(UroToday.com) The 2026 ASCO annual meeting featured a models of care session and a presentation by Dr. Zachary Moore discussing practice patterns and outcomes by genomic risk in octogenarians with high-risk localized prostate cancer. Chronologic age and traditional clinical-pathologic prostate cancer risk factors (ie. PSA, Gleason Score) are useful but incomplete predictors of prognosis. In octogenarians with high risk or very high risk localized prostate cancer, management decisions must balance: risk of progression and metastasis, treatment related morbidity, and competing non cancer mortality. While some octogenarians may benefit from watchful waiting for clinically high risk and very high risk prostate cancer due to competing risks, others may survive more than a decade with curative prostate directed treatment. At the ASCO 2026 annual meeting, Dr. Moore and colleagues examined real world data on practice patterns and outcomes for octogenarians with high risk prostate cancer stratified by genomic classifier scores.
This was a retrospective cohort study conducted using a national database of clinical−genomic linkage of Decipher genomic classifier with longitudinal real world data (Veracyte). The cohort included 1,519 patients, ≥80-years-old with high risk/very high risk prostate cancer who underwent genomic classifier testing with >1 year of follow-up. Patients were stratified by low (genomic classifier-low) compared to intermediate or high (genomic classifier-high/intermediate) genomic classifier scores. Observational management was determined by the absence of treatment with evidence of prostate cancer related services (ie. genomic classifier-high/intermediate-observation). Freedom from distant metastases, metastasis free survival, and overall survival were modeled using Kaplan Meier analysis and log-rank tests.
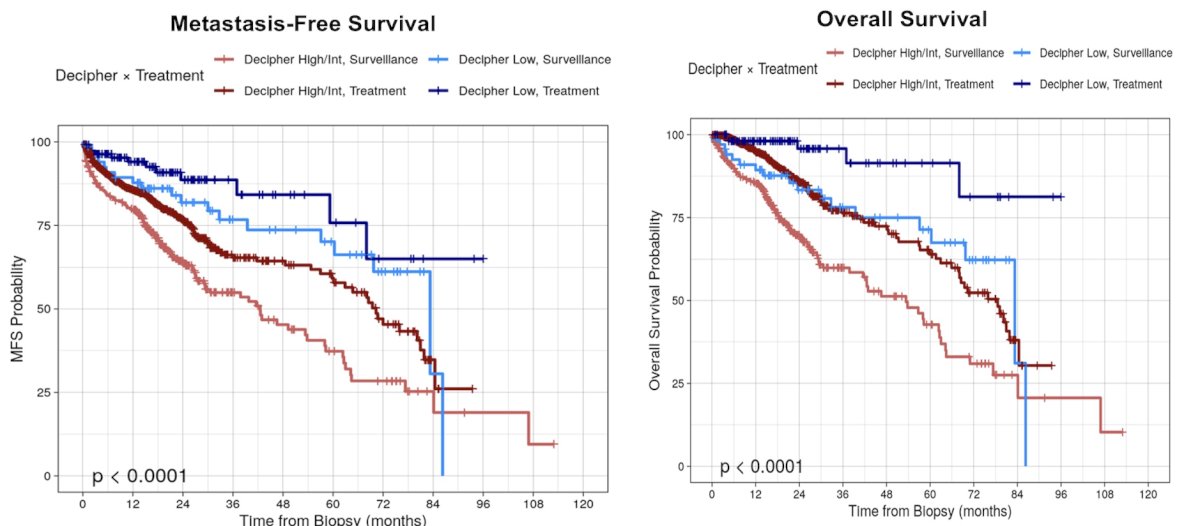
Most patients (86%) had genomic classifier-high/intermediate risk disease. The rate of observational management was significantly lower in the genomic classifier-high/intermediate cohort compared to the genomic classifier-low cohorts (26% versus 38%, p = 0.001). Among treated patients, there were similar rates of ADT only use (52% genomic classifier-low versus 54% genomic classifier-high/intermediate), but amongst those who were treated with radiotherapy, concurrent ADT use was lower in genomic classifier-low compared to genomic classifier-high/intermediate (55% versus 69%, OR 0.83, 95% CI 0.73-0.95, p = 0.007). There were significant differences between groups for freedom from distant metastases (p = 0.003), metastasis free survival (p < 0.001), and overall survival (p < 0.001):
Among observed patients, genomic classifier-low had significantly better freedom from distant metastases than genomic classifier-high/intermediate (HR 0.11, 95% CI 0.02−0.80; p = 0.03).

Dr. Moore concluded his presentation discussing practice patterns and outcomes by genomic risk in octogenarians with high-risk localized prostate cancer with the following take home points:
- In patients >80 years old with NCCN high risk and very high risk localized prostate cancer, the Decipher genomic classifier score was associated with management patterns and outcomes
- Even with NCCN high risk or very high risk, patients with genomic classifier-low disease were managed with observation 38% of the time, but had favorable outcomes including better metastasis free survival and overall survival, than patients with genomic classifier-high/intermediate who were observed or treated
- In this cohort, genomic classifier-low was associated with significantly better freedom from distant metastases, with <5% risk of metastatic disease within 5 years with observation alone
- These findings suggest a genomic classifier may provide useful prognostic information in addition to standard clinicopathologic factors for elderly patients with aggressive localized prostate cancer
- Future direction includes validation in additional contexts to increase generalizability, developing patient-specific calculators integrating genomic risk, cancer specific outcomes, competing non-cancer mortality, and treatment morbidity
- Combining genomic classifier risk with geriatric assessment to guide individualized treatment intensity in older adults with localized high risk prostate cancer should be explored
Presented by: Zachary Moore, MD, PhD, Memorial Sloan Kettering Cancer Center, New York, NY
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Associate Professor of Urology, Georgia Cancer Center, Wellstar MCG Health, @zklaassen_md on Twitter during the American Society of Clinical Oncology Genitourinary (ASCO) Annual Meeting held in Chicago, IL between May 29th and June 1st, 2026