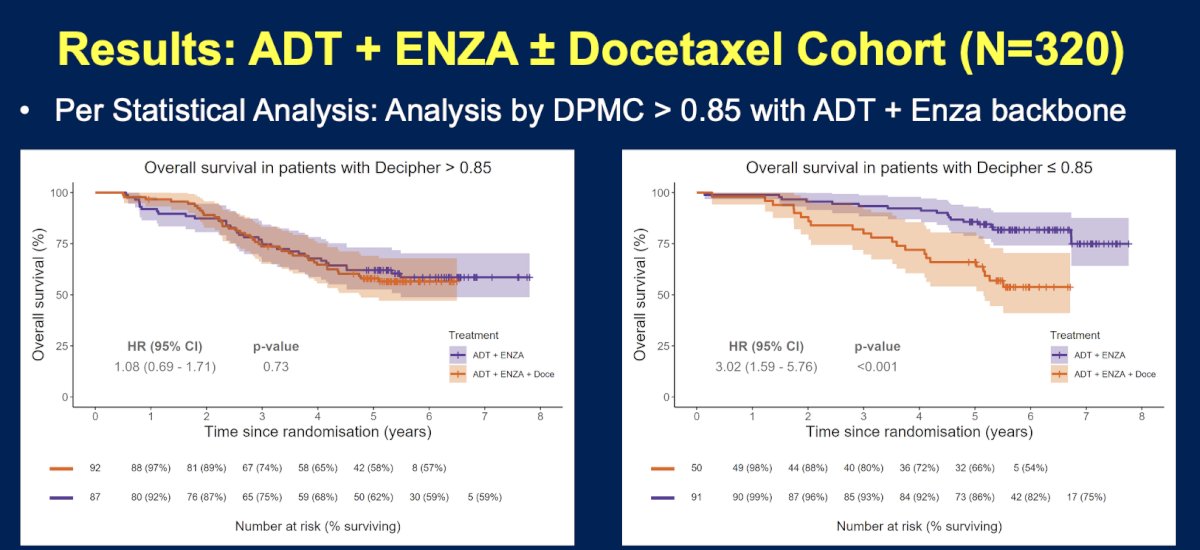
Among patients with high-volume disease, the prognostic impact of the DPMC classifier appeared particularly pronounced. In the ADT plus enzalutamide cohort, patients with DPMC >0.85 had substantially worse overall survival compared with those with DPMC ≤0.85, with 5-year OS rates of 41% versus 81%, respectively (HR 2.83, 95% CI 1.07–7.49). In contrast, among patients treated with ADT plus enzalutamide plus docetaxel, outcomes were similar regardless of DPMC status, with 5-year OS rates of 48% for DPMC >0.85 and 58% for DPMC ≤0.85 (HR 1.07, 95% CI 0.60–1.92). These findings further support the hypothesis that docetaxel may help overcome the poor prognostic impact associated with high-risk transcriptomic disease in patients with high-volume mHSPC.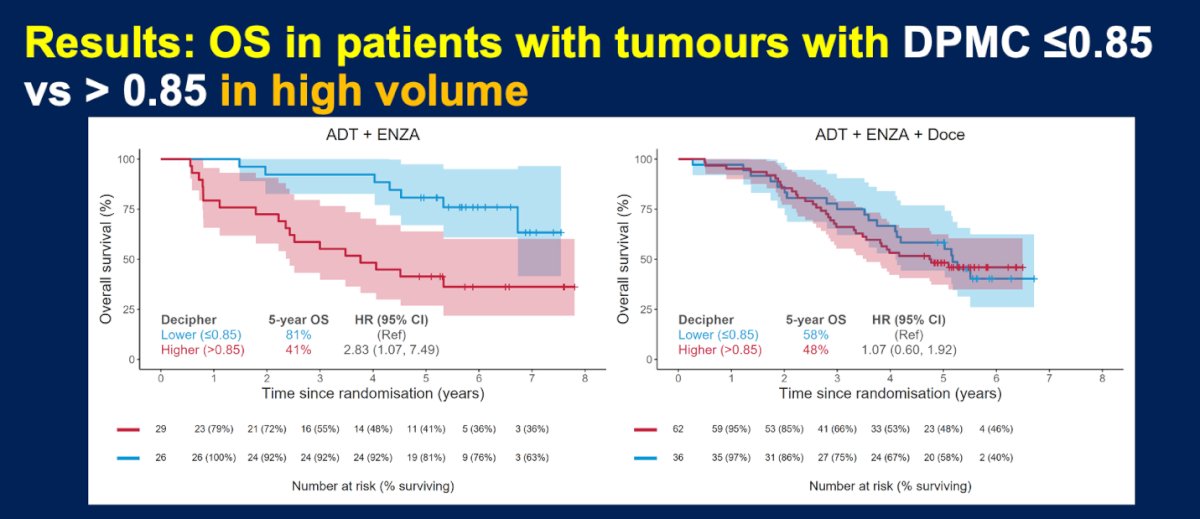
To account for treatment selection bias given the non-randomized use of docetaxel in ENZAMET, the investigators performed inverse probability of treatment weighting using propensity score modeling based on baseline clinical factors known at randomization. Weighting substantially improved the balance between treatment groups, with most covariates moving within the predefined acceptable standardized mean difference threshold of ≤0.2. However, residual imbalance remained for disease volume, Gleason score, and timing of metastases in the ADT plus enzalutamide plus docetaxel cohort, suggesting that unmeasured clinical or biological factors may still have influenced the decision to administer docetaxel.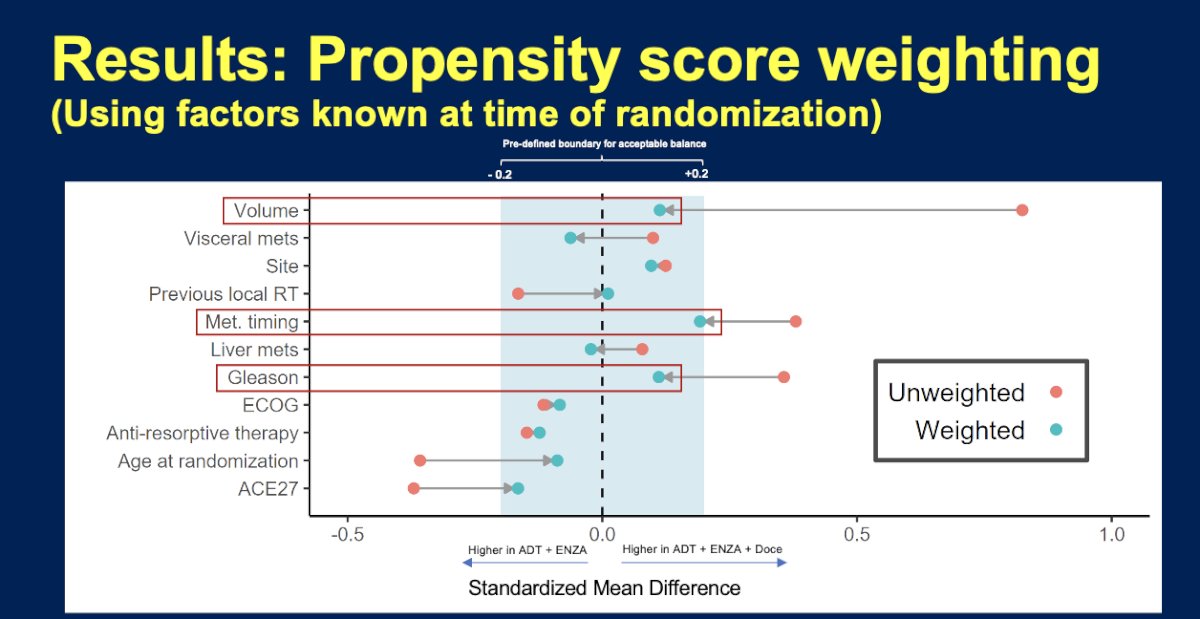
After adjustment with inverse probability of treatment weighting (IPTW) and multivariable analysis (MVA), a significant interaction between DPMC status and docetaxel benefit was observed. Among patients with lower Decipher scores (≤0.85), the addition of docetaxel to ADT plus enzalutamide was associated with worse overall survival (IPTW-weighted HR 1.94, 95% CI 0.95–3.96), whereas patients with higher Decipher scores (>0.85) demonstrated a trend toward improved overall survival with triplet therapy (IPTW-weighted HR 0.75, 95% CI 0.43–1.33). The interaction remained statistically significant after weighting (interaction p=0.04), supporting the hypothesis that higher DPMC scores may predict preferential benefit from adding docetaxel to ADT plus enzalutamide, although some residual imbalance remained despite propensity score adjustment.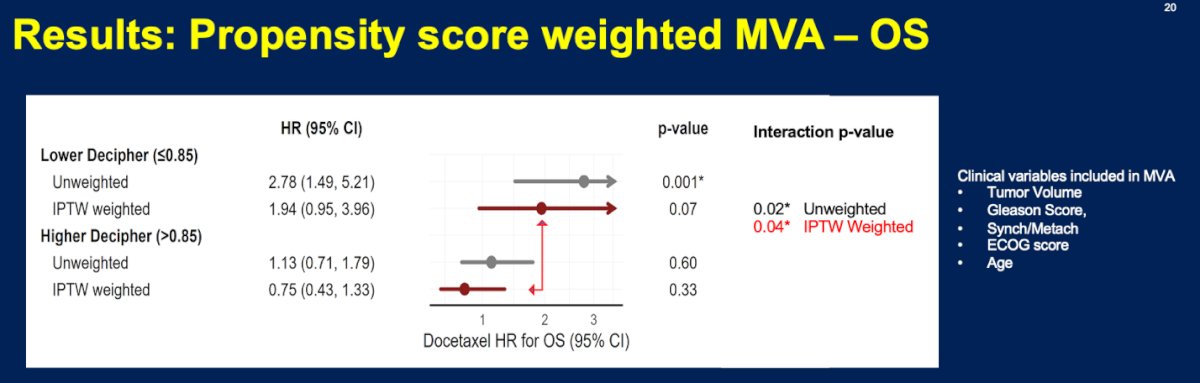
Dr. Sweeney acknowledged several important limitations of these analyses, most notably the lack of randomization to docetaxel use within ENZAMET, which introduced potential selection bias despite the use of multiple statistical adjustment strategies, including inverse probability treatment weighting and propensity score analyses. Additional limitations included variability in the use of prostate-directed radiation therapy and stereotactic body radiotherapy for metastatic disease, as treatment decisions were left to clinician's discretion. He also noted that broader global access to Decipher testing remains a challenge and emphasized that the biological mechanisms underlying the apparent benefit of docetaxel in patients with higher DPMC scores (>0.85) remain incompletely understood, warranting further investigation through genomic classifier correlations and exploratory machine learning-based analyses.
Dr. Sweeney concluded his presentation with the following key takeaway messages:
- Patients with metastatic hormone-sensitive prostate cancer demonstrate substantial biological heterogeneity despite treatment with modern ARPI-based therapy.
- ADT plus ARPI improves survival across prognostic groups compared with ADT alone.
- The Decipher Prostate Metastatic Classifier (DPMC) may help refine treatment selection for triplet therapy in mHSPC.
- Tumors with DPMC scores >0.85 were associated with worse outcomes with ADT plus enzalutamide alone.
- Patients with DPMC scores >0.85 appeared to derive benefit from the addition of docetaxel to ADT plus enzalutamide.
- Patients with DPMC scores ≤0.85 showed no clear evidence of benefit from docetaxel intensification.
- These findings suggest docetaxel may potentially be avoided in selected patients with lower DPMC scores.
Presented by: Christopher Sweeney, MBBS, Director, South Australian ImmunoGENomics Cancer Institute (SAiGENCI), Professor of Medicine, University of Adelaide, Consulting Medical Oncologist, Royal Adelaide Hospital in Adelaide, Australia
Written by: Rashid K. Sayyid, MD, MSc, Assistant Professor, Urologic Oncologist, Department of Urology at The University of Arizona and Banner University Medical Center, Tucson, AZ – @rksayyid on X during the American Society of Clinical Oncology Genitourinary (ASCO) Annual Meeting held in Chicago, IL between May 29th and June 1st, 2026
Related content: Predicting Docetaxel Benefit with a Genomic Classifier in mHSPC - Christopher Sweeney
References:
- Fizazi K, Foulon S, Carles J, Roubaud G, McDermott R, Fléchon A, Tombal B, Supiot S, Berthold D, Ronchin P, Kacso G, Gravis G, Calabro F, Berdah JF, Hasbini A, Silva M, Thiery-Vuillemin A, Latorzeff I, Mourey L, Laguerre B, Abadie-Lacourtoisie S, Martin E, El Kouri C, Escande A, Rosello A, Magne N, Schlurmann F, Priou F, Chand-Fouche ME, Freixa SV, Jamaluddin M, Rieger I, Bossi A; PEACE-1 investigators. Abiraterone plus prednisone added to androgen deprivation therapy and docetaxel in de novo metastatic castration-sensitive prostate cancer (PEACE-1): a multicentre, open-label, randomised, phase 3 study with a 2 × 2 factorial design. Lancet. 2022 Apr 30;399(10336):1695-1707. doi: 10.1016/S0140-6736(22)00367-1. Epub 2022 Apr 8. PMID: 35405085.
- Smith MR, Hussain M, Saad F, Fizazi K, Sternberg CN, Crawford ED, Kopyltsov E, Park CH, Alekseev B, Montesa-Pino Á, Ye D, Parnis F, Cruz F, Tammela TLJ, Suzuki H, Utriainen T, Fu C, Uemura M, Méndez-Vidal MJ, Maughan BL, Joensuu H, Thiele S, Li R, Kuss I, Tombal B; ARASENS Trial Investigators. Darolutamide and Survival in Metastatic, Hormone-Sensitive Prostate Cancer. N Engl J Med. 2022 Mar 24;386(12):1132-1142. doi: 10.1056/NEJMoa2119115. Epub 2022 Feb 17. PMID: 35179323; PMCID: PMC9844551.
- Freedland SJ, de Almeida Luz M, De Giorgi U, Gleave M, Gotto GT, Pieczonka CM, Haas GP, Kim CS, Ramirez-Backhaus M, Rannikko A, Tarazi J, Sridharan S, Sugg J, Tang Y, Tutrone RF Jr, Venugopal B, Villers A, Woo HH, Zohren F, Shore ND; EMBARK Study. Improved Outcomes with Enzalutamide in Biochemically Recurrent Prostate Cancer. N Engl J Med. 2023 Oct 19;389(16):1453-1465. doi: 10.1056/NEJMoa2303974. Erratum in: N Engl J Med. 2025 Aug 21;393(8):832. doi: 10.1056/NEJMx250003. PMID: 37851874.
- Kyriakopoulos CE, Chen YH, Carducci MA, Liu G, Jarrard DF, Hahn NM, Shevrin DH, Dreicer R, Hussain M, Eisenberger M, Kohli M, Plimack ER, Vogelzang NJ, Picus J, Cooney MM, Garcia JA, DiPaola RS, Sweeney CJ. Chemohormonal Therapy in Metastatic Hormone-Sensitive Prostate Cancer: Long-Term Survival Analysis of the Randomized Phase III E3805 CHAARTED Trial. J Clin Oncol. 2018 Apr 10;36(11):1080-1087. doi: 10.1200/JCO.2017.75.3657. Epub 2018 Jan 31. PMID: 29384722; PMCID: PMC5891129.
- Grist E, Dutey-Magni P, Parry MA, Mendes L, Sachdeva A, Proudfoot JA, Hamid AA, Ismail M, Howlett S, Friedrich S, DePaula Oliveira L, Murphy L, Brawley C, Dairo O, Lall S, Liu Y, Wetterskog D, Wingate A, Nowakowska K, Zakka L, Amos CL, Atako NB, Wang V, Rush HL, Jones RJ, Leung H, Cross WR, Gillessen S, Parker CC, Marafioti T, Urbanucci A, Fittall M, Schaeffer EM, Spratt DE, Waugh D, Powles T, Sydes MR, Feng FY, Berney DM, Parmar MKB, Clarke NW, Davicioni E, Lotan TL, Sweeney CJ, Brown LC, James ND, Attard G. Tumor transcriptome-wide expression classifiers predict treatment sensitivity in advanced prostate cancers. Cell. 2025 Oct 2;188(20):5717-5734.e10. doi: 10.1016/j.cell.2025.07.042. Epub 2025 Aug 26. PMID: 40865526.