(UroToday.com) The 2026 American Society of Clinical Oncology (ASCO) Annual Meeting was host to State-of-the-Art Session on advances in the perioperative management of bladder and kidney cancers. Dr. Rana McKay delivered a state-of-the-art overview of neoadjuvant treatment strategies in renal cell carcinoma (RCC), reviewing historical experience with targeted therapy, emerging perioperative immunotherapy data, evolving pathologic response endpoints, and ongoing clinical trials seeking to define the role of neoadjuvant therapy in localized and locally advanced disease.
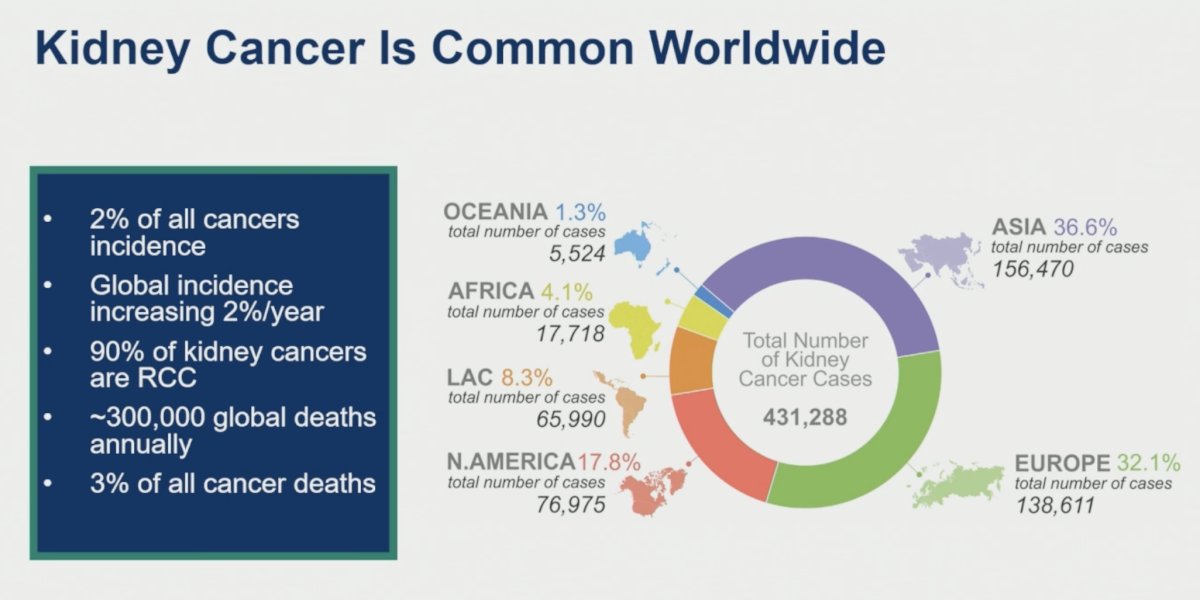
Kidney cancer remains a significant global health burden, accounting for approximately 2% of all cancer diagnoses, with incidence increasing by roughly 2% annually worldwide. RCC comprises approximately 90% of kidney cancers and contributes to nearly 300,000 deaths each year. Although most patients present with localized disease, outcomes remain heterogeneous, emphasizing the need for accurate recurrence risk stratification and improved perioperative treatment approaches.
Several tools have been developed to estimate recurrence risk following nephrectomy. Preoperative models include the Karakiewicz, Raj/Kattan (MSKCC), and Yaycioglu nomograms, incorporating factors such as age, symptoms, tumor size, and clinical TNM stage. Postoperative models such as ASSURE, SSIGN, and Leibovich integrate pathologic stage, grade, histology, necrosis, sarcomatoid features, and performance status to predict recurrence and survival outcomes.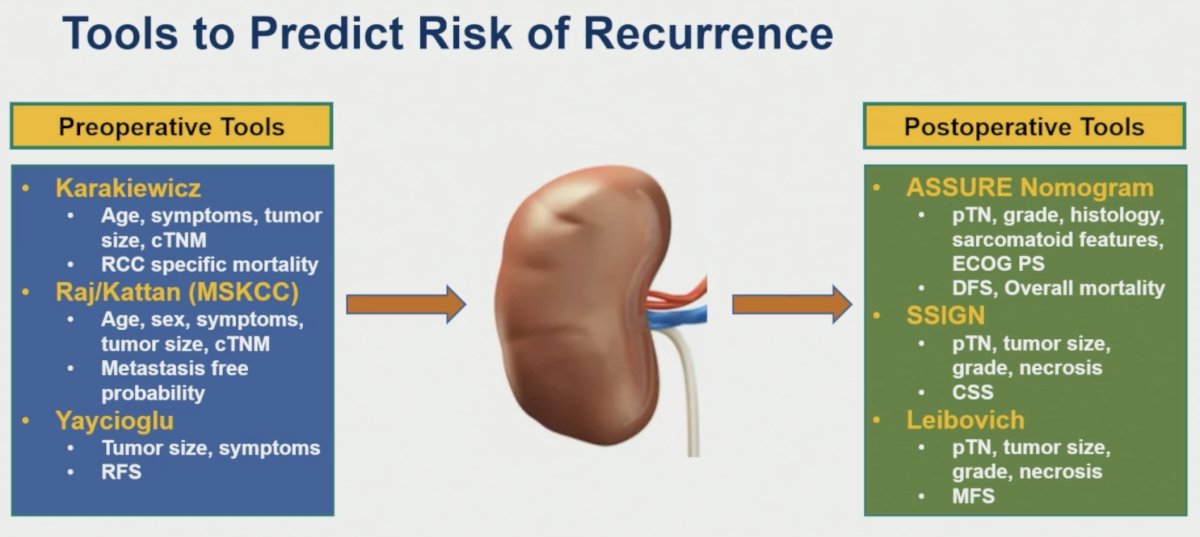
Dr. McKay highlighted the rationale for perioperative systemic therapy, emphasizing that neoadjuvant approaches offer several theoretical advantages over adjuvant treatment alone. Goals include tumor downstaging, improved surgical resectability, reduction in recurrence risk, and the opportunity to assess in vivo treatment response.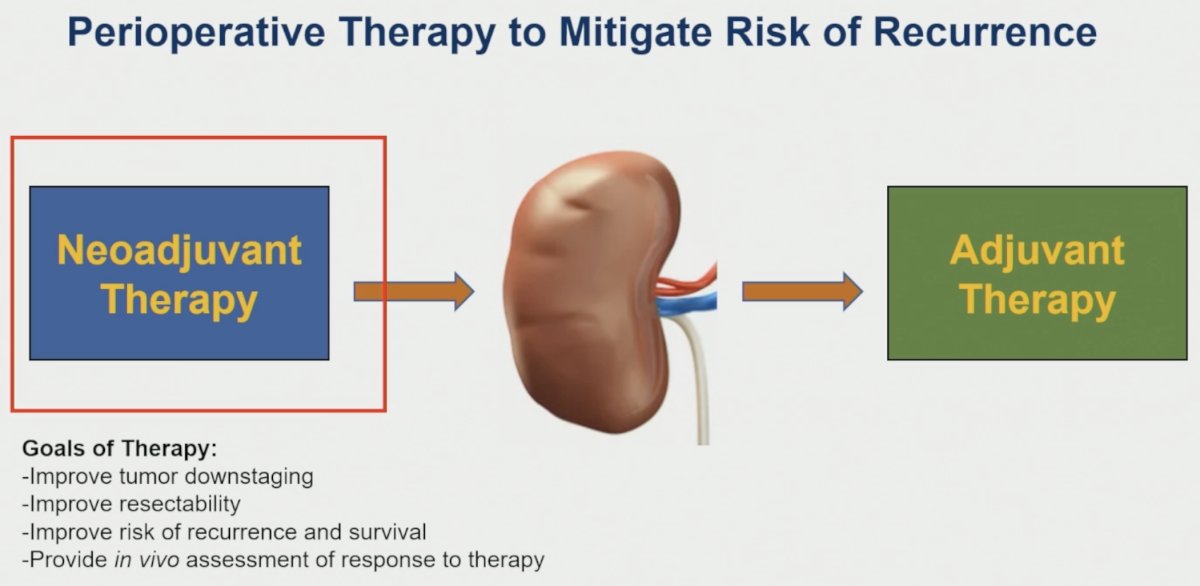
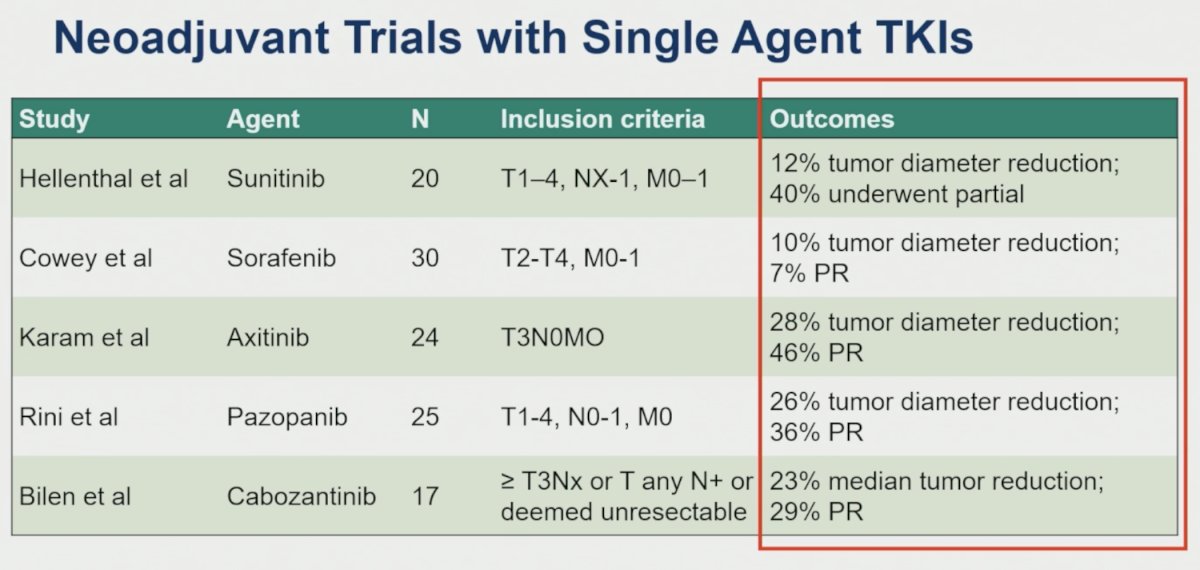
Early neoadjuvant experiences primarily involved single-agent VEGF-targeted tyrosine kinase inhibitors (TKIs). Across several small studies, tumor shrinkage was consistently observed:
- Hellenthal et al evaluated sunitinib in 20 patients with T1–4, NX–1, M0–1 disease, demonstrating a 12% reduction in tumor diameter, with 40% achieving partial response.
- Cowey et al reported a 10% reduction in tumor diameter and a 7% partial response rate among 30 patients treated with sorafenib.
- Karam et al evaluated axitinib in 24 patients with cT3N0M0 disease, reporting a 28% tumor diameter reduction and a 46% partial response rate.
- Rini et al treated 25 patients with pazopanib and observed a 26% reduction in tumor diameter with a 36% partial response rate.
- Bilen et al evaluated cabozantinib in 17 patients with ≥T3 disease, node-positive disease, or tumors considered unresectable, reporting a median 23% tumor reduction and a 29% partial response rate.
From these studies, several important lessons emerged:
- Neoadjuvant TKI therapy proved feasible and generally well tolerated, with modest but variable radiographic responses
- Pathologic response was not systematically evaluated, pathologic complete responses were exceedingly rare, and disease progression during therapy was uncommon
- While nephron-sparing surgery could occasionally be facilitated, most studies were methodologically limited and lacked robust long-term outcome reporting.
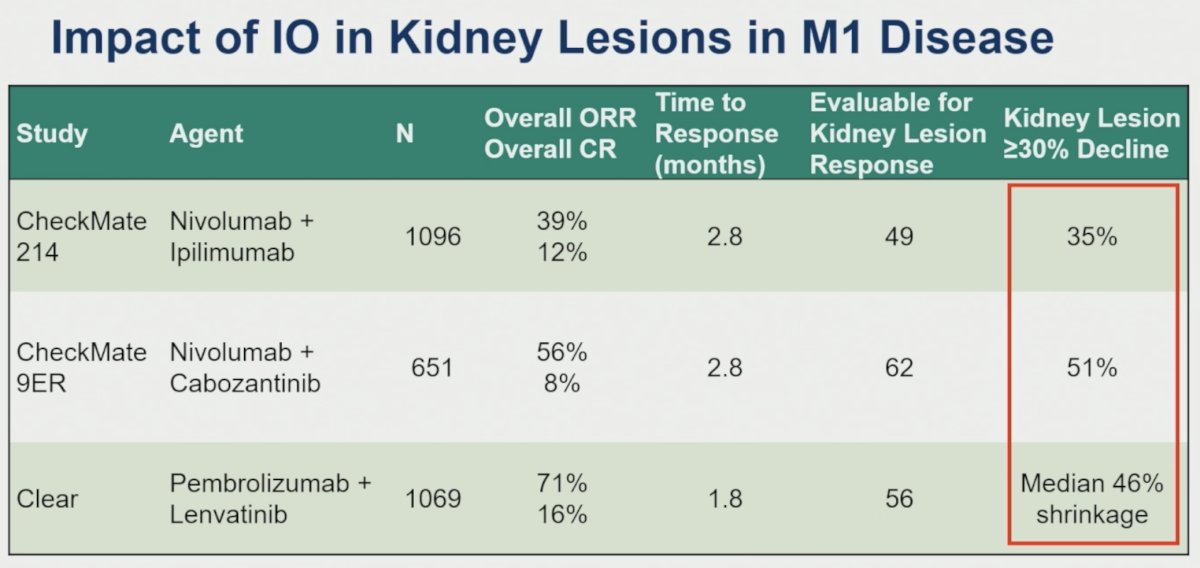
The emergence of immune checkpoint inhibitors has renewed interest in neoadjuvant approaches. Dr. McKay reviewed evidence from metastatic RCC demonstrating meaningful activity of immunotherapy within primary kidney lesions. In CheckMate-214,1 nivolumab plus ipilimumab achieved a 39% objective response rate with a 12% complete response rate overall; among evaluable kidney lesions, 35% experienced at least a 30% reduction. In CheckMate-9ER, nivolumab plus cabozantinib yielded a 56% objective response rate and an 8% complete response rate, with 51% of evaluable kidney lesions demonstrating ≥30% shrinkage.2 In CLEAR, pembrolizumab plus lenvatinib achieved a 71% objective response rate and a 16% complete response rate, with a median 46% reduction in kidney lesion size.3
Additional retrospective data suggest that neoadjuvant immunotherapy may generate meaningful pathologic responses. In a multi-institutional retrospective series of 52 patients treated with immunotherapy prior to nephrectomy, 44% experienced pathologic downstaging and 13% achieved a pathologic complete response. Downstaging rates increased with higher baseline tumor stage, reaching 85% among patients with T4 disease.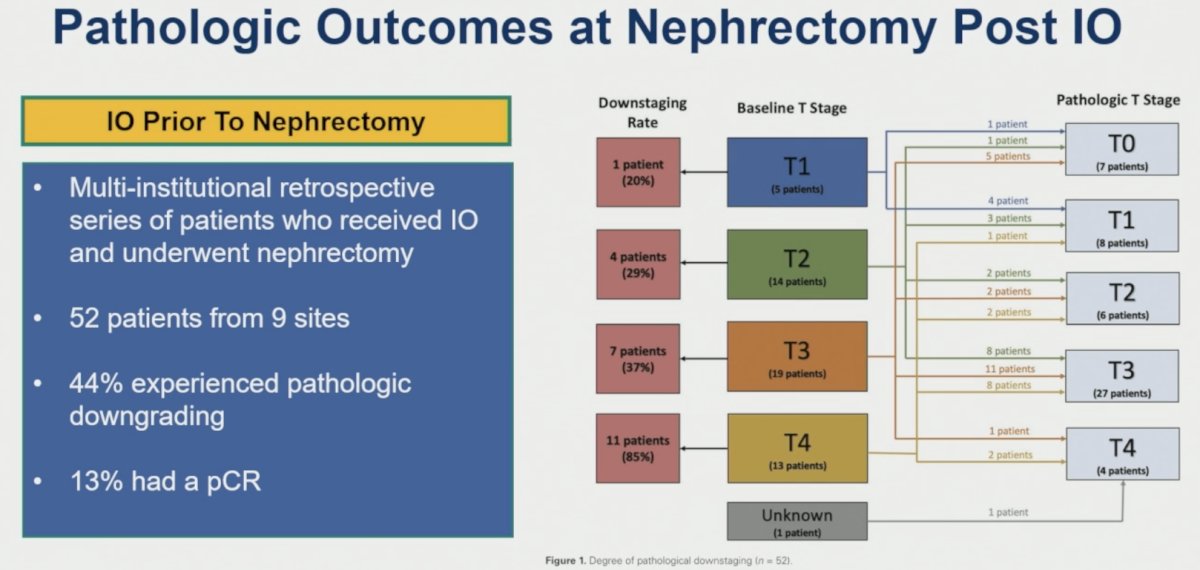
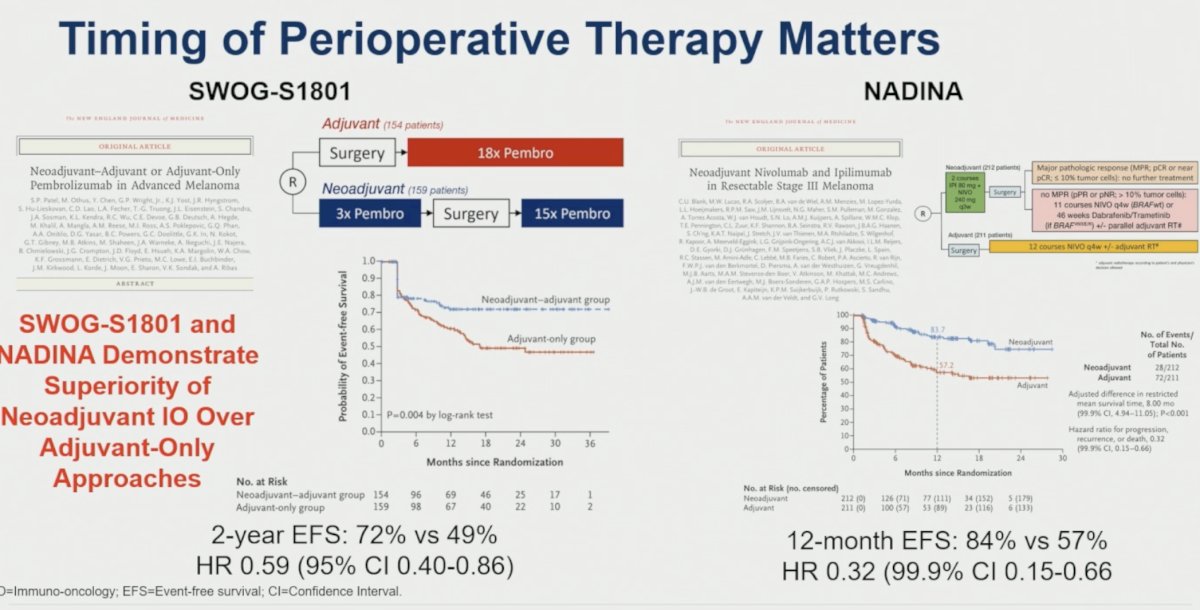
Dr. McKay emphasized that the timing of systemic therapy may matter. She highlighted evidence from melanoma showing the superiority of neoadjuvant-containing approaches over adjuvant-only treatment. In SWOG S1801, neoadjuvant plus adjuvant pembrolizumab improved 2-year event-free survival compared with adjuvant pembrolizumab alone (72% versus 49%; HR 0.59, 95% CI 0.40–0.86).4 Similarly, the NADINA study demonstrated superior 12-month event-free survival for neoadjuvant nivolumab/ipilimumab-based therapy compared with adjuvant treatment alone (84% versus 57%; HR 0.32, 99.9% CI 0.15–0.66).5 These studies provide proof-of-principle that neoadjuvant immunotherapy can generate meaningful antitumor immune responses and improve long-term outcomes.
Dr. McKay then reviewed contemporary neoadjuvant and perioperative immunotherapy studies in RCC.
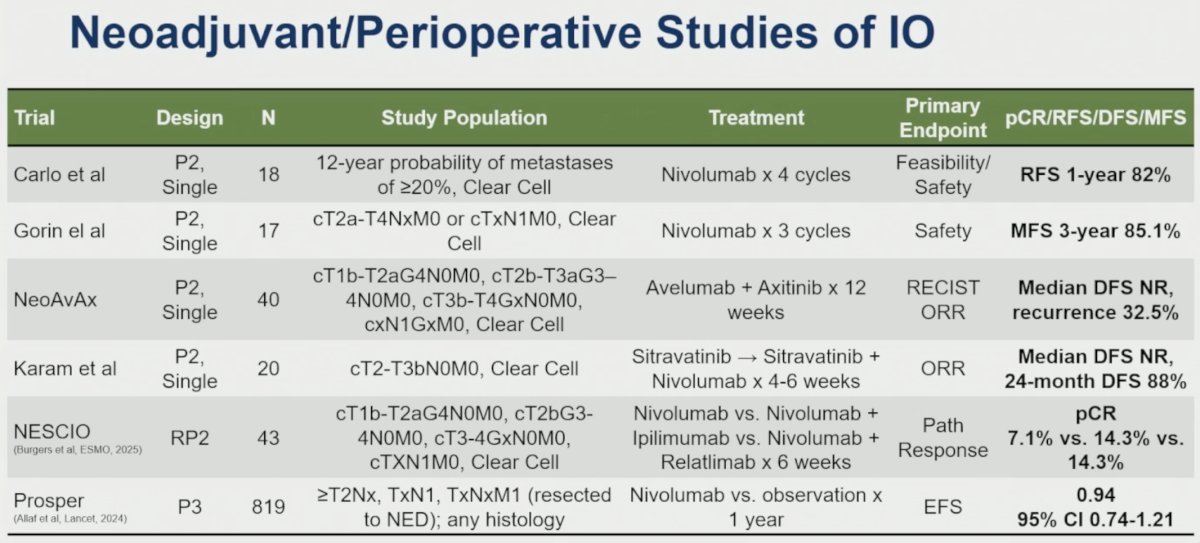
- Among early phase studies, Carlo et al evaluated four cycles of nivolumab in 18 high-risk clear-cell RCC patients, reporting a 1-year recurrence-free survival rate of 82%.
- Gorin et al treated 17 patients with three cycles of nivolumab, observing a 3-year metastasis-free survival rate of 85.1%.
- The NeoAvAx study enrolled 40 patients with high-risk localized clear-cell RCC and evaluated avelumab plus axitinib for 12 weeks prior to surgery. Median disease-free survival had not yet been reached, although recurrence occurred in 32.5% of patients.
- Karam et al evaluated sitravatinib followed by sitravatinib plus nivolumab in 20 patients with localized clear-cell RCC, reporting a 24-month disease-free survival rate of 88%.
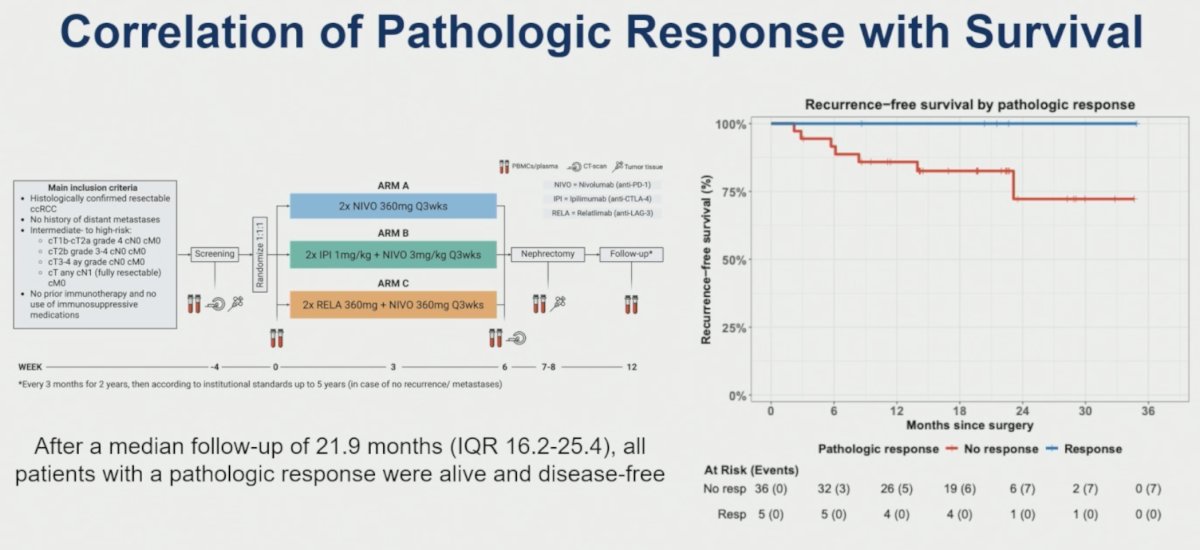
- The NESCIO randomized phase II trial compared nivolumab alone, nivolumab plus ipilimumab, and nivolumab plus relatlimab. Pathologic complete response rates were 7.1%, 14.3%, and 14.3%, respectively, providing evidence that combination immunotherapy strategies may enhance pathologic response.6
- In contrast, the phase III PROSPER trial failed to demonstrate a significant event-free survival benefit for perioperative nivolumab versus observation among 819 patients with high-risk RCC (HR 0.94, 95% CI 0.74–1.21).7
A major challenge in RCC remains the lack of validated pathologic response endpoints. Drawing from experience in melanoma, Dr. McKay discussed the International Neoadjuvant Melanoma Consortium (INMC) framework, which categorizes pathologic response according to the percentage of viable tumor remaining in the treated tumor bed:
- Pathologic complete response (pCR): 0% viable tumor
- Near pCR: ≤10% viable tumor
- Pathologic partial response (pPR): >10–50% viable tumor
- Pathologic non-response (pNR): >50% viable tumor
She emphasized that useful pathologic endpoints must be standardized, reproducible, and correlate with clinical outcomes.
To address this need, the International Neoadjuvant Kidney Cancer Consortium (INKCC) recently proposed RCC-specific pathologic response criteria. These guidelines arose from recognition that pathologic response reporting in RCC has historically been inconsistent; among 119 RCC studies reviewed, only 4% described how pathologic response was assessed and only 7% used quantitative measurements. The INKCC criteria adapt melanoma-derived thresholds and recommend rigorous gross and microscopic sampling methods, including complete submission of tumors <4 cm and extensive sampling of larger tumors. Importantly, whether pathologic response predicts event-free or overall survival in RCC remains unproven.
Preliminary evidence supporting pathologic response as a surrogate endpoint comes from the NESCIO study. After a median follow-up of 21.9 months, all patients achieving a pathologic response remained alive and disease-free, whereas recurrences were observed among patients without a pathologic response.
Dr. McKay concluded by highlighting several ongoing efforts designed to advance the field.
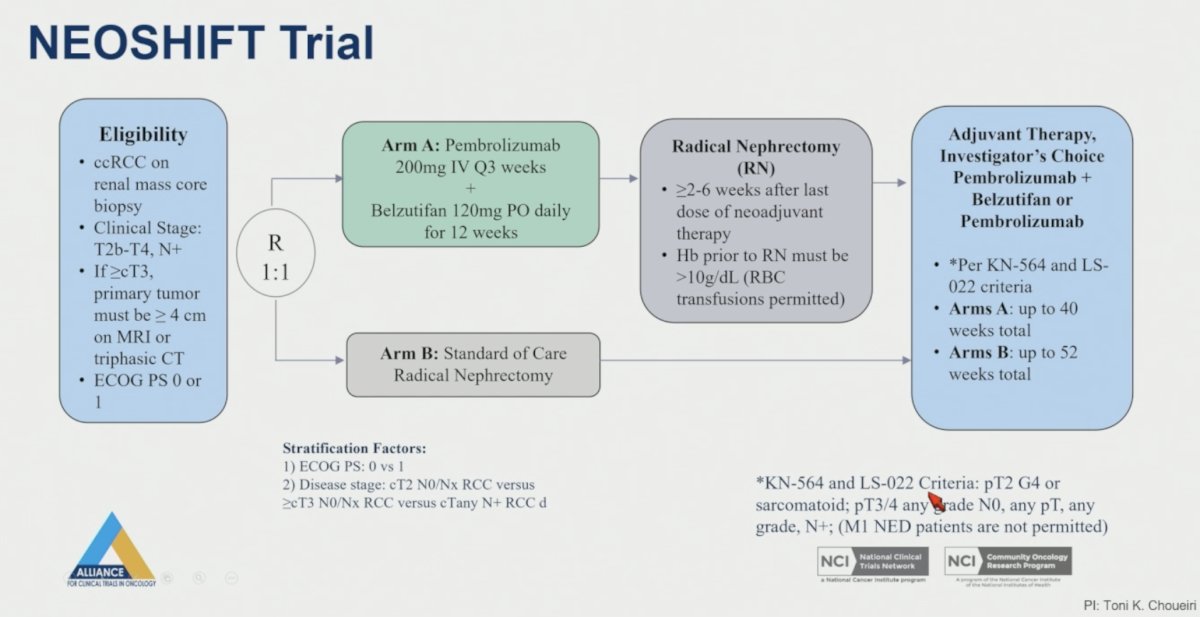
- The Alliance-sponsored NEOSHIFT trial is evaluating neoadjuvant pembrolizumab plus belzutifan before nephrectomy in patients with cT2b–T4 and/or node-positive clear-cell RCC, followed by risk-adapted adjuvant therapy.
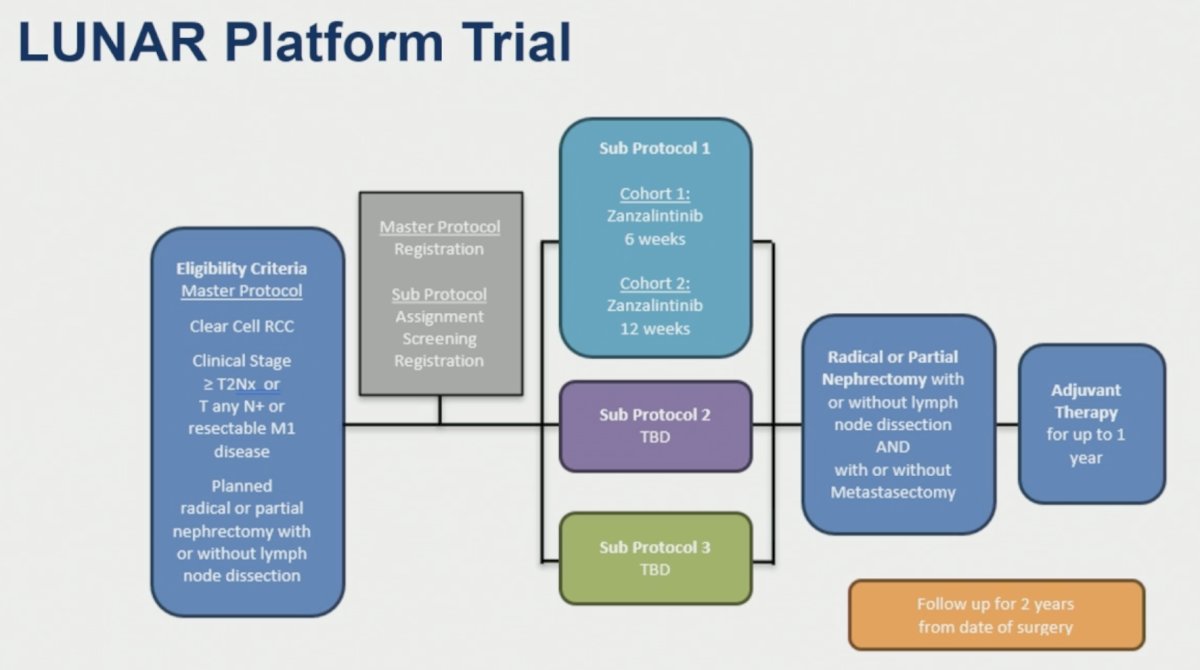
- The LUNAR platform trial is testing multiple neoadjuvant strategies in patients with clinical stage T2N× disease, node-positive disease, or resectable metastatic RCC, with adaptive subprotocols and integrated perioperative treatment approaches.
In her concluding remarks, Dr. McKay emphasized three key takeaways. First, neoadjuvant therapy in RCC remains investigational. Second, combination immunotherapy-based strategies have demonstrated encouraging pathologic response signals. Third, the development and validation of a standardized RCC-specific pathologic response framework that correlates with long-term outcomes remains a critical unmet need for the field.
Presented by: Rana R. McKay, MD, Professor of Medicine and Urology, Department of Medicine, University of California, San Diego Moores Cancer Center, La Jolla, CA, USA
Written by: Rashid K. Sayyid, MD, MSc, Assistant Professor, Urologic Oncologist, Department of Urology at The University of Arizona and Banner University Medical Center, Tucson, AZ – @rksayyid on X during the American Society of Clinical Oncology Genitourinary (ASCO) Annual Meeting held in Chicago, IL between May 29th and June 1st, 2026
References:- Motzer RJ, Tannir NM, McDermott DF, et al. Nivolumab plus ipilimumab versus sunitinib in advanced renal-cell carcinoma. N Engl J Med. 2018;378(14):1277-1290.
- Choueiri TK, Powles T, Burotto M, et al. Nivolumab plus cabozantinib for advanced renal-cell carcinoma. N Engl J Med. 2021;384(9):829-841.
- Motzer R, Alekseev B, Rha SY, et al. Lenvatinib plus pembrolizumab or everolimus for advanced renal cell carcinoma. N Engl J Med. 2021;384(14):1289-1300.
- Patel SP, Othus M, Chen Y, Wright GP, Yost K, Hyngstrom J, et al. Neoadjuvant–adjuvant or adjuvant-only pembrolizumab in advanced melanoma. N Engl J Med. 2023;388(9):813-823.
- Blank CU, Rozeman EA, Fanchi LF, et al. Neoadjuvant nivolumab plus ipilimumab in resectable stage III melanoma. N Engl J Med. 2024;391:1696-1708.
- Burgers F, de Ruijter A, Graafland NM, et al. Neoadjuvant immunotherapy in locally advanced clear cell renal cell carcinoma at risk for recurrence or distant metastases: the randomized phase II NESCIO trial. Ann Oncol. 2025;36(Suppl 2):S1636-S1637.
- Allaf ME, Kim SE, Master V, et al. Perioperative nivolumab versus observation in patients with renal cell carcinoma undergoing nephrectomy (PROSPER ECOG-ACRIN EA8143): an open-label, randomised, phase 3 study. Lancet Oncol. 2024;25(8):1038-1052.