(UroToday.com) The 2026 American Society of Clinical Oncology Genitourinary (ASCO) Annual Meeting held in Chicago, IL between Fri, May 29 – Tues, Jun 2, 2026, was host to Prostate, Testicular, and Penile Cancer – Posters Session. Dr. Karen A. Autio presented Abstract TPS5142: TIDAL: A phase II study of the DLL3-directed T-cell engager tarlatamab in DLL3-positive metastatic prostate cancer.
Dr. Autio highlighted that while T-cell engagers targeting canonical prostate adenocarcinoma surface antigens such as STEAP1 and KLK2 have shown meaningful activity, additional tumor-directed targets are needed for patients whose tumors develop lineage plasticity or neuroendocrine/small cell features.1,2 DLL3 is a surface antigen variably expressed across neuroendocrine and small cell malignancies and has emerged as a potential therapeutic target in this setting.3
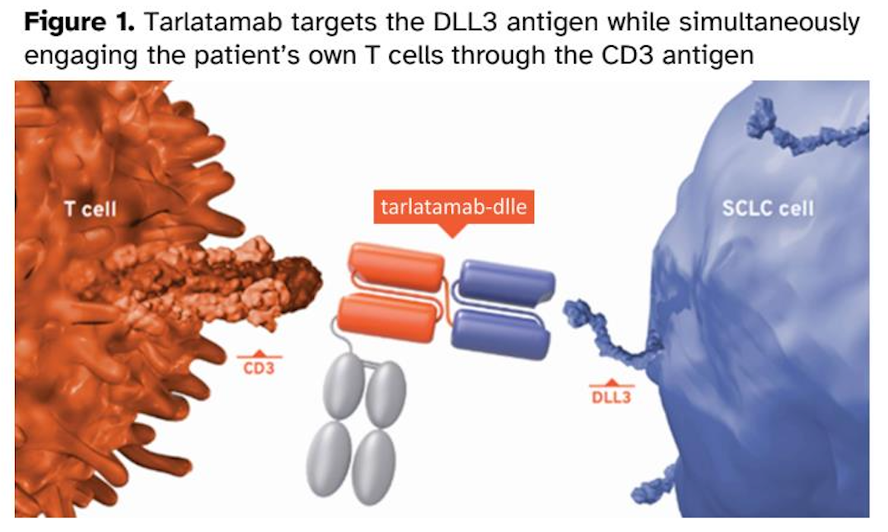
Tarlatamab is a bispecific T-cell engager targeting DLL3 and CD3, with regulatory approval in small cell lung cancer and emerging evidence of activity in DLL3-positive prostate cancer. The TIDAL trial (NCT07111507) is a multicenter, prospective, single-arm phase II study evaluating the safety and efficacy of tarlatamab in patients with DLL3-positive advanced prostate cancer.
Eligible patients must have metastatic prostate cancer with progression after at least one prior systemic therapy in the metastatic setting and DLL3-positive disease, defined as IHC ≥50%, regardless of histologic subtype. Patients without measurable disease by RECIST 1.1 may enroll, although at least 50% of the overall study population must have measurable disease.
Tarlatamab is administered in 28-day cycles using a step-up dosing strategy, beginning with a 1 mg priming dose on cycle 1 day 1, followed by the target dose of 10 mg on cycle 1 day 8, cycle 1 day 15, and days 1 and 15 of subsequent cycles. Given the potential for early immune-mediated toxicity with T-cell engagers, all patients require hospitalization for at least 24 hours of monitoring after the cycle 1 day 1 and cycle 1 day 8 infusions.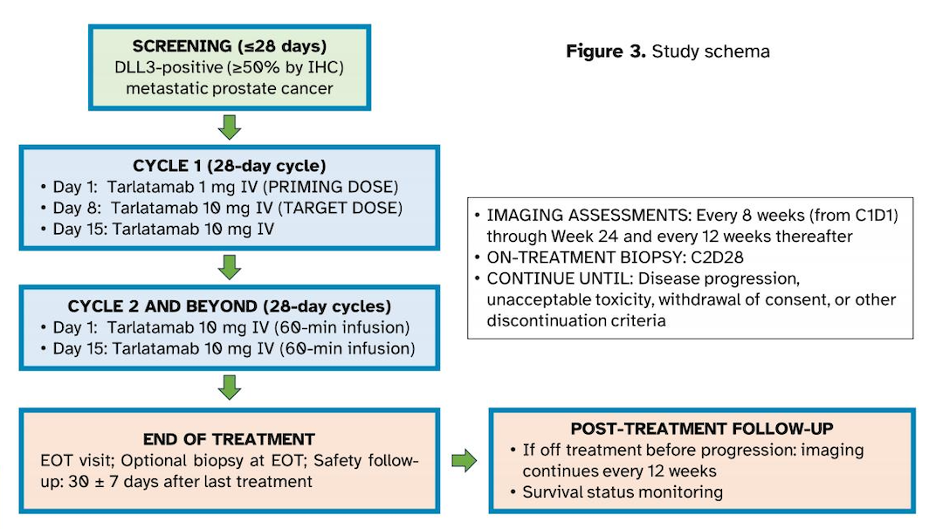
The study also incorporates mandatory translational assessments. Tumor biopsy and ctDNA collection are required at screening and again at cycle 2. At end of treatment, ctDNA collection is required, while repeat biopsy is optional. Disease assessments with CT and bone scan are performed every 8 weeks for the first 24 weeks and every 12 weeks thereafter.
The primary endpoint is 24-week radiographic progression-free survival. Secondary endpoints include objective response rate, median duration of response, median rPFS, median composite PFS, median OS, and safety.
Importantly, the trial includes correlative analyses evaluating the association between tumor DLL3 expression, circulating immune profiles, and clinical outcomes. A subset of patients may also co-enroll in an imaging biomarker study using a novel DLL3 PET tracer, 89Zr-DFO-SC16.56, to further characterize DLL3 expression and potentially support patient selection.
As of April 29, 2026, 7 of the planned 32 participants have been enrolled, with the first patient enrolled on September 8, 2025. The planned investigational sites are illustrated below:

Presented by: Karen Autio, MD, MSc, Memorial Sloan Kettering Cancer Center, New York, NY, United States of America
Written by: Julian Chavarriaga, MD, Clinical Assistant Professor, Urologic Oncologist, Department of Urology at Penn State Health @chavarriagaj on X during the American Society of Clinical Oncology Genitourinary (ASCO) Annual Meeting held in Chicago, IL between May 29th and June 1st, 2026
References:
- Kelly WK, Danila DC, Lin CC, Lee JL, Matsubara N, Ward PJ, Armstrong AJ, Pook D, Kim M, Dorff TB, Fischer S, Lin YC, Horvath LG, Sumey C, Yang Z, Jurida G, Smith KM, Connarn JN, Penny HL, Stieglmaier J, Appleman LJ. Xaluritamig, a STEAP1 √ó CD3 XmAb 2+1 Immune Therapy for Metastatic Castration-Resistant Prostate Cancer: Results from Dose Exploration in a First-in-Human Study. Cancer Discov. 2024 Jan 12;14(1):76-89. doi: 10.1158/2159-8290.CD-23-0964. PMID: 37861461; PMCID: PMC10784743.
- Stein MN, Vinceneux A, Robbrecht D, Doger B, Autio KA, Schweizer MT, Calvo E, Medina L, Van Dongen M, Deville JL, Bernard-Tessier A, Ghosh D, Shotts K, Shen F, Jaiprasart P, Chaudhary R, Wu S, Cartee L, Schnepp R, Gaut D, Lauring J, Wang SC, Villalobos VM, Baldini C. Pasritamig, a First-in-Class, Bispecific T-Cell Engager Targeting Human Kallikrein 2, in Metastatic Castration-Resistant Prostate Cancer: A Phase I Study. J Clin Oncol. 2025 Aug;43(22):2515-2526. doi: 10.1200/JCO-25-00678. Epub 2025 Jun 1. PMID: 40450573; PMCID: PMC12288886.
- Chou J, Egusa EA, Wang S, Badura ML, Lee F, Bidkar AP, Zhu J, Shenoy T, Trepka K, Robinson TM, Steri V, Huang J, Wang Y, Small EJ, Chan E, Stohr BA, Ashworth A, Delafontaine B, Rottey S, Cooke KS, Hashemi Sadraei N, Yu B, Salvati M, Bailis JM, Feng FY, Flavell RR, Aggarwal R. Immunotherapeutic Targeting and PET Imaging of DLL3 in Small-Cell Neuroendocrine Prostate Cancer. Cancer Res. 2023 Jan 18;83(2):301-315. doi: 10.1158/0008-5472.CAN-22-1433. PMID: 36351060; PMCID: PMC10263373.