(UroToday.com) The 2026 American Society of Clinical Oncology Genitourinary (ASCO) Annual Meeting held in Chicago, IL between Fri, May 29 – Tues, Jun 2, 2026, was host to Prostate, Testicular, and Penile Cancer – Posters Session. Dr. Manojkumar Bupathi presented Abstract 5080: Real-world characteristics, HRR mutation testing, treatment patterns, and outcomes of patients with mCSPC in the US community oncology setting.
Dr. Bupathi highlighted that homologous recombination repair mutation (HRRm) testing is now recommended by NCCN guidelines for patients with metastatic castration-sensitive prostate cancer. Prior real-world evidence from a European cohort of 556 patients with metastatic castration-sensitive prostate cancer demonstrating poorer outcomes among patients harboring homologous recombination repair mutations, particularly BRCA alterations. (1) Patients with HRR-mutated disease experienced shorter median overall survival and radiographic progression-free survival compared with non-HRR-mutated patients (OS: 39.0 vs 55.7 months; rPFS: 20.5 vs 30.6 months). Outcomes were even worse among patients with BRCA-mutated disease compared with non-BRCA HRR mutations, with median overall survival of 25.0 versus 50.3 months and median rPFS of 13.2 versus 25.2 months, respectively. (1)
However, he noted that real-world evidence evaluating the prognostic impact of HRR mutation status in metastatic hormone-sensitive prostate cancer remains limited and heterogeneous. The current study was therefore designed to address this evidence gap and better characterize unmet clinical needs across U.S. community oncology practice settings.
This retrospective observational cohort study evaluated patients with documented HRRm testing who initiated systemic therapy for mCSPC between January 2019 and March 2024 across The US Oncology Network and affiliated non-network practices. Stratified random samples of 150 patients with HRRm and 150 without HRRm were selected for detailed chart abstraction.
Dr. Bupathi noted that study data were derived from structured fields within the iKnowMed electronic health record platform used by the US Oncology Network. The network includes more than 2,400 providers across over 700 sites of care throughout the United States, in addition to approximately 50 non-network clinics utilizing the same electronic health record platform and participating in real-world research collaborations with Ontada.
Patient characteristics within 60 days prior to index and prostate cancer treatments throughout follow-up were analyzed descriptively. Somatic and/or germline testing results were collected for 12 homologous recombination repair-related genes, including ATM, ATR, BRCA1, BRCA2, CDK12, CHEK2, FANCA, MLH1, MRE11A, NBN, PALB2, and RAD51C. High-volume disease was defined by the presence of ≥4 bone metastases, at least one bone metastasis outside the pelvis or vertebral column, visceral metastases, and/or explicit chart documentation of high-volume disease. The study design is shown below: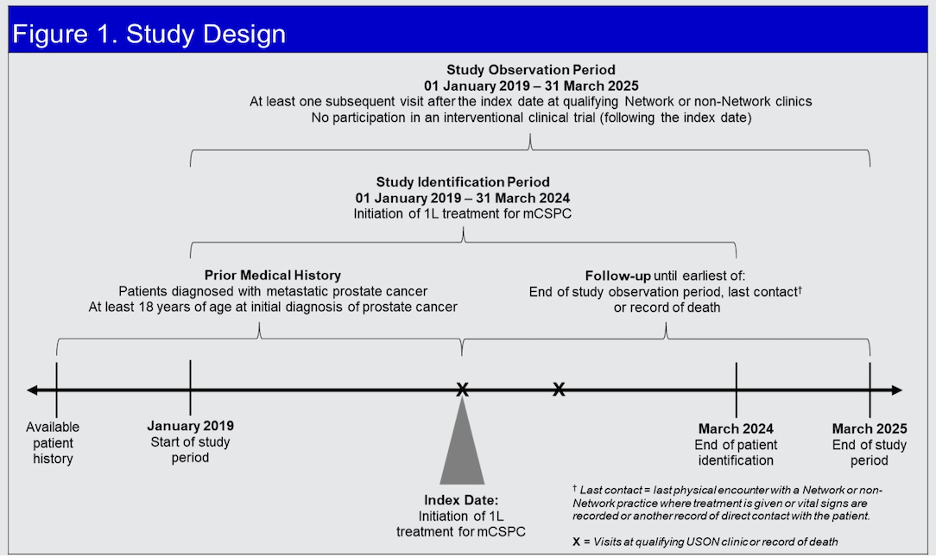
Descriptive Kaplan-Meier analyses evaluated real-world progression-free survival, defined as provider-documented disease progression, and overall survival across clinically relevant subgroups, including HRR-mutated versus non-HRR-mutated disease, BRCA-mutated versus non-BRCA HRR-mutated disease, de novo versus recurrent metastatic disease, and high-volume versus low-volume disease stratified by HRR mutation status.
Overall, 300 patients were included, with a median age of 69 years and median follow-up of 25 months. Among HRRm-positive patients, 47% harbored BRCA mutations while 53% had non-BRCA HRRm alterations. De novo metastatic disease was identified in 65% of HRRm patients and 67% of non-HRRm patients, while high-volume disease was present in 57% and 64%, respectively.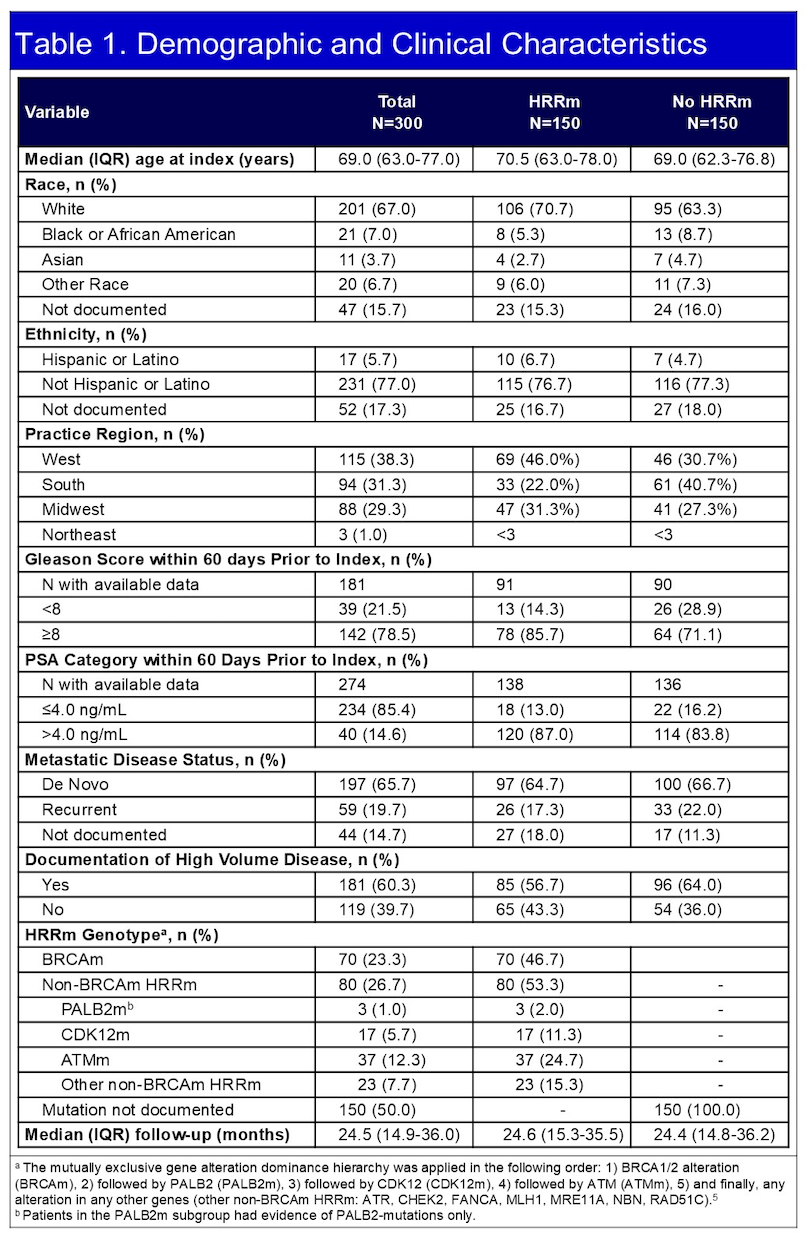
Frontline treatment approaches were generally balanced between groups, including ADT alone (28%/22%), ADT +ARPI (39%|4/%).ADT +DOC (15%/15%) and ADT+ARPI+DOC (15%/15%).
Dr. Bupathi highlighted that patients with HRRm mCSPC experienced numerically shorter survival outcomes across several clinical subgroups compared with patients without HRRm alterations. In the overall population, median OS was 44.0 months in the HRRm cohort versus 48.5 months in the non-HRRm cohort, while median rwPFS was 17.5 versus 22.6 months, respectively as shown in the Kaplan meier curves below for OS and rwPFS.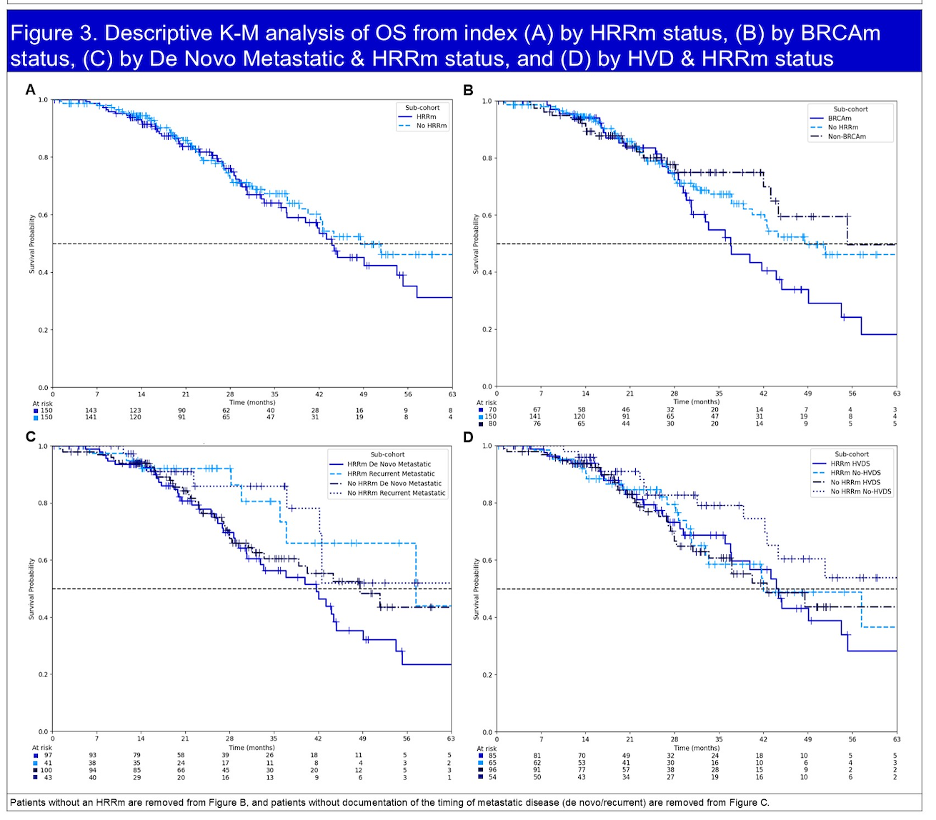
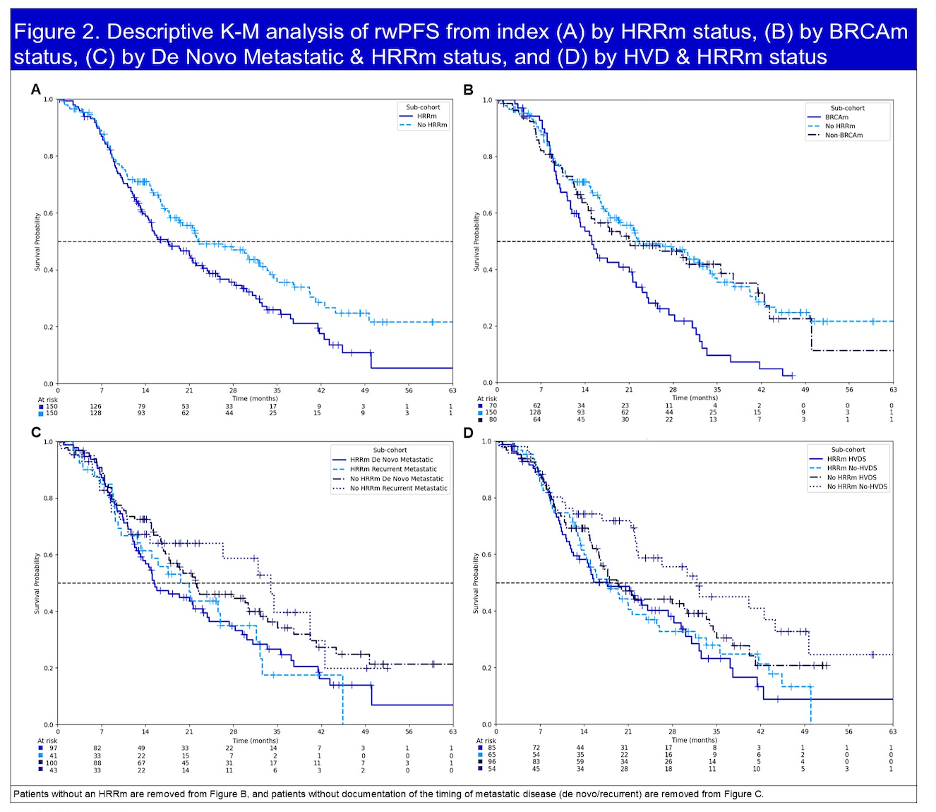
Median real-world progression-free survival and overall survival outcomes across de novo versus recurrent metastatic disease and high-volume disease subgroups were analyzed according to HRR mutation status. Among patients with de novo metastatic disease, those harboring HRR mutations experienced shorter median rwPFS (15.4 vs 22.0 months) and OS (41.7 vs 48.5 months) compared with patients without HRR mutations. Similar trends were observed in the recurrent metastatic setting, where HRR-mutated patients had shorter rwPFS (19.6 vs 33.9 months) and OS (57.4 months vs not reached).
Within the high-volume disease subgroup, patients with HRR-mutated tumors demonstrated numerically shorter rwPFS compared with non-HRR-mutated patients (17.7 vs 19.2 months), while overall survival was similar between groups (44.4 vs 42.5 months). In patients without high-volume disease, HRR-mutated status was associated with substantially shorter rwPFS (17.5 vs 31.9 months) and numerically shorter overall survival (42.0 months vs not reached).
Dr. Bupathi concluded their presentation with the following key messages:
- Real-world progression-free survival and overall survival were consistently shorter among patients with HRR-mutated mCSPC across most de novo metastatic and high-volume disease subgroups
- Poorer outcomes associated with HRR mutations appeared to be more pronounced in patients harboring BRCA mutations compared with non-BRCA HRR alterations
- These findings highlight the importance of comprehensive HRR testing and support the need for earlier implementation of biomarker-driven targeted treatment strategies in prostate cancer
Presented by: Manojkumar Bupathi, MD, MS, Medical Oncologist, Rocky Mountain Cancer Centers, Littleton, CO
Written by: Julian Chavarriaga, MD, Clinical Assistant Professor, Urologic Oncologist, Department of Urology at Penn State Health @chavarriagaj on X during the American Society of Clinical Oncology Genitourinary (ASCO) Annual Meeting held in Chicago, IL between May 29th and June 1st, 2026