(UroToday.com) The 2026 American Society of Clinical Oncology Genitourinary (ASCO) Annual Meeting held in Chicago, IL between Fri, May 29 – Tues, Jun 2, 2026, was host to Prostate, Testicular, and Penile Cancer – Posters Session. Dr. Andrew J. Armstrong presented Abstract 5093: Predictors of treatment duration in patients with mHSPC treated with ENZA: A post hoc analysis of ARCHES.
Dr. Armstrong highlighted that prior analyses from the phase 3 ARCHES trial demonstrated significant improvements in radiographic progression-free survival and overall survival with enzalutamide plus ADT compared with placebo plus ADT in patients with metastatic hormone-sensitive prostate cancer (mHSPC). (1) This post hoc analysis explored factors associated with varying durations of enzalutamide treatment exposure and evaluated reasons for treatment discontinuation over long-term follow-up.
Patients receiving enzalutamide were categorized according to treatment duration into short treatment (STx, 0–2 years), medium treatment (MTx, 2–5 years), and long treatment duration (LTx, >5 years). Among 572 enzalutamide-treated patients, 204 (36%) were classified as STx, 140 (24%) as MTx, and 228 (40%) as LTx.
The study endpoints included exposure-adjusted event rates (EAERs) of treatment-emergent adverse events according to treatment duration, as well as exposure-adjusted rates of treatment-related adverse events of special interest over time. Additional endpoints included overall survival according to treatment duration and identification of baseline clinical factors predictive of longer treatment duration. The data cutoff for these analyses was July 31, 2024.
Among the 572 patients randomized to ENZA + ADT, 204 patients (36%) received short treatment duration (STx), 140 (24%) medium treatment duration (MTx), and 228 (40%) long treatment duration (LTx). Progressive disease and adverse events or participant withdrawal represented the most common reasons for treatment discontinuation across treatment duration subgroups. Notably, within the STx subgroup, 14 patients (6.9%) discontinued treatment for reasons other than progressive disease, adverse events, participant withdrawal, or death.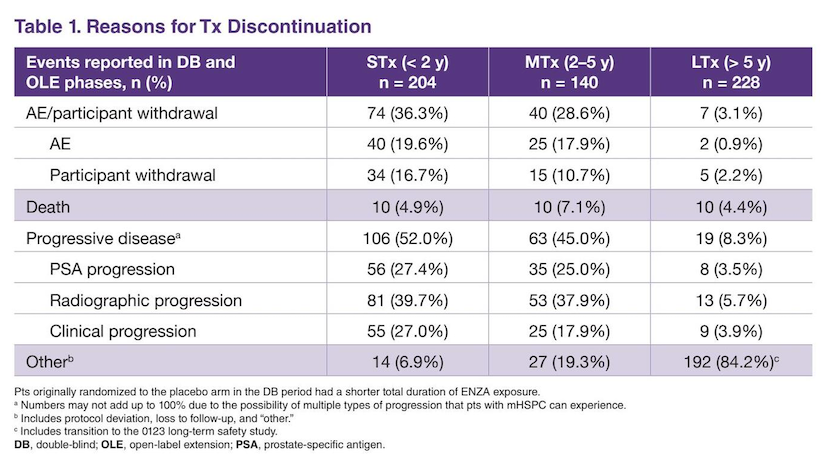
Dr. Armstrong noted that patients in the STx cohort were generally older and more likely to present with high-volume disease and ECOG performance status 1 compared with patients in the MTx and LTx groups. However, importantly, adverse disease features remained common even among patients with prolonged treatment exposure, as 55.3% of patients in the LTx cohort had high-volume disease and 73.2% had synchronous metastatic disease.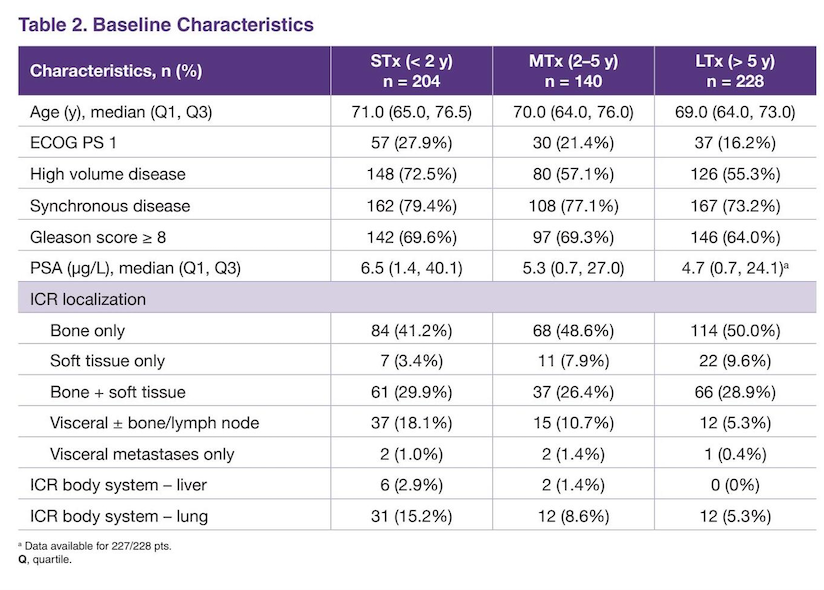
Drug-related treatment-emergent adverse events per 100 patient-years were more common among patients receiving short treatment duration (STx; 156.0) compared with medium (MTx; 89.5) and long treatment duration (LTx; 47.1). Similarly, treatment-emergent adverse events leading to treatment discontinuation occurred more frequently in the STx subgroup (34.2 per 100 patient-years) versus MTx (8.5) and LTx (0.6). Rates of treatment-related adverse events leading specifically to treatment discontinuation were 12.4, 1.5, and 0.1 per 100 patient-years for STx, MTx, and LTx, respectively. Dr. Armstrong noted that adverse events leading to treatment discontinuation were heterogeneous, with no single predominant toxicity pattern identified. Treatment-emergent adverse events leading to dose reduction were observed at rates of 6.2, 5.8, and 2.0 per 100 patient-years in the STx, MTx, and LTx groups, respectively.
Achievement of deep PSA responses differed substantially according to treatment duration. A PSA nadir <0.2 ng/mL post-baseline was observed in 44.4% of STx patients, compared with 78.9% in the MTx group and 91.4% among patients receiving long-term therapy. Similarly, ECOG PS 0 status was more common among patients with prolonged treatment duration.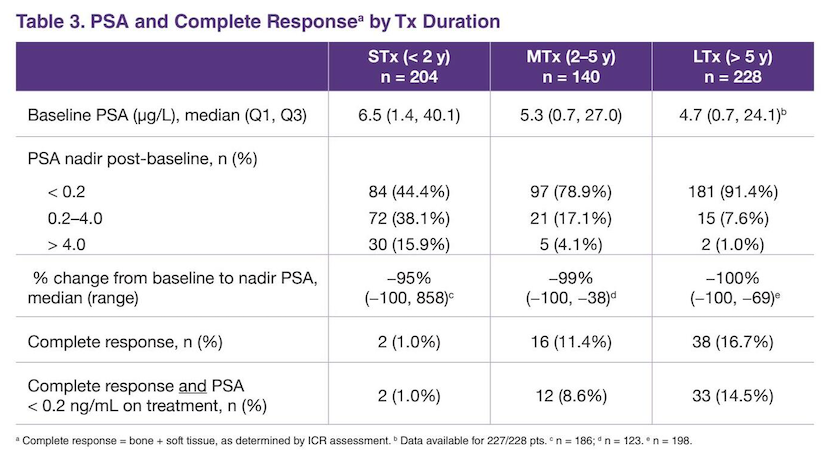
Rates of adverse events of special interest were also generally higher among patients with shorter treatment duration. Fatigue rates per 100 patient-years were 19 in STx patients compared with 10.7 and 4.8 in the MTx and LTx groups, respectively. Select cardiovascular events, falls, fractures, and convulsions were also numerically more frequent among STx patients.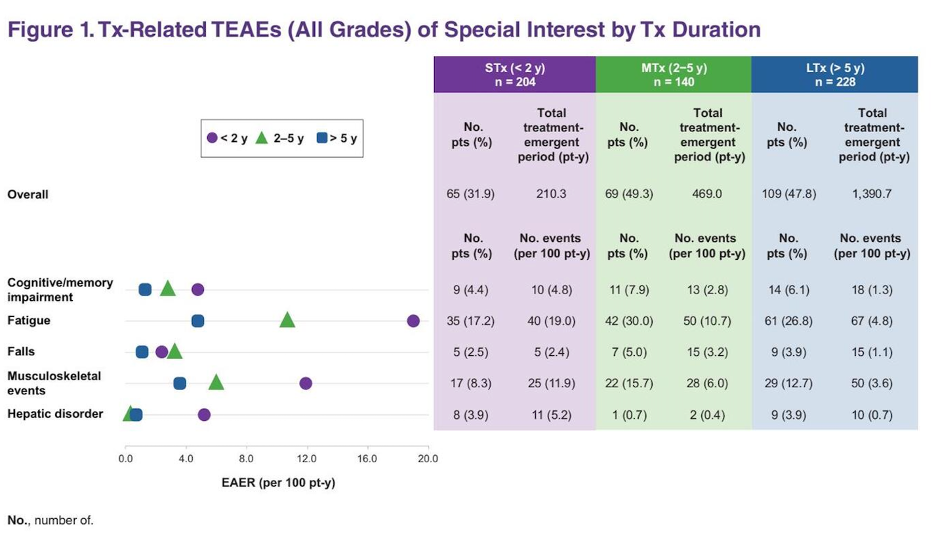
Overall survival outcomes varied substantially according to treatment duration, with the most pronounced benefit observed among patients receiving long treatment duration (LTx). Median overall survival was 29.5 months in the short-treatment subgroup, 57.3 months in the medium-treatment subgroup, and was not estimable in the long-treatment subgroup, where only 12 events (5.3%) had occurred at the time of analysis. Compared with the short-treatment subgroup, the risk of death was significantly lower among patients receiving medium-duration therapy (HR 0.30; 95% CI 0.22–0.42) and especially among those receiving long-duration therapy (HR 0.01; 95% CI 0.00–0.03), highlighting that the overall survival benefit was greatest in patients able to remain on prolonged ENZA + ADT treatment.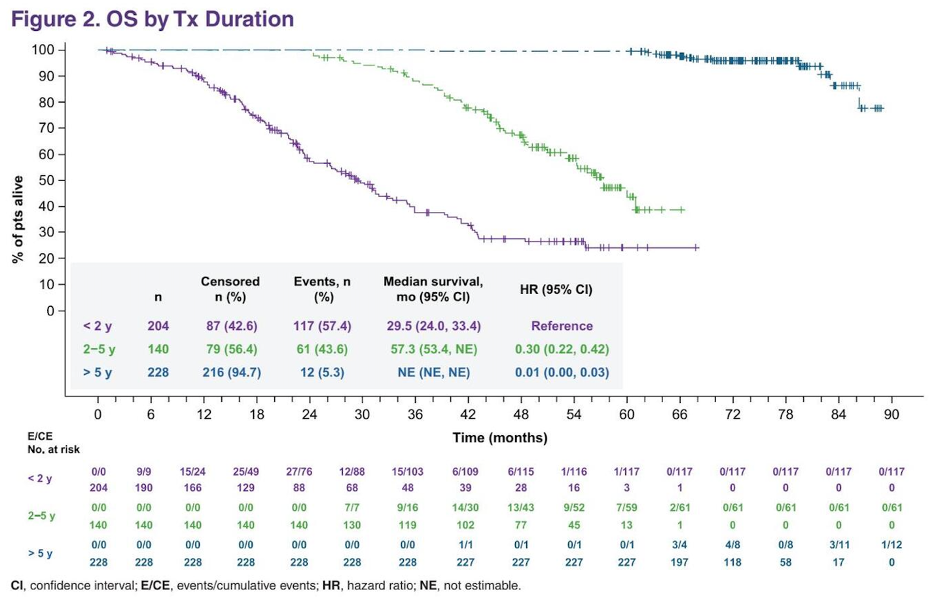
Among multiple potential confounders identified in univariate analyses, high disease volume emerged as the only independent predictor of early treatment discontinuation in multivariable analyses. Patients with low-volume disease were significantly more likely to remain on longer ENZA + ADT treatment compared with those with high-volume disease, both in comparisons of short- versus medium-duration therapy (OR 2.24; 95% CI 1.39–3.64; p=0.001) and short- versus long-duration therapy (OR 2.45; 95% CI 1.59–3.77; p<0.0001).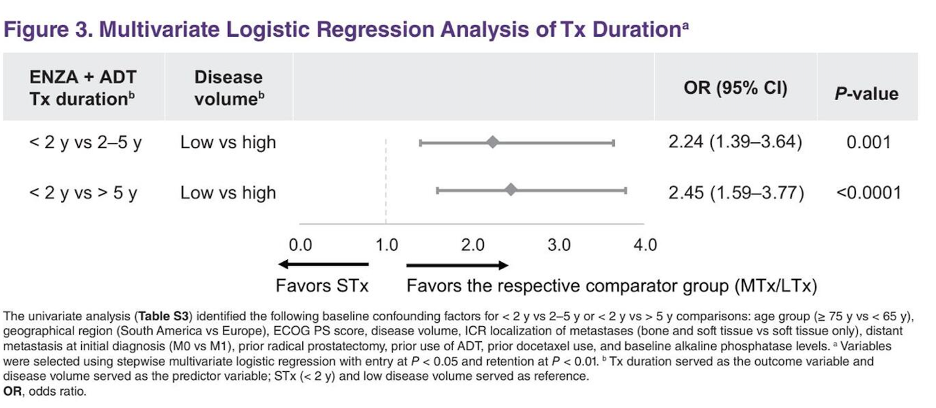
Dr. Armstrong acknowledged several important limitations of the analysis. He noted that the treatment-duration subgroups were predefined primarily to ensure adequate sample sizes, which may have influenced both safety and efficacy outcomes across groups. In addition, the overall survival analyses were descriptive and exploratory in nature and may have been affected by selection bias and immortal time bias. Moreover, limited data were collected during the ARCHES open-label extension phase initiated after study unblinding, and genetic or genomic tumor data were not available for analysis. The study also did not distinguish predictors of early toxicity from predictors of early disease progression, and prospective risk-mitigation strategies such as dose reductions or treatment holds for ENZA-related adverse events were not predefined.
Dr. Armstrong concluded his presentation with the following key messages:
- Short ENZA + ADT treatment duration was most commonly driven by early disease progression (52.0%), followed by adverse events (19.6%) and participant withdrawal (16.7%)
- Patients receiving medium- and long-duration treatment generally had more favorable baseline disease characteristics compared with those receiving short-duration therapy
- Despite this, a substantial proportion of patients in the long-treatment subgroup still had high-volume (55.3%) and synchronous disease (73.2%)
- High disease volume was the only independent predictor of early treatment discontinuation in multivariable analyses
- Complete radiographic and biochemical response (PSA <0.2 ng/mL) was achieved more frequently in the long-treatment subgroup (14.5%) compared with the medium- (8.6%) and short-treatment (1.0%) subgroups
- Notably, 44.4% of patients in the short-treatment subgroup still achieved PSA <0.2 ng/mL despite shorter therapy exposure
- Treatment-related adverse events of special interest occurred more frequently in the short-treatment subgroup compared with the medium- and long-treatment groups
- No single dominant toxicity pattern leading to treatment discontinuation was identified
- Adverse event-related treatment changes are multifactorial, and dose modifications along with proactive management of adverse events and comorbidities may help prolong ENZA treatment duration
Presented by: Andrew Armstrong, MD, MSc, Medical Oncologist, Professor of Medicine, Surgery, Pharmacology and Cancer Biology, Duke Cancer Institute, Center for Prostate and Urologic Cancers, Durham, NC
Written by: Julian Chavarriaga, MD, Clinical Assistant Professor, Urologic Oncologist, Department of Urology at Penn State Health @chavarriagaj on X during the American Society of Clinical Oncology Genitourinary (ASCO) Annual Meeting held in Chicago, IL between May 29th and June 1st, 2026
Reference: