(UroToday.com) The 2026 ASCO annual meeting featured an oral abstract kidney cancer session and a discussant presentation by Dr. Martin Voss discussing three abstracts “A phase 2 randomized trial of radium-223 dichloride and cabozantinib in patients with renal cell carcinoma (RCC) with bone metastases: RADICAL (Alliance A031801)” by Dr. Rana McKay, “A prospective, multi-center, phase 1b/II trial of first line cadonilimab + axitinib in advanced non-clear cell RCC” by Dr. Xu Hu, and “ctDNA analysis in participants with RCC treated with adjuvant pembrolizumab in the KEYNOTE-564 trial” by Dr. Toni Choueiri.
With regards to the RADICAL trial, patients with osseous metastases, particularly those with a high burden of disease in the bone, suffer a detriment in quality of life due to symptomatic skeletal events. Radium-223 is well established in prostate cancer, based on the ALSYMPCA trial,1 ERA-223 trial,2 and PEACE-III3 trials: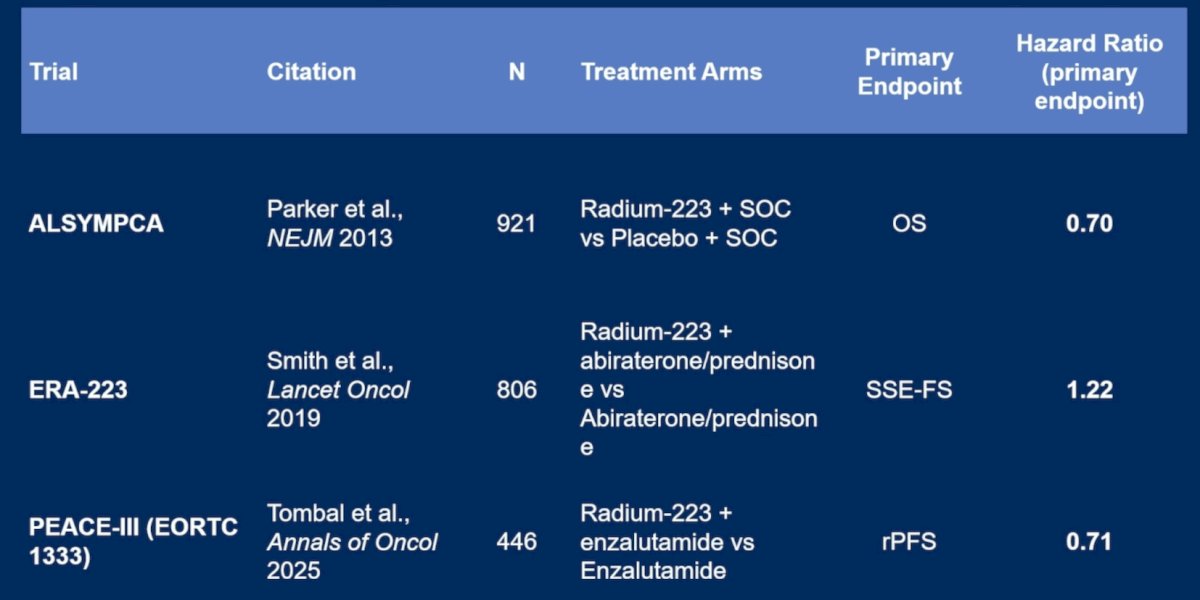
Previously, a pilot study of radium-223 with VEGF tyrosine kinase inhibitors (TKI) in RCC with bone metastases showed safety and early efficacy,4 and cabozantinib has been shown to have a proven benefit in osseous metastases based on data from the METEOR trial.5
RADICAL is an open-label multicenter study that enrolled RCC patients with ≥1 symptomatic bone metastasis not previously irradiated and Karnofsky performance status ≥60%. Prior therapies were allowed, and the non-clear cell population was limited to 20%. Randomization was 1:1 to cabozantinib with (Arm A) or without (Arm B) radium-223, stratified by osteoclast targeted therapy, prior therapy, baseline opioid use, and IMDC risk. In Arm A, cabozantinib was given as 40 mg daily for cycle 1 and 60 mg thereafter, if tolerated. Radium-223 was 1.49 microcurie/kg IV every 28 days for 6 doses. In Arm B, cabozantinib was 60 mg daily. The primary endpoint was symptomatic skeletal event-free survival, and secondary endpoints were safety, objective response rate, progression-free survival, and overall survival:
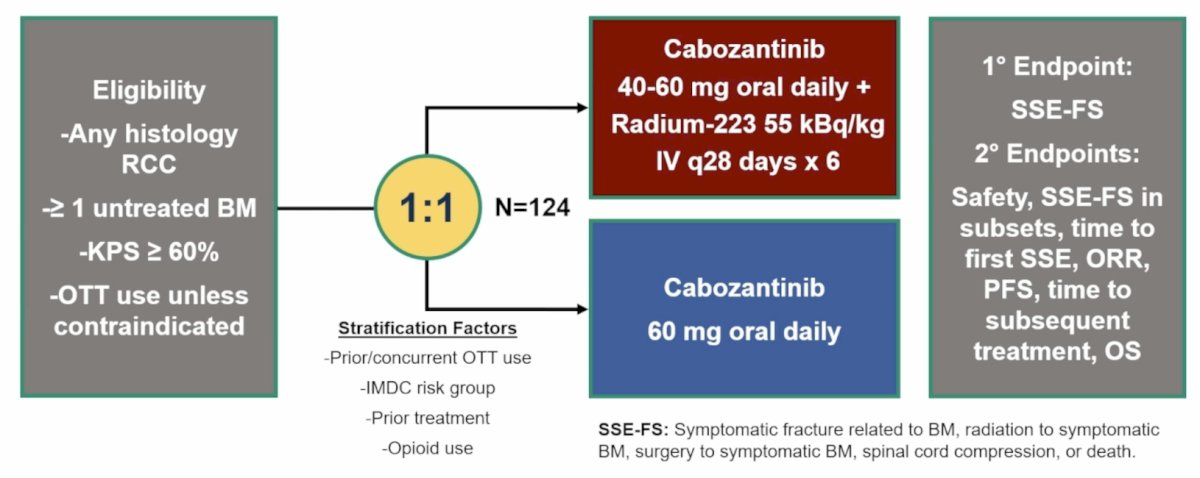
Dr. Voss noted that there are several important points to highlight regarding the trial design:
- The primary endpoint was unique, assessing symptomatic skeletal events
- There was liberal eligibility, including any prior treatment, any number of metastases, and prior symptomatic skeletal event being allowed
- Stratification factors were: prior/concurrent osteoclast targeted therapy, IMDC risk group, prior treatment, and opioid use
- For patients receiving radium-223, there was a 28-day lead-in of cabozantinib 40 mg daily, with the ability to increase to 60 mg daily versus cabozantinib 60 mg daily in the cabozantinib arm alone
Among all enrolled patients, for symptomatic skeletal event-free survival, the stratified hazard ratio was 1.46 (90% CI 0.86-2.51):
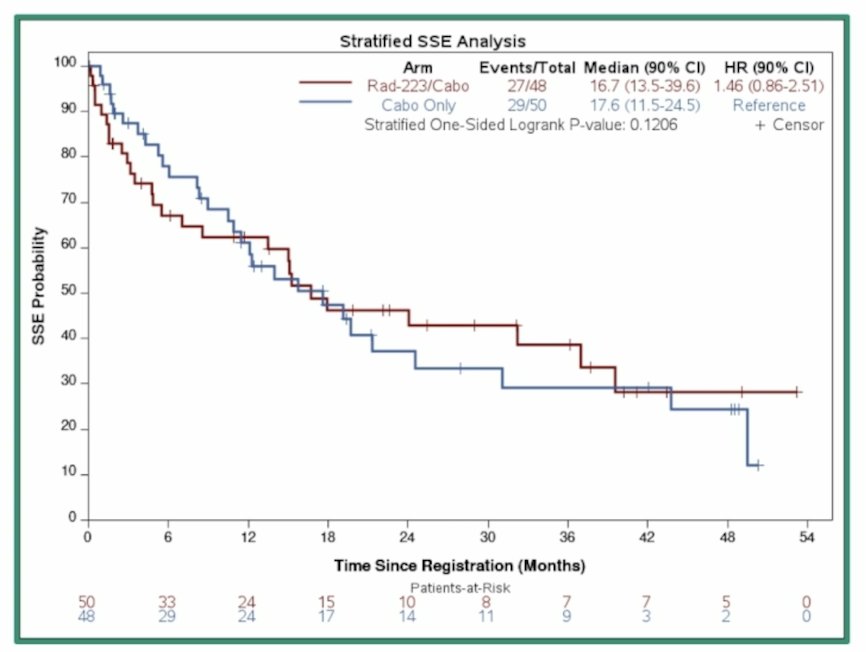
Why was there no symptomatic skeletal event benefit despite receiving additional bone-directed therapy? Dr. Voss notes that in the radium-223 arm, only 39.1% of patients had escalated cabozantinib from 40 mg to 60 mg, with a relative difference in median daily cabozantinib dose of 27%.
There are several additional questions: Why are the Kaplan Meier curves crossing after 12 months? What are these symptomatic skeletal events? Are they the same early versus late? Could radium-223 have raised the fracture risk early (symptomatic skeletal event as an adverse event) but helped later (prevented a cancer-related symptomatic skeletal event)? Or is there a subgroup that benefits and specifically benefits in the longer term?
Among all patients, the stratified progression-free survival hazard ratio was 1.37 (95% CI 0.74-2.53), and was 1.40 (95% CI 0.70-2.79) for overall survival:
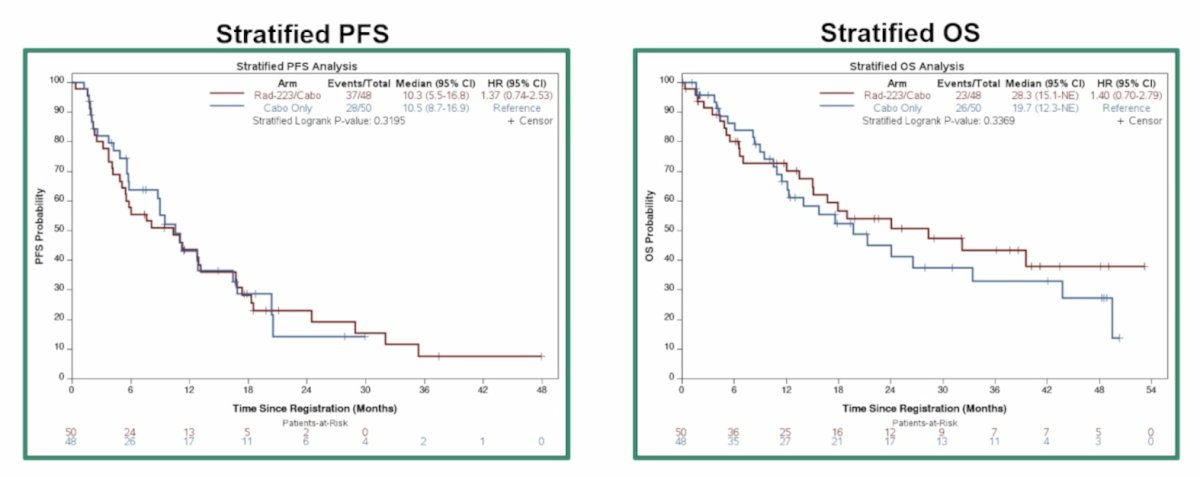
Why is there a crossing of the curves for the symptomatic skeletal event and overall survival curves, but not for progression-free survival? Dr. Voss notes that RECIST assessment does not estimate anticancer effect in the bone very well. Why are the overall survival curves crossing at 10 months? He states that this may be secondary to broad eligibility (1 bone metastasis was sufficient for enrolment, and any prior therapy was allowed), and that early deaths may be due to progression outside the bone.
Dr. Voss noted the following conclusions from the RADICAL trial:
- This is a first-of-its-kind randomized study to address this apparent area of need
- The study closed early due to an adverse symptomatic skeletal event-free survival signal on an early, preplanned futility analysis
- Differences in cabozantinib exposure were apparent and may have played an important role
- There may be a subgroup of patients who benefit from longer term, as suggested by late differences in the symptomatic skeletal event and overall survival curves
- Implications for future research include:
- Future analyses of RADICAL: Bone scans, biomarkers, and burden of disease
- Trials of radioligand therapy are here (targets: CD70, CAIX, PSMA)
Dr. Voss then discussed the trial of first-line cadonilimab + axitinib in advanced non-clear cell RCC. Contemporary regimens in non-clear cell RCC include lenvatinib + pembrolizumab, cabozantinib + nivolumab, and ipilimumab + nivolumab: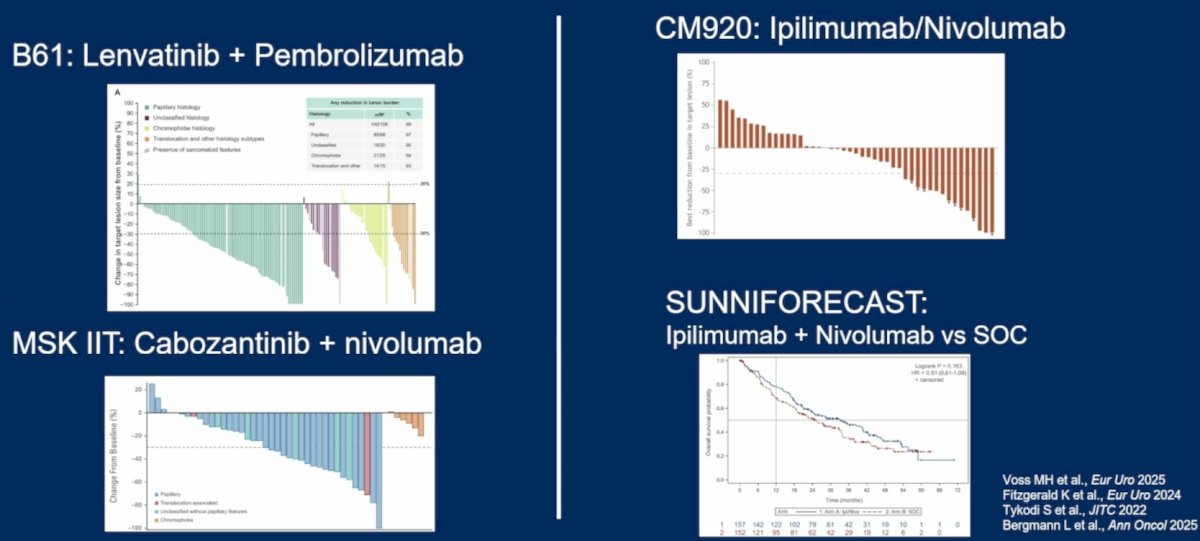
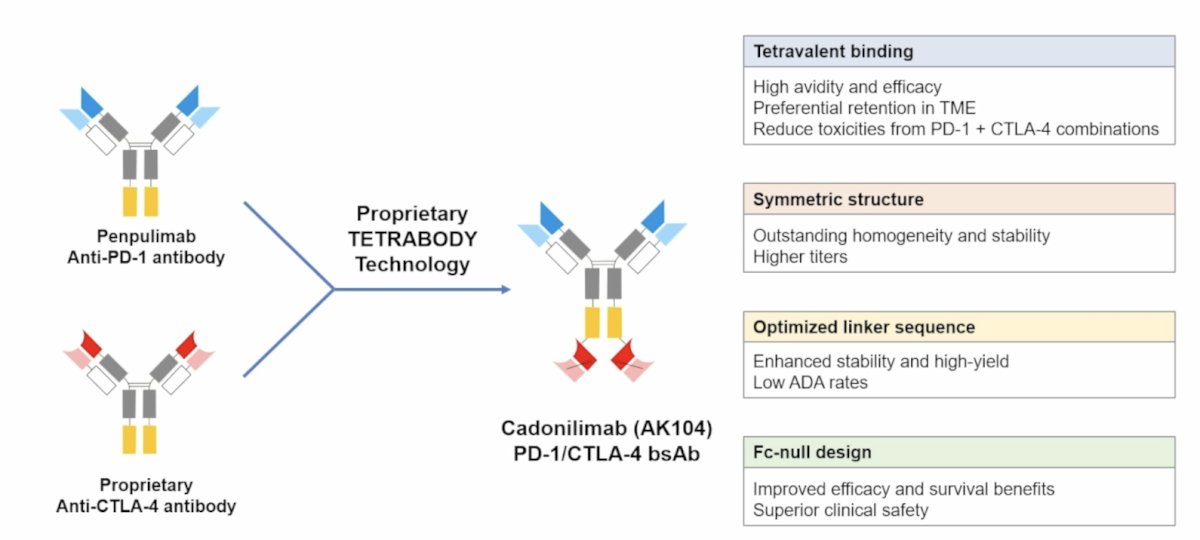
Cadonilimab, a bispecific PD-1/CTLA-4 antibody, has shown antitumor activity in various solid tumors, but its efficacy in RCC remains unknown:
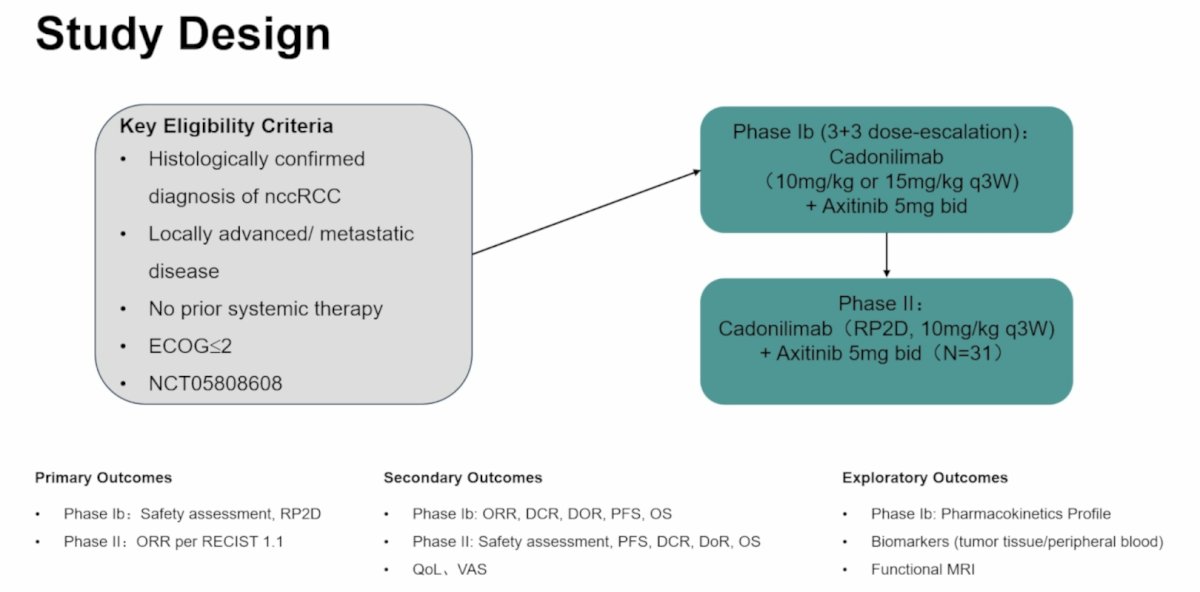
This open-label, multi-center, single-arm, phase Ib/II trial included patients with metastatic or unresectable treatment-naive non-clear cell RCC, regardless of PD-L1 status, to receive cadonilimab + axitinib 5 mg BID. In phase Ib, a 3+3 dose-escalation design was adopted, starting at 10 mg/kg every 3 weeks of cadonilimab with axitinib to evaluate safety. In phase II, an additional 31 patients were enrolled at the recommended phase II dose. The primary endpoints were safety assessment in phase Ib and objective response rate by RECIST v1.1 in phase II:
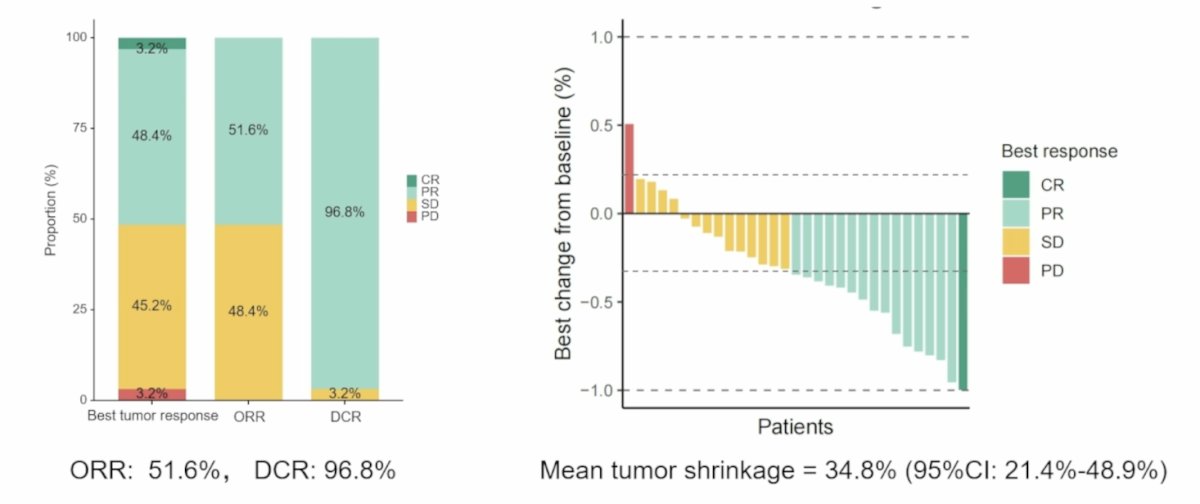
The median follow-up duration was 14.4 months. In phase Ib, no dose-limiting toxicities were observed, and adverse events were reported in 100% (6/6) of cases. Grade ≥ 3 treatment-related adverse events occurred in 66.7% (4/6) of cases, including proteinuria, hypertriglyceridemia, myasthenia gravis, diarrhea, and increased alanine aminotransferase. The recommended phase II dose for cadonilimab was 10 mg/kg. For secondary endpoints, objective response rate was 50% (2/4) and disease control rate was 100% (6/6). In phase II, the objective response rate was 51.6% (16/31), the disease control rate was 96.8% (30/31), and mean tumor shrinkage was 34.8% (95% CI 21.4%-48.9%):
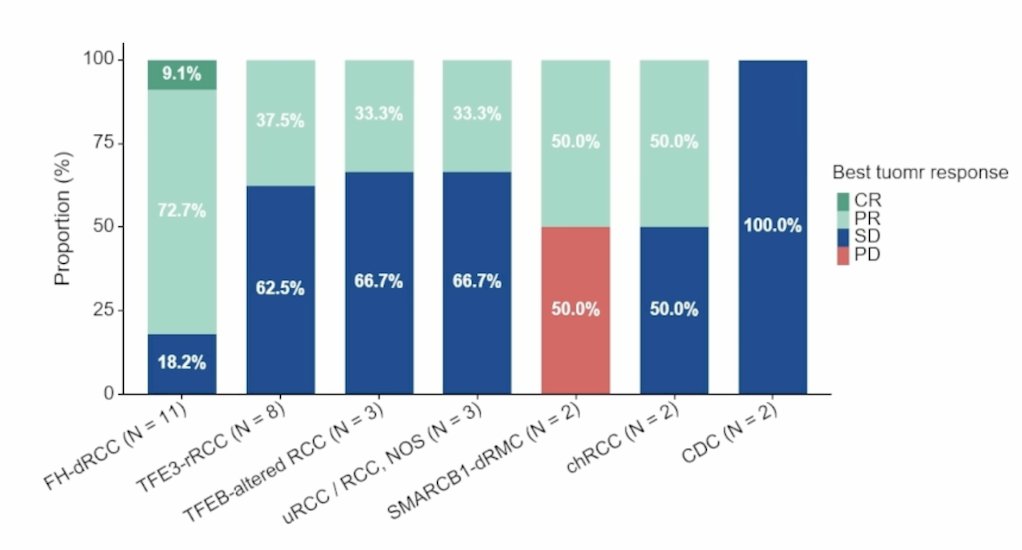
Among histopathological subtypes, the objective response rates were:
- FH-dRCC: 81.8% (9/11)
- TFE3-rRCC: 37.5% (3/8)
- TFEB-altered RCC: 33.3% (1/3)
- uRCC/RCC, NOS: 33.3% (1/3)
- SMARCB1-deficient RCC: 50% (1/2)
- chRCC: 50% (1/2)
- Collecting duct carcinoma: 0% (0/2)
Dr. Voss provided the following conclusions from the trial assessing first line cadonilimab + axitinib in advanced non-clear cell RCC:
- The study succeeded in demonstrating the safety and efficacy of this combination across a number of non-clear cell RCC variants
- Despite the integration of 3 targets, tolerance appeared very manageable
- Despite the integration of 3 targets, efficacy appeared on par with TKI + IO doublets in this space, including duration of response and complete response rate
- Implications for the clinic: this data further supports the current paradigm of using TKI + IO strategies broadly across the non-clear cell RCC space
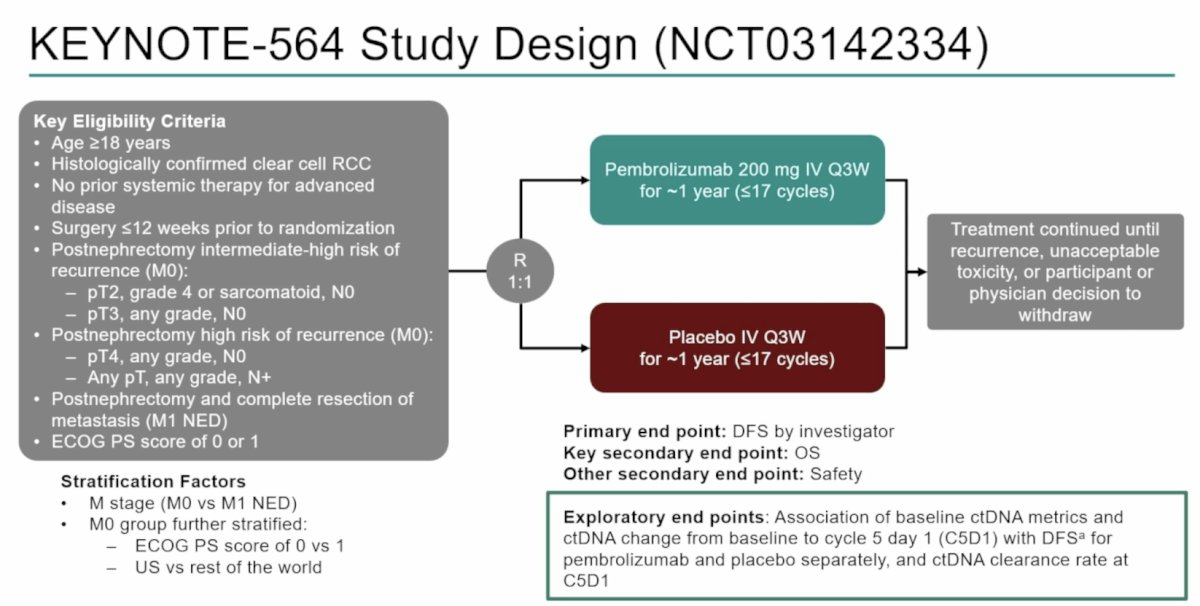
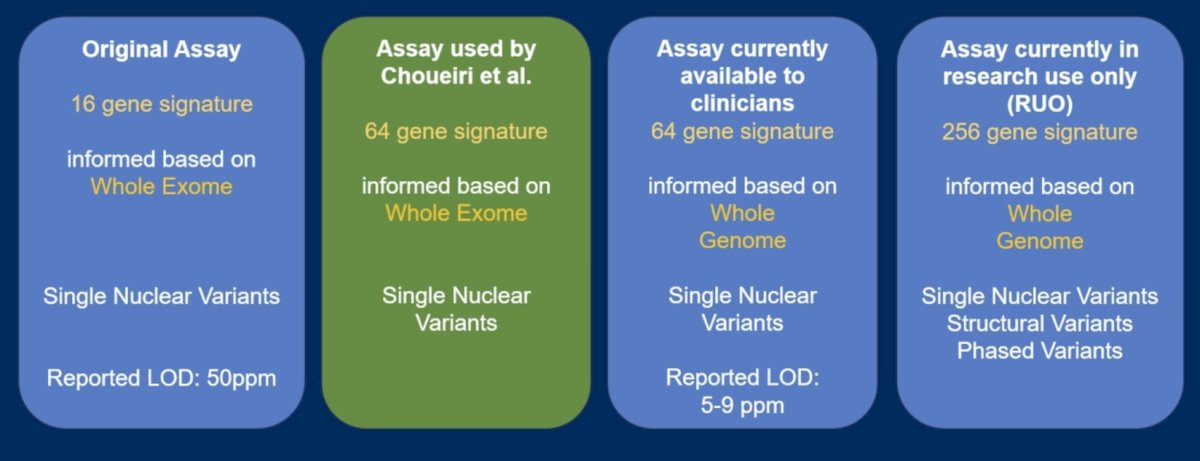
Finally, Dr. Voss discussed the KEYNOTE-564 trial, which enrolled participants with clear cell RCC at increased risk of recurrence post nephrectomy, randomizing patients 1:1 to pembrolizumab or placebo. ctDNA was evaluated using Natera’s Signatera RUO tissue-exome-based 16-plex and 64-plex ctDNA assays:
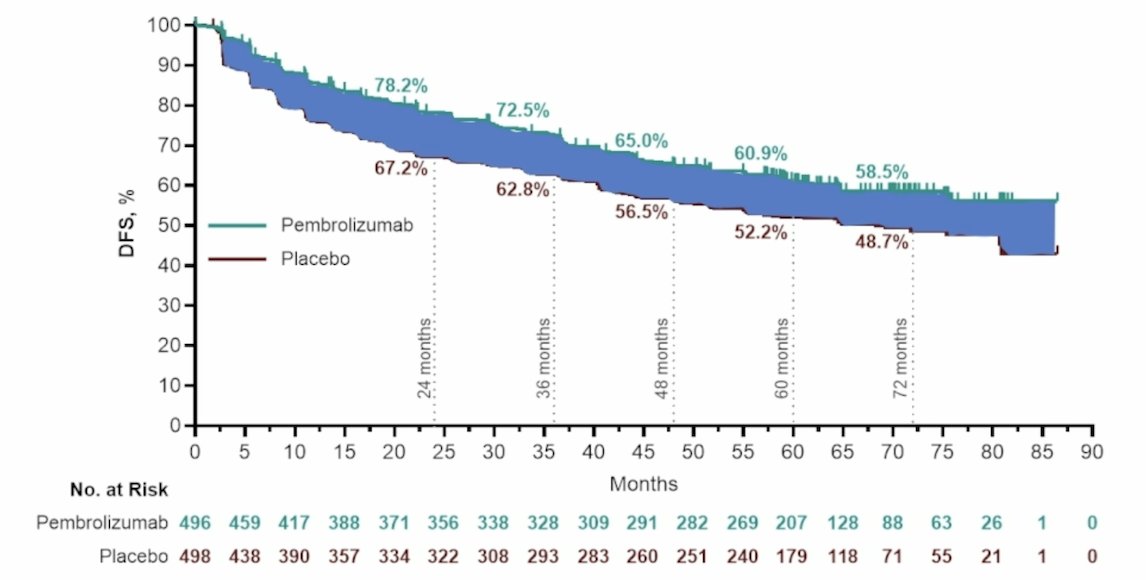
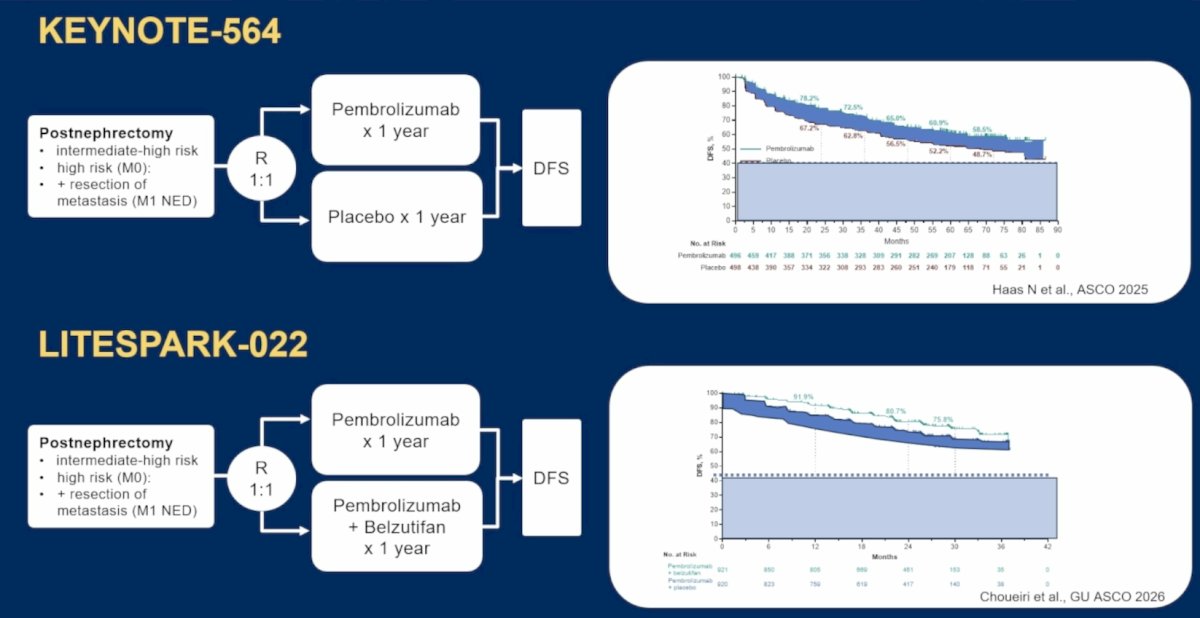
KEYNOTE-564 previously reported an improvement in disease-free survival with adjuvant pembrolizumab, however the proportion of patients that benefit versus placebo is modest:
Similarly, in the recently presented LITESPARK-022 trial assessing pembrolizumab + belzutifan versus pembrolizumab, the combination therapy improved disease-free survival, with a similar net benefit versus pembrolizumab alone:
Dr. Voss notes that there are several relevant questions:
- When should we escalate patients who need the second agent (belzutifan)?
- When should we de-escalate? Who are the KEYNOTE-564 patients who are surgically cured and do not need adjuvant therapy at all?
Dr. Voss notes that there have been evolving versions of the Signatera assay, as noted in the following figure:
The primary objectives of this analysis were to evaluate the association of baseline ctDNA status and ctDNA status change from baseline to cycle 5 day 1 (C5D1) with disease-free survival:
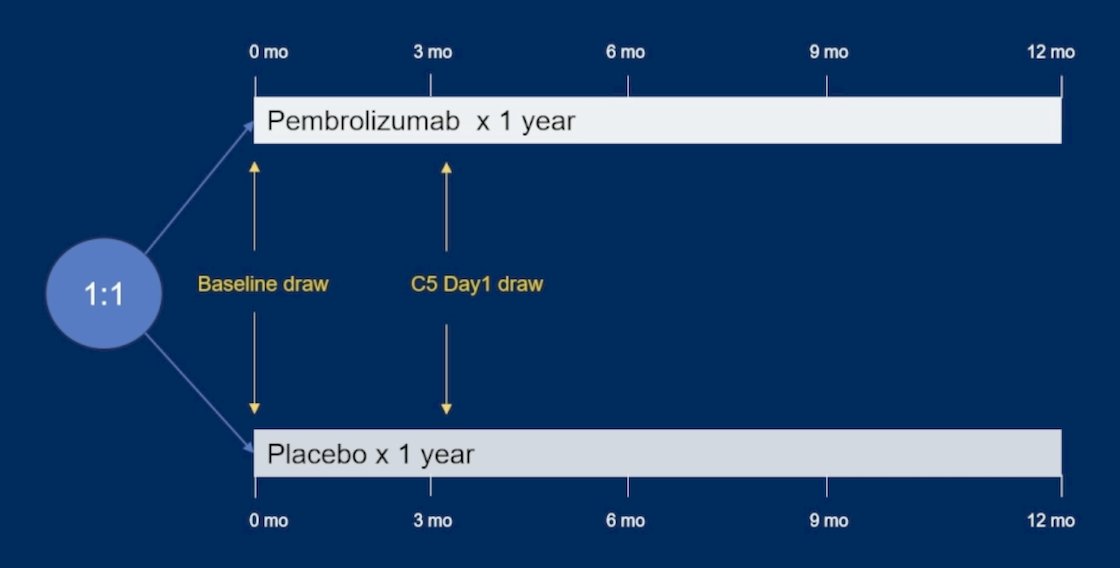
This timing allowed two analyses, and the ability to answer several objectives:
- Single time point analyses (baseline only)
- The proportion of ctDNA-positive versus negative at baseline
- The association of baseline ctDNA status (positive versus negative) and disease-free survival
- Clearance rate
- The association of change between time points (including clearance) and disease-free survival
In both treatment arms, ctDNA was detectable at baseline in 40 participants (5.4%) using the 16-plex assay and 60 participants (8.2%) using the 64-plex assay. By risk group, using the 16-plex assay, ctDNA was detectable at baseline in 26 of 642 (4.0%) intermediate-high risk participants, 10 of 53 (18.9%) high-risk participants, and 4 of 38 (10.5%) M1 NED participants. Using the 64-plex assay, ctDNA was detectable in 44 of 642 (6.9%) intermediate-high risk participants, 11 of 53 (20.8%) high-risk participants, and 5 of 38 (13.2%) M1 NED participants. For both assays, ctDNA positivity was negatively associated with disease-free survival in both the pembrolizumab and placebo arms (both p-values < 0.0001). Additionally, ctDNA status at baseline showed low sensitivity and high specificity to predict disease-free survival in both treatment arms:
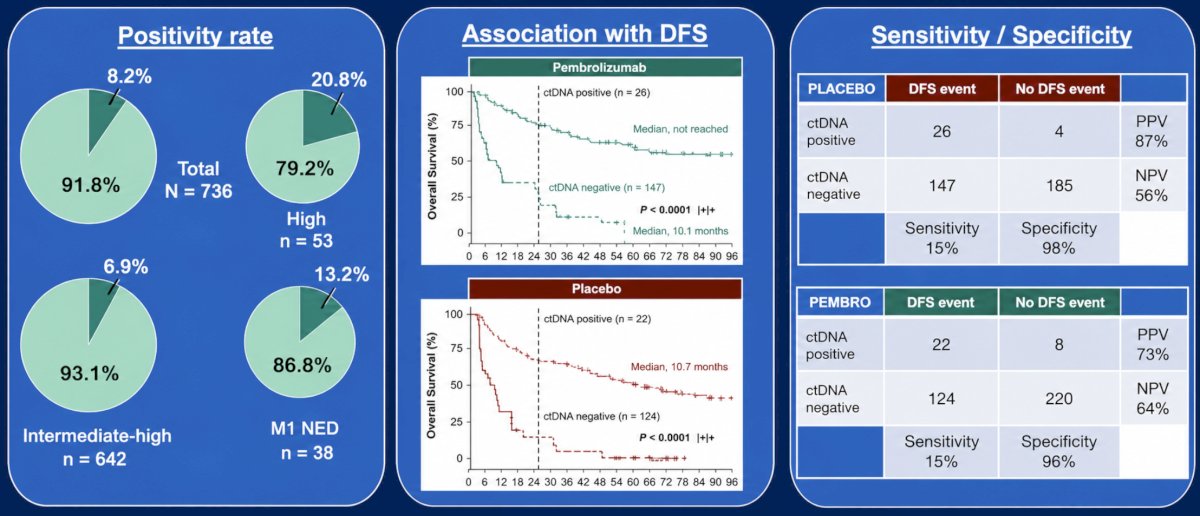
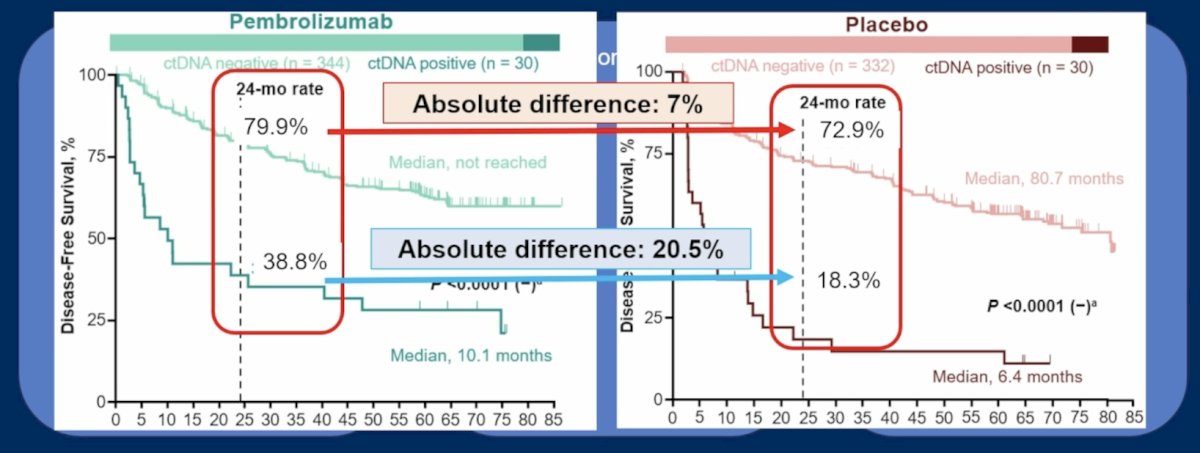
Dr. Choueiri concluded that the ctDNA positivity rate at baseline was associated with worse disease-free survival in both the pembrolizumab and placebo arms, irrespective of the number of variants (16 versus 64) utilized to test for ctDNA. Additionally, pembrolizumab led to improved outcomes regardless of baseline ctDNA positivity. Dr. Voss notes that among patients with ctDNA positivity, there is an absolute difference of 20.5% for those receiving pembrolizumab versus placebo, and only a 7% difference among those who are ctDNA negative:
Dr. Voss notes that there are other promising minimal residual disease strategies available, including: methylation-based profiling, fragmentomics, KIM-1, and combinations of the aforementioned options.
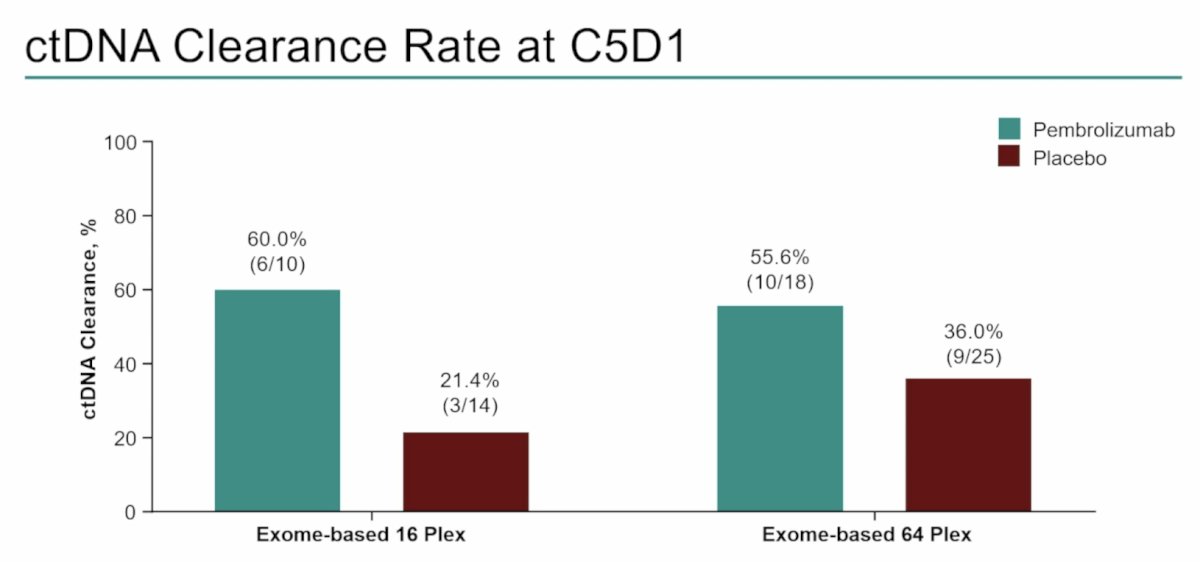
Of participants with detectable ctDNA at baseline and evaluable ctDNA at C5D1, ctDNA clearance at C5D1 occurred in 6 of 10 participants in the pembrolizumab arm and 3 of 14 participants in the placebo arm using the 16-plex assay, and 10 of 18 participants in the pembrolizumab arm and 9 of 25 participants in the placebo arm using the 64-plex assay:
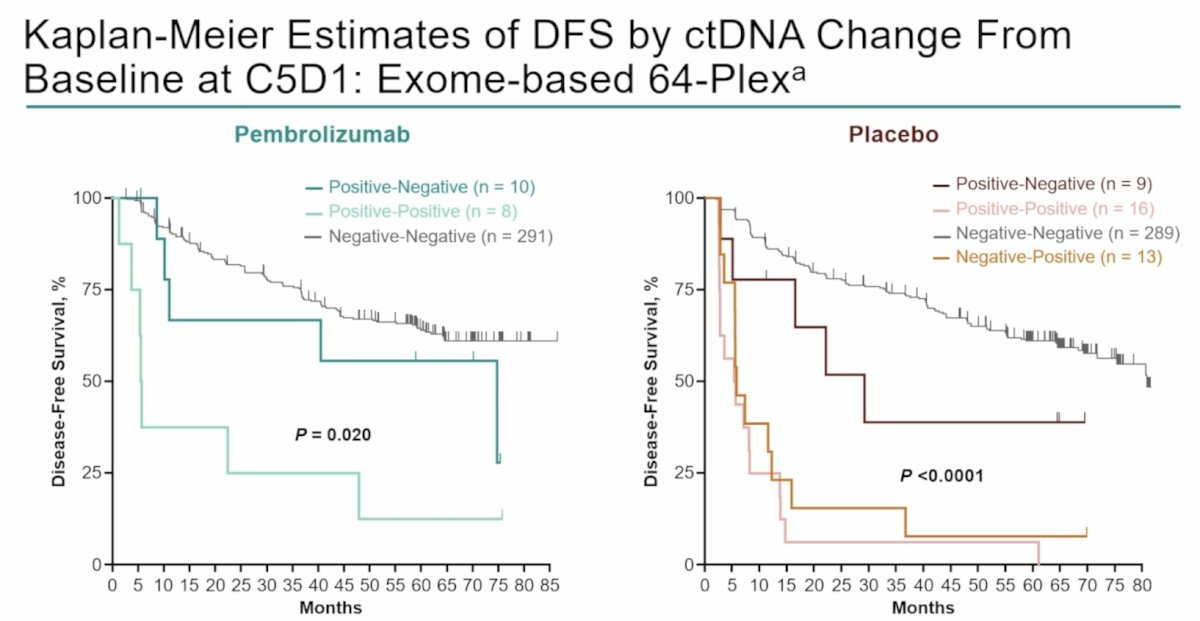
In both assays, ctDNA change from baseline at C5D1 was associated with disease-free survival for both pembrolizumab (p = 0.020) and placebo arms (p < 0.0001):
Dr. Voss concluded his discussant presentation with the following take-home points from the ctDNA analysis of KEYNOTE-564:
- The sensitivity / negative predictive value of the assay tested here was poor
- Specificity / positive predictive value was high in the placebo-treated patients (98% / 87%)
- For baseline positive patients, the 24-month recurrence rate was decreased by 20.5% with the addition of adjuvant pembrolizumab
- For the baseline negative patients, the size effect was markedly lower (7% reduction at 24 months)
- At 2 time points, expectedly, clearance of ctDNA confers favorable outcomes
- Implications for the clinic: post-nephrectomy ctDNA positivity suggests a greater likelihood of benefit from adjuvant pembrolizumab
- Implications for future research: prospective escalation, and especially de-escalation strategies, need to integrate minimal residual disease markers
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Associate Professor of Urology, Georgia Cancer Center, Wellstar MCG Health, @zklaassen_md on Twitter during the American Society of Clinical Oncology Genitourinary (ASCO) Annual Meeting held in Chicago, IL between May 29th and June 1st, 2026
References:
- Parker C, Nilsson S, Heinrich D, et al. Alpha emitter radium-223 and survival in metastatic prostate cancer. N Engl J Med 2013;369(3):213-223.
- Smith M, Parker C, Saad F, et al. Addition of radium-223 to abiraterone acetate and prednisone or prednisolone in patients with castration-resistant prostate cancer and bone metastases (ERA 223): A randomized, double-blind, placebo-controlled, phase 3 trial. Lancet Oncol 2019 Mar;20(3):408-419.
- Tombal B, Choudhury A, Saad F, et al. Enzalutamide plus radium-223 in metastatic castration-resistant prostate cancer: results of the EORTC 1333/PEACE-3 trial. Ann Oncol. 2025 Sep;36(9):1058-1067.
- McKay RR, Bosse D, Gray KP, et al. Radium-223 dichloride in combination with vascular endothelial growth factor-targeting therapy in advanced renal cell carcinoma with bone metastases. Clin Cancer Res. 2018 Sep 1;24(17):4081-4088.
- Choueiri TK, Escudier B, Powles T, et al. Cabozantinib versus Everolimus in Advanced Renal-Cell Carcinoma. N Engl J Med 2015;373(19):1814-1823.