(UroToday.com) The 2026 American Society of Clinical Oncology (ASCO) Annual Meeting was host to a session on new approaches to curing bladder and kidney cancer. Dr. Elizabeth Nally presented a study of decision regret and toxicity perception following adjuvant pembrolizumab in renal cell carcinoma (RCC).
Adjuvant pembrolizumab has demonstrated significant disease-free and overall survival benefits in RCC;1 however, unlike traditional systemic therapies, some immunotherapy-related toxicities may persist long after treatment discontinuation. The investigators noted that CTCAE criteria were not designed to capture the long-term impact of ICIs and that despite clinically significant toxicity rates reported across adjuvant ICI trials, Health-Related Quality of Life (HRQoL) analyses have frequently demonstrated minimal differences between treatment and placebo arms. This discrepancy raises the possibility that conventional toxicity classification systems and standard HRQoL methodologies may inadequately characterize the long-term consequences of immune-related toxicity.
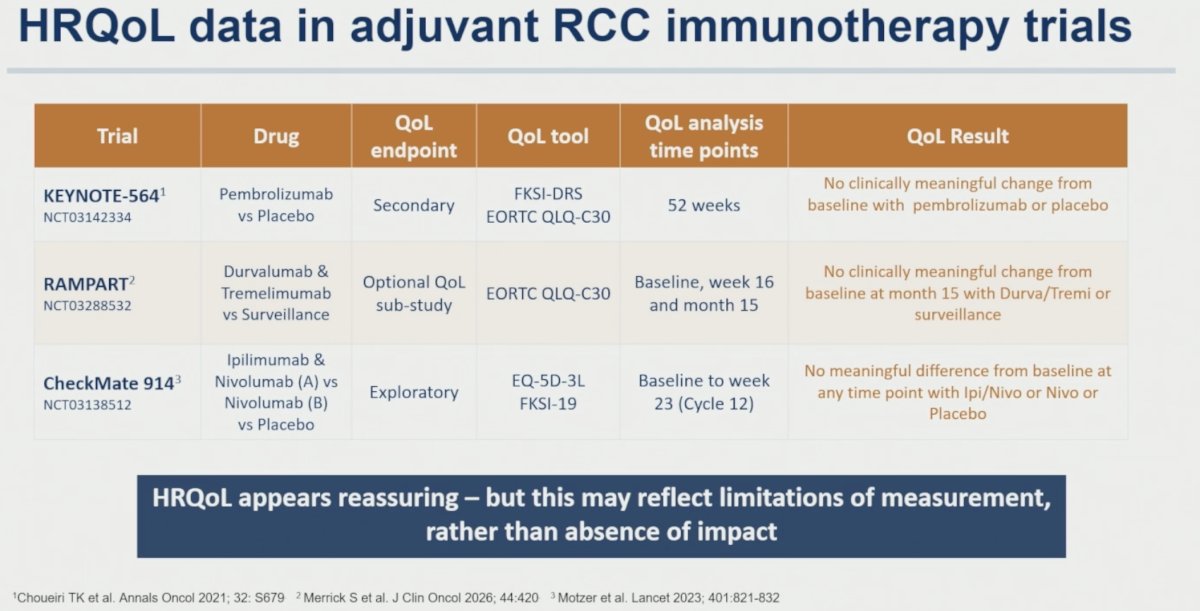
To support this premise, the authors reviewed HRQoL findings from major adjuvant RCC immunotherapy trials. In KEYNOTE-564, no clinically meaningful change from baseline was observed with pembrolizumab or placebo at 52 weeks using FKSI-DRS and EORTC QLQ-C30 instruments. Similarly, RAMPART demonstrated no clinically meaningful change from baseline at month 15 with durvalumab/tremelimumab versus surveillance, while CheckMate 914 reported no meaningful difference from baseline at any time point among treatment groups. As highlighted by the investigators, “HRQoL appears reassuring – but this may reflect limitations of measurement, rather than absence of impact.”
Several limitations of conventional HRQoL assessment were identified. Existing tools may not adequately capture concerns unique to the adjuvant setting, where patient expectations differ substantially from those in metastatic disease. Patients who discontinue therapy due to toxicity or who become unwell may fail to complete QoL assessments, creating informative missingness. Patients who experience disease recurrence are often lost from longitudinal HRQoL follow-up, potentially biasing analyses toward individuals with more favorable outcomes. Finally, traditional toxicity grading systems were developed to capture acute toxicity and provide a limited assessment of patient perception and functional impact.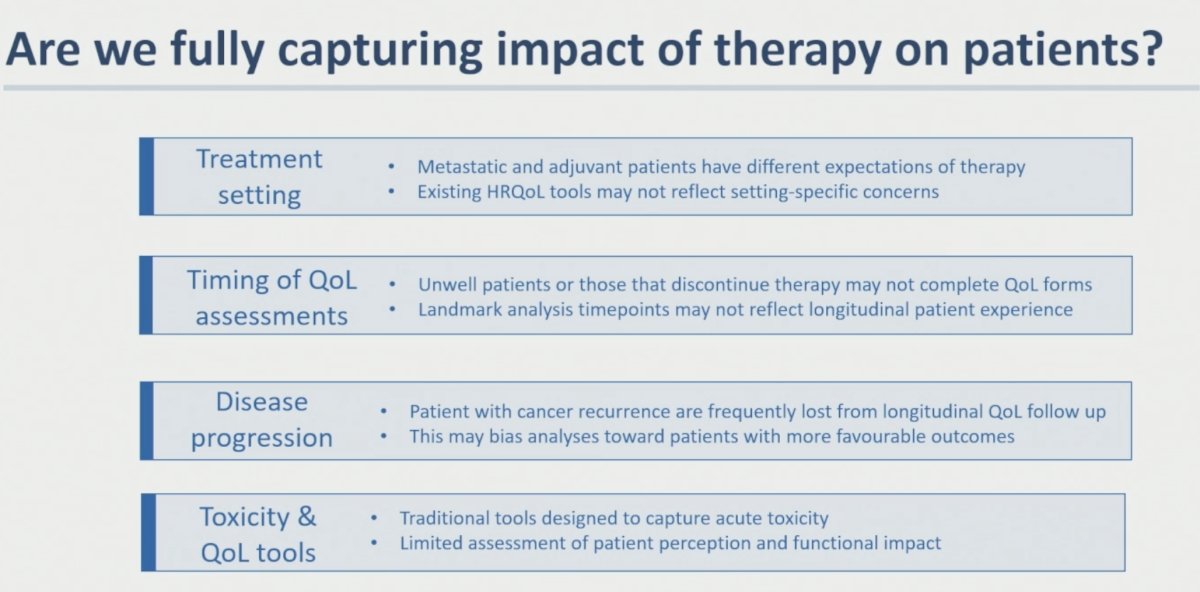
The study consisted of three components. First, the investigators developed a patient-defined toxicity framework through a patient and public involvement and engagement (PPIE) workshop that informed toxicity category definitions and duration thresholds. This framework was subsequently piloted in 104 RCC patients treated with ICIs and refined through an independent patient validation group. Second, the framework was applied in an exploratory post hoc analysis of the phase III IMmotion010 trial. Third, a decision regret analysis was performed among RCC patients who had received adjuvant immune checkpoint inhibitor therapy.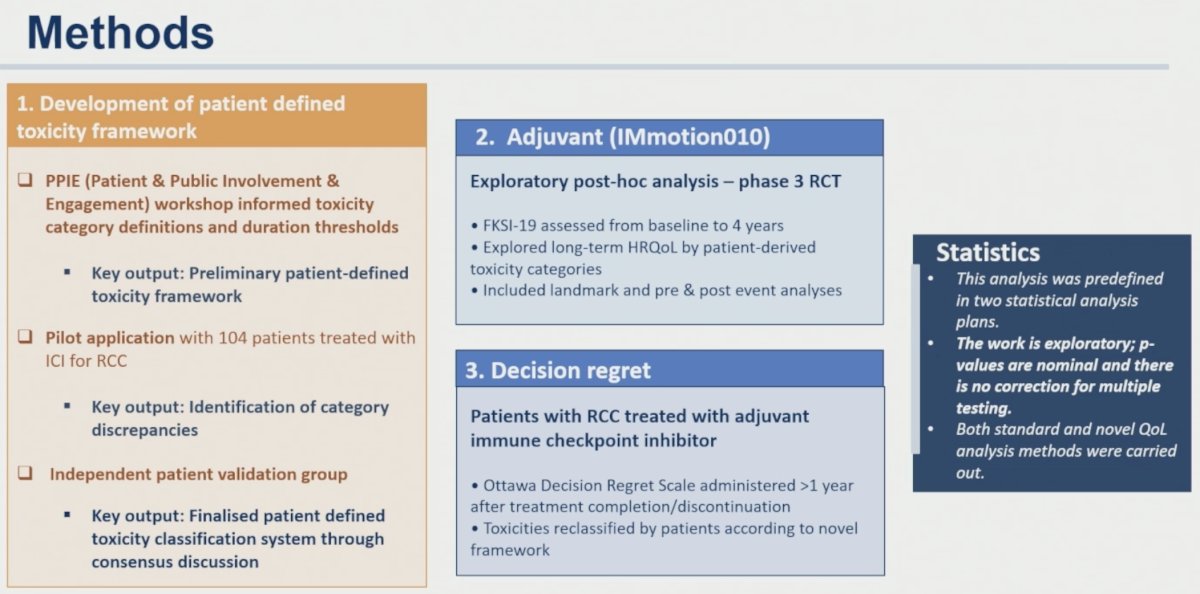
The final patient-defined toxicity framework classified toxicities into four categories:
- Life-changing (LC): adverse events with permanent or long-lasting impact on daily life and functioning
- Significant long-term (SLT): clinically significant adverse events persisting beyond 90 days
- Significant short-term (SST): clinically significant adverse events resolving within 90 days
- Non-significant (NS): mild adverse events or no adverse events with minimal impact on well-being or daily functioning
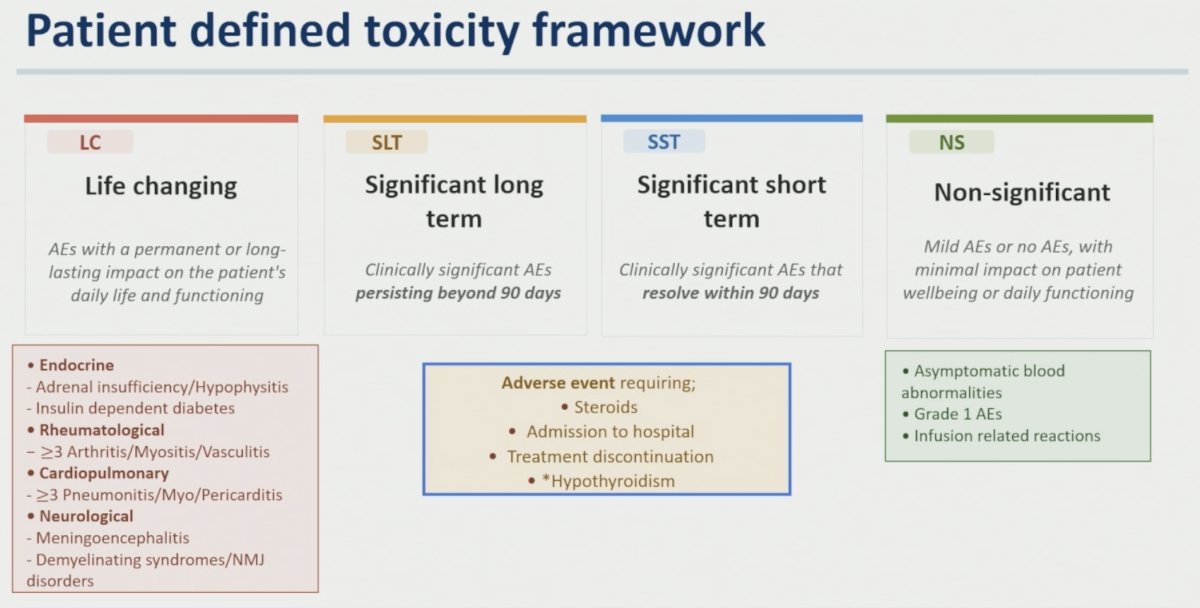
Examples of life-changing toxicities included adrenal insufficiency/hypophysitis, insulin-dependent diabetes, severe rheumatologic toxicity (≥ grade 3 arthritis/myositis/vasculitis), severe cardiopulmonary toxicity (≥ grade 3 pneumonitis/myocarditis/pericarditis), and neurologic toxicities such as meningoencephalitis or demyelinating syndromes. Significant long-term toxicity categories included adverse events requiring steroids, hospitalization, or treatment discontinuation, whereas asymptomatic laboratory abnormalities, grade 1 adverse events, and infusion reactions were generally classified as non-significant.
The IMmotion010 HRQoL analysis included 532 patients with available HRQoL data among 778 randomized patients. A total of 262 patients received atezolizumab and 270 received a placebo. HRQoL was assessed using the FKSI-19 instrument from baseline through 5 years of follow-up. The FKSI-19 total score ranges from 0–76, with higher scores indicating better quality of life. A ≥5-point decline has traditionally been considered a clinically meaningful deterioration in RCC trials.
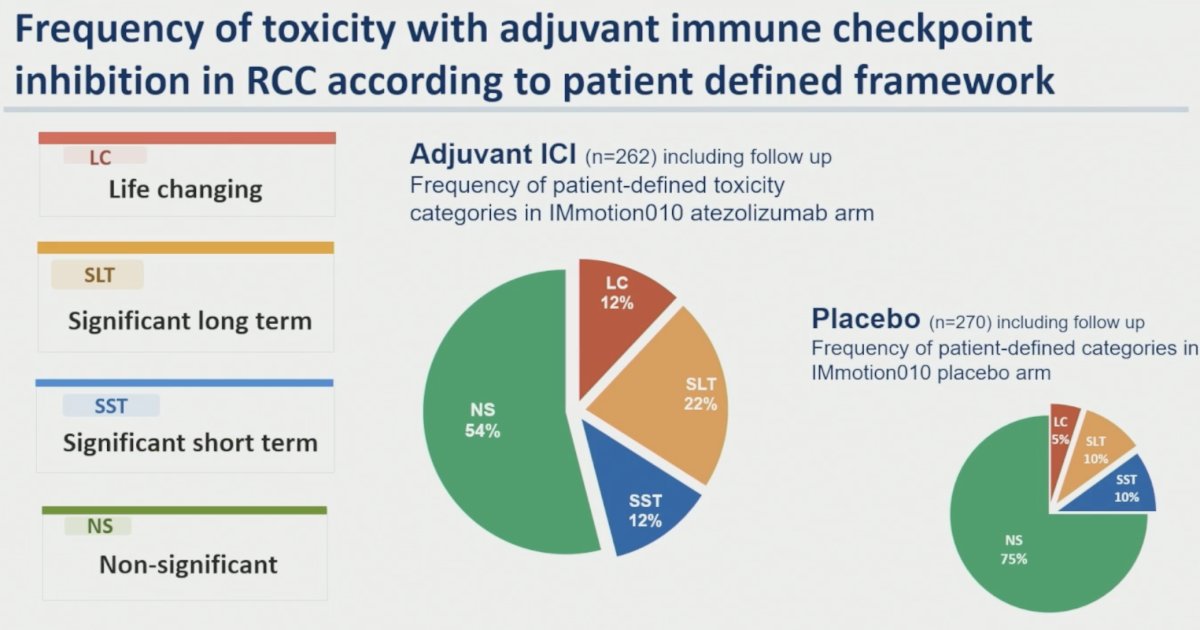
Application of the patient-defined toxicity framework demonstrated marked differences in toxicity burden between treatment groups. In the atezolizumab arm, toxicity categories were distributed as follows:
- Life-changing: 12%
- Significant long-term: 22%
- Significant short-term: 12%
- Non-significant: 54%
By comparison, placebo-treated patients experienced:
- Life-changing: 5%
- Significant long-term: 10%
- Significant short-term: 10%
- Non-significant: 75%
The investigators next compared conventional CTCAE grading with patient-informed toxicity classifications. Among patients who experienced grade 3–4 toxicities (n=68), only 31% were classified as life-changing, 29% as significant long-term, 27% as significant short-term, and 13% as non-significant. Importantly, many patients classified as having no toxicity or only grade 1–2 toxicity according to CTCAE criteria were reclassified into patient-defined categories associated with meaningful long-term impact. The authors concluded that “chronic immunotherapy-related toxicity may not be adequately captured by conventional CTCAE grading.”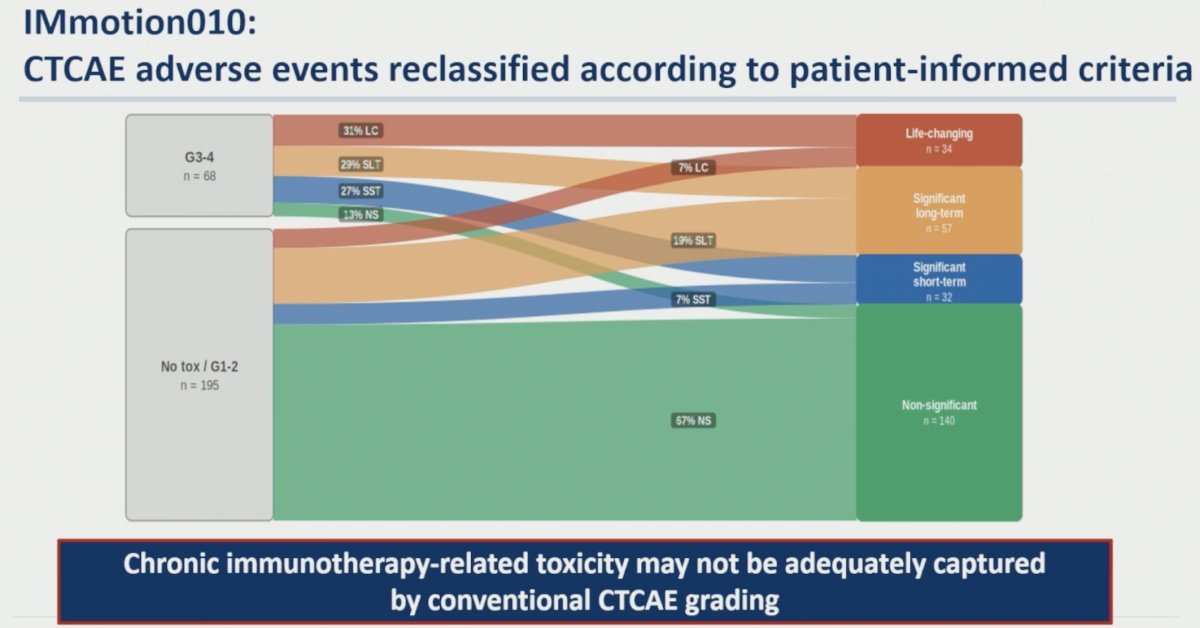
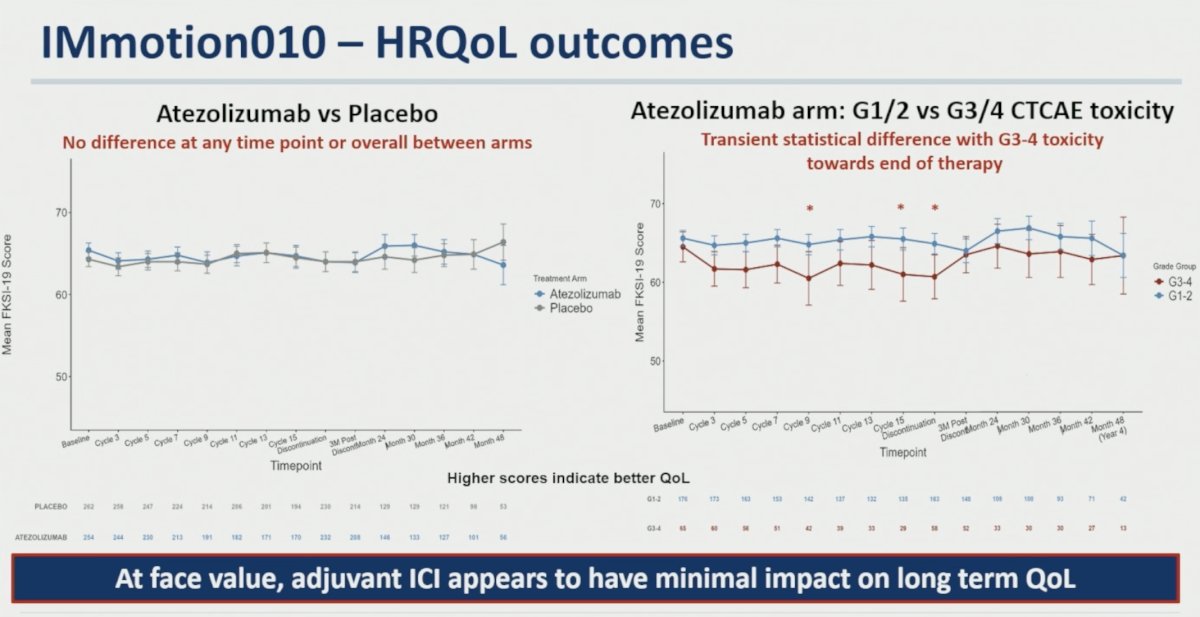
The first HRQoL analysis reproduced the reassuring findings commonly reported in adjuvant immunotherapy trials. Comparing atezolizumab versus placebo, no difference in FKSI-19 scores was observed at any time point or overall throughout follow-up. Similarly, within the atezolizumab arm, only transient statistical differences were observed between patients experiencing grade 1–2 versus grade 3–4 CTCAE toxicities near the end of treatment. As summarized on the slide, “At face value, adjuvant ICI appears to have minimal impact on long-term QoL.”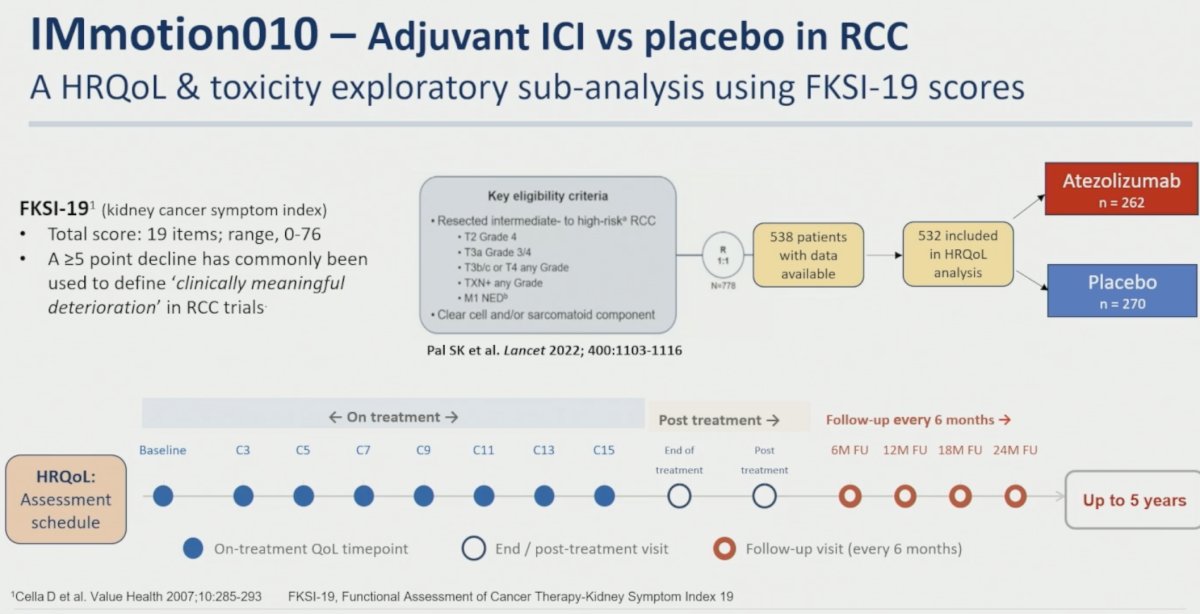
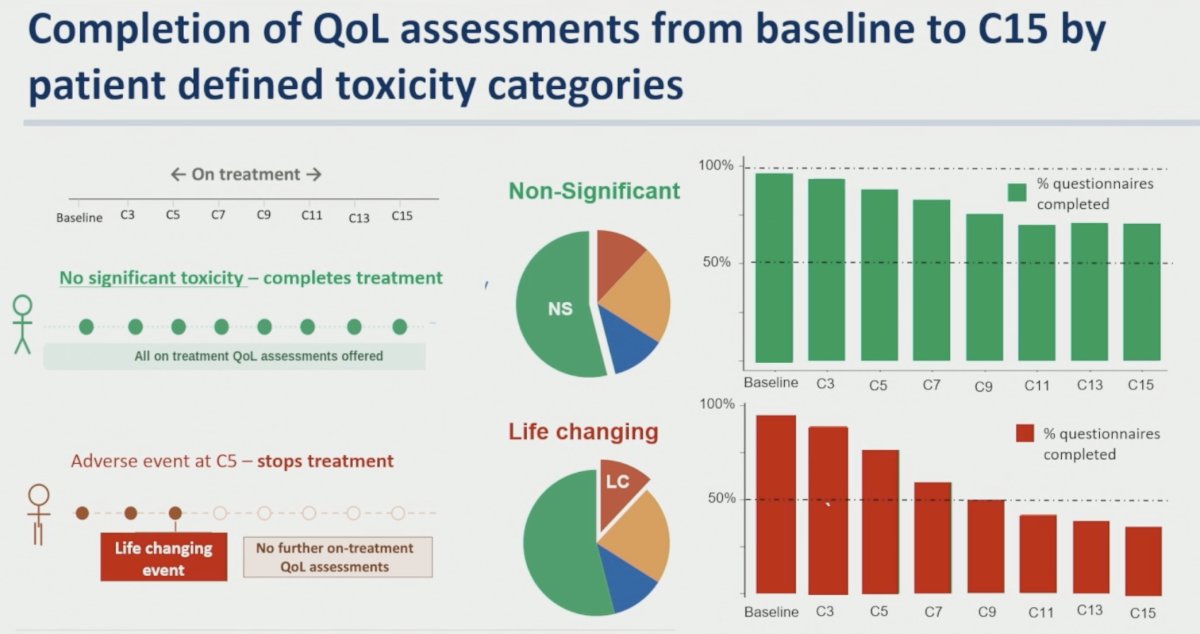
The investigators then examined questionnaire completion rates according to patient-defined toxicity categories. Patients without significant toxicity generally completed all on-treatment assessments. In contrast, patients experiencing life-changing toxicity frequently discontinued treatment early and subsequently stopped completing on-treatment QoL assessments. Completion rates among patients classified as non-significant remained relatively high throughout treatment (~70–95%), whereas completion rates among patients with life-changing toxicity progressively declined from approximately 90% at baseline to roughly 35% by cycle 15. Similar patterns persisted during long-term follow-up, suggesting substantial informative missingness.
When HRQoL was analyzed only during the treatment period (baseline to cycle 15), minimal differences were observed between toxicity categories. Mean FKSI-19 scores remained generally stable across life-changing, significant long-term, significant short-term, and non-significant groups, reinforcing the impression that conventional analyses may underestimate toxicity-related burden.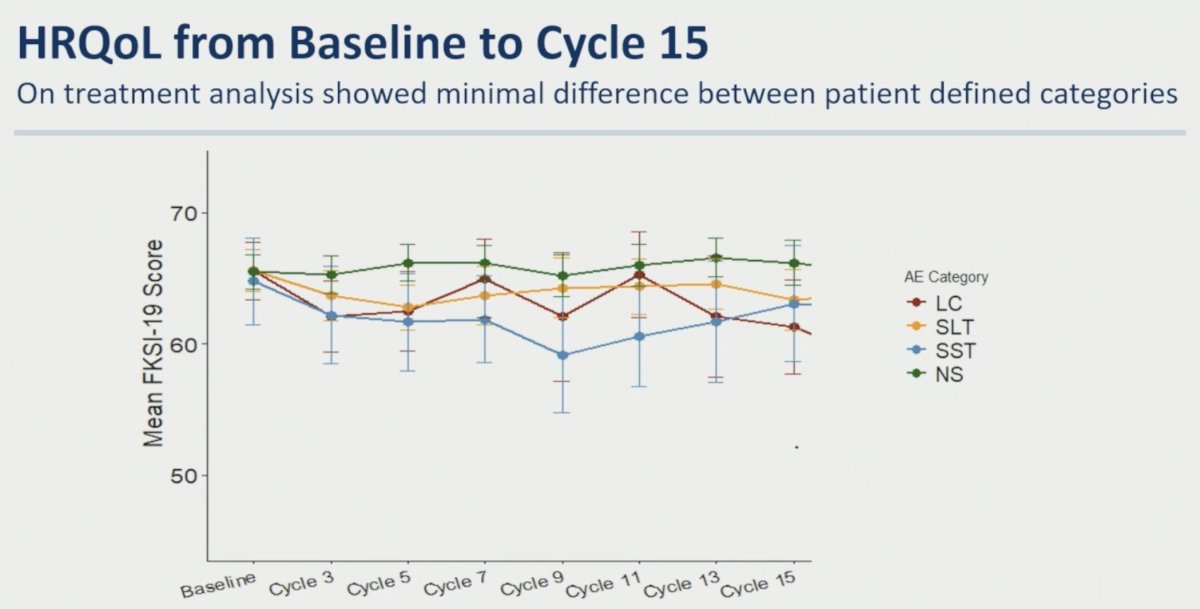
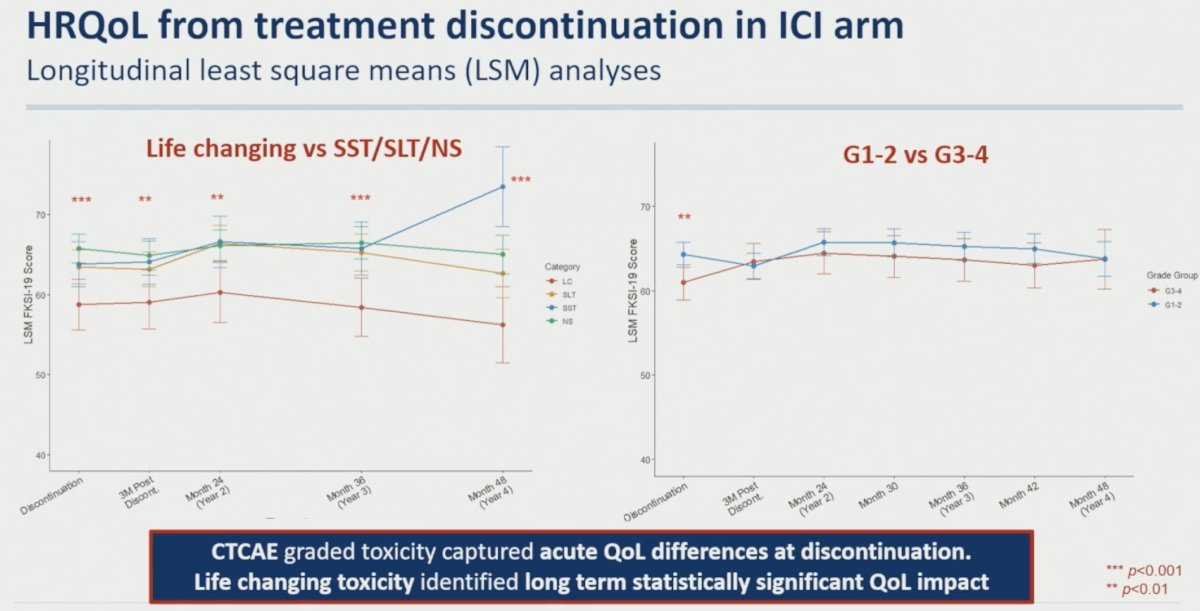
However, analyses anchored around treatment discontinuation revealed a markedly different picture. Longitudinal least squares mean analyses demonstrated that CTCAE grade captured acute QoL differences at treatment discontinuation, but these differences largely resolved over time. In contrast, patients experiencing life-changing toxicity demonstrated persistent and statistically significant long-term HRQoL impairment extending through 48 months after discontinuation.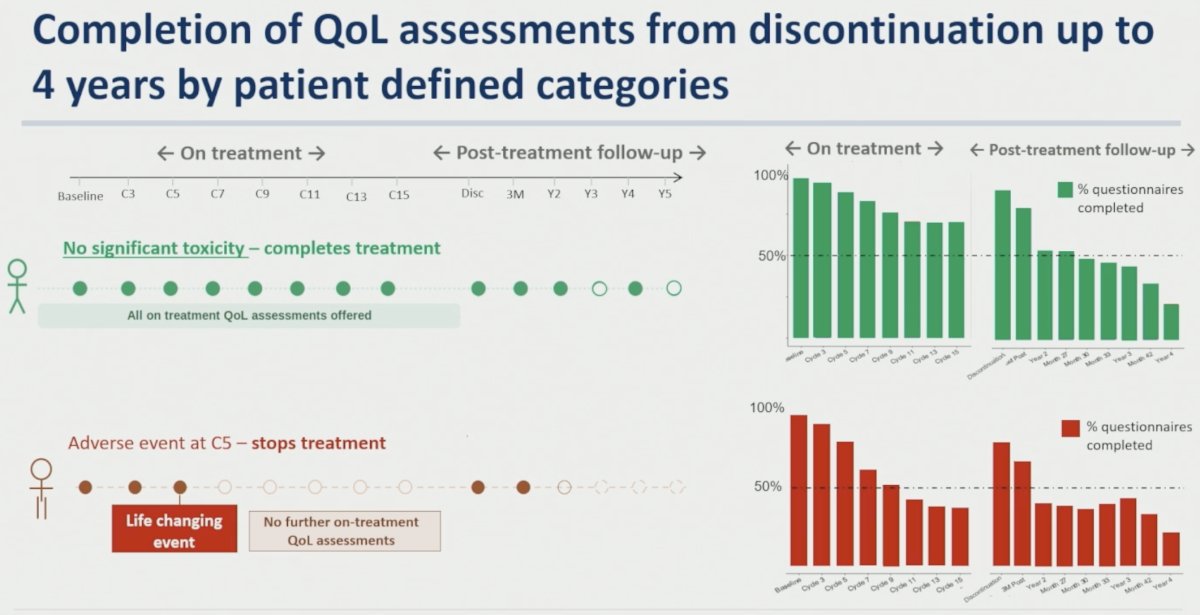
Significant differences between life-changing toxicity and SST/SLT/NS categories were observed at multiple post-discontinuation time points:
- Discontinuation: p<0.001
- Month 24 (Year 2): p<0.01
- Month 36 (Year 3): p<0.001
- Month 48 (Year 4): p<0.001
As highlighted by the investigators, “CTCAE graded toxicity captured acute QoL differences at discontinuation. Life-changing toxicity identified long-term statistically significant QoL impact.”
A sensitivity analysis excluding patients with disease recurrence demonstrated similar findings. Although disease progression can affect QoL in metastatic RCC, persistent QoL deterioration in this adjuvant population was not explained solely by recurrence events. Significant differences favoring non-life-changing toxicity groups persisted throughout follow-up, supporting the conclusion that long-term impairment was directly associated with toxicity burden rather than recurrence alone.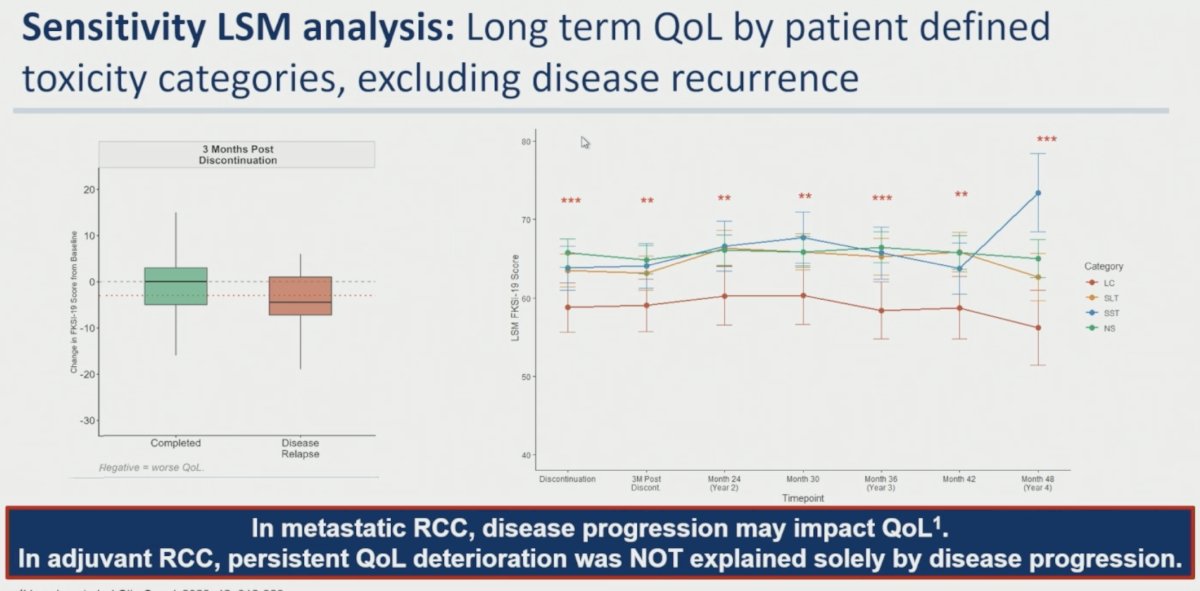
The investigators also examined HRQoL immediately before and after adverse event onset. Life-changing toxicities were associated with clinically meaningful deterioration in FKSI-19 scores, declining from 64.0 pre-event to 58.4 post-event, representing a change greater than the established 5-point threshold for clinically meaningful deterioration. Significant long-term toxicities demonstrated a smaller decline from 63.7 to 60.4 (approximately 3 points), while significant short-term toxicities showed essentially no change (63.7 to 63.9). Notably, CTCAE grade 3–4 toxicity showed only a modest decline from 63.6 to 61.7, underscoring the limited ability of CTCAE grading alone to identify persistent QoL impairment. The authors concluded: “Life-changing & Significant long-term toxicities were associated with persistent deterioration. CTCAE graded toxicity did not capture long-term QoL deterioration.”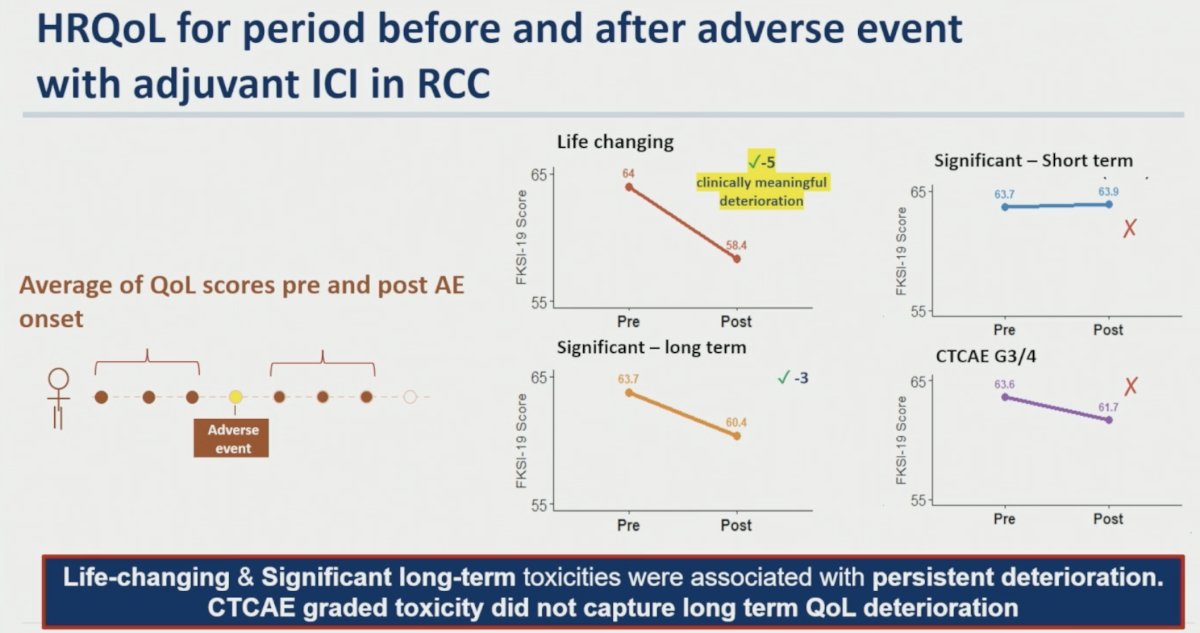
The decision regret analysis included 104 patients treated with adjuvant immunotherapy across three UK centers, more than 12 months after treatment completion. Decision regret was measured using the Ottawa Decision Regret Scale (DRS), a validated five-item patient-reported outcome instrument transformed to a 0–100 scale. Scores of 1–25 indicate mild regret, scores ≥25 indicate clinically significant regret, and scores ≥50 indicate high regret.
Overall, decision regret levels were low. The mean DRS score across the cohort was 13.8. Patients experiencing non-significant toxicity reported the lowest regret (mean 5.5), while patients with life-changing toxicity and significant toxicity demonstrated the highest scores:
- Life-changing toxicity: 27.0
- Significant toxicity: 26.0
- Non-significant toxicity: 5.5
Patients experiencing grade 3–4 CTCAE toxicity had a mean regret score of 17.9 compared with 12.7 among patients with grade 1–2 toxicity. Patients with recurrence had a mean score of 10.0 compared with 15.0 among those without recurrence.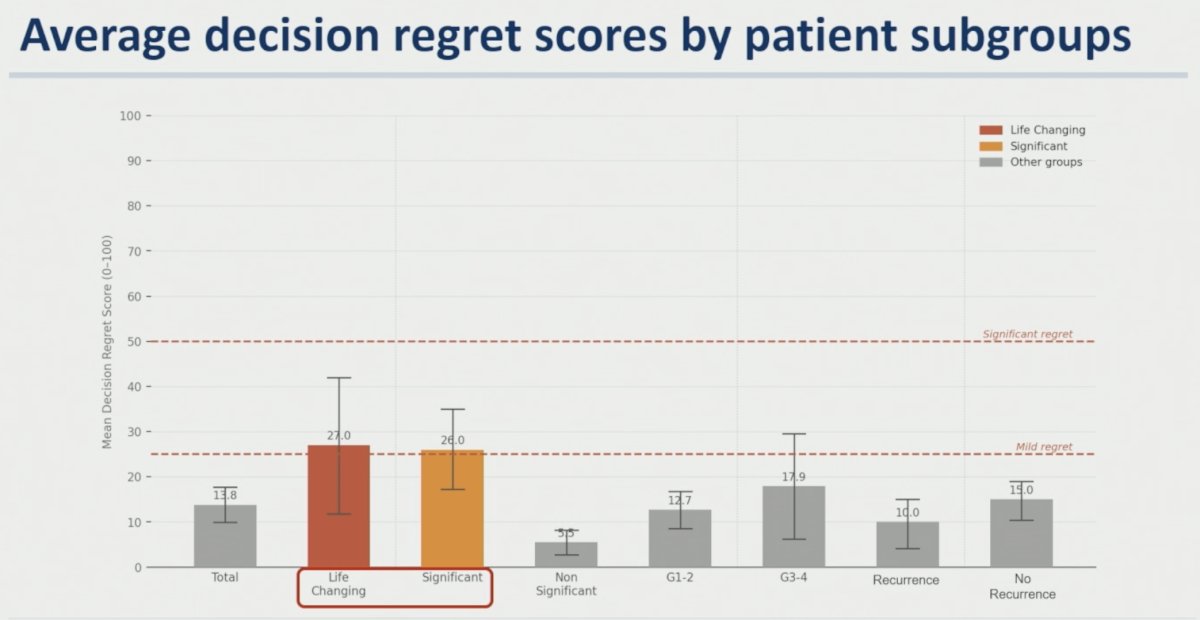
Importantly, pre-treatment expectations regarding toxicity influenced subsequent regret. Patients who retrospectively reported low expectations of toxicity experienced a mean regret score of 19.6, whereas those with high expectations of toxicity reported substantially lower regret scores (7.1). The authors emphasized that improved long-term toxicity and survivorship data are needed to better inform shared decision-making in the adjuvant setting.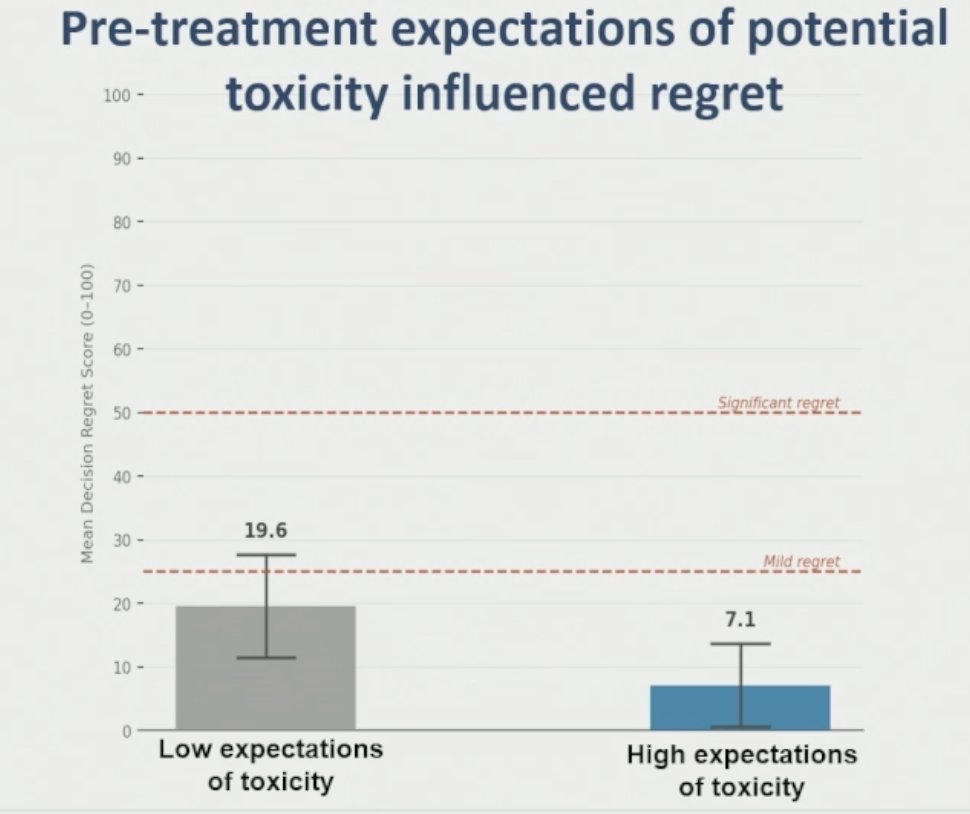
Dr. Nally concluded her presentation as follows:
- Long-term impact with adjuvant ICI may be underestimated by conventional HRQoL analyses due to reduced follow-up after toxicity or disease progression.
- Novel analyses centred around toxicity events and treatment discontinuation may better capture long-term patient experience.
- Life-changing toxicity occurs in approximately 10% of patients following treatment with adjuvant ICI in RCC.
- Life-changing toxicity demonstrated persistent long-term HRQoL impairment beyond conventional CTCAE grade alone.
- The majority of patients were satisfied with the decision they made to have adjuvant therapy.
- Patient that exhibited regret were more likely to have experienced long-term toxicity.
- Future perioperative ICI trials require more robust long-term toxicity and HRQoL follow-up alongside traditional efficacy endpoints.
Presented by: Elizabeth Nally, Clinical Research Fellow, Barts Cancer Institute, London, UK
Written by: Rashid K. Sayyid, MD, MSc, Assistant Professor, Urologic Oncologist, Department of Urology at The University of Arizona and Banner University Medical Center, Tucson, AZ – @rksayyid on X during the American Society of Clinical Oncology Genitourinary (ASCO) Annual Meeting held in Chicago, IL between May 29th and June 1st, 2026
References:- Choueiri TK, Tomczak P, Park SH, Venugopal B, Ferguson T, Chang YH, Hajek J, Symeonides SN, Lee JL, Sarwar N, Thiery-Vuillemin A, Gross-Goupil M, Mahave M, Haas NB, Sawrycki P, Gurney H, Chevreau C, Melichar B, Kopyltsov E, Alva A, Burke JM, Doshi G, Topart D, Oudard S, Hammers H, Kitamura H, Bedke J, Perini RF, Zhang P, Imai K, Willemann-Rogerio J, Quinn DI, Powles T; KEYNOTE-564 Investigators. Adjuvant Pembrolizumab after Nephrectomy in Renal-Cell Carcinoma. N Engl J Med. 2021 Aug 19;385(8):683-694. doi: 10.1056/NEJMoa2106391. PMID: 34407342.
- Choueiri TK, Tomczak P, Park SH, Venugopal B, Ferguson T, Symeonides SN, Hajek J, Chang YH, Lee JL, Sarwar N, Haas NB, Gurney H, Sawrycki P, Mahave M, Gross-Goupil M, Zhang T, Burke JM, Doshi G, Melichar B, Kopyltsov E, Alva A, Oudard S, Topart D, Hammers H, Kitamura H, McDermott DF, Silva A, Winquist E, Cornell J, Elfiky A, Burgents JE, Perini RF, Powles T; KEYNOTE-564 Investigators. Overall Survival with Adjuvant Pembrolizumab in Renal-Cell Carcinoma. N Engl J Med. 2024 Apr 18;390(15):1359-1371. doi: 10.1056/NEJMoa2312695. PMID: 38631003.