(UroToday.com) The 2026 American Society of Clinical Oncology (ASCO) Annual Meeting was host to a session on new approaches to curing bladder and kidney cancer. Dr. James Larkin presented results from the phase III RAMPART trial evaluating adjuvant durvalumab monotherapy and durvalumab plus tremelimumab versus active monitoring following resection of primary renal cell carcinoma (RCC).
RAMPART represents one of the largest adjuvant immunotherapy studies conducted in RCC and was designed to determine whether immune checkpoint blockade could reduce recurrence risk following nephrectomy in patients with intermediate- and high-risk disease.
Adjuvant therapy in RCC remains an area of active investigation. While pembrolizumab demonstrated a disease-free survival (DFS) and overall survival (OS) benefit in KEYNOTE-564,1,2 uncertainty remains regarding the optimal immunotherapeutic approach, the patient populations most likely to benefit, and whether combination checkpoint blockade may improve outcomes further. RAMPART was therefore developed as an international, investigator-led randomized phase III trial assessing adjuvant durvalumab alone and durvalumab plus tremelimumab following complete resection of RCC.
RAMPART was originally planned to enroll 1,750 patients; however, the study design was modified following the COVID-19 pandemic and publication of KEYNOTE-564. The modified design was blinded to accumulating outcome data and retained disease-free survival (DFS) as the primary endpoint. A pre-specified and pre-powered analysis was also planned according to baseline relapse risk.
Eligible patients had confirmed RCC and were considered at high or intermediate risk of relapse according to Leibovich risk criteria, including patients with fully resected synchronous ipsilateral adrenal metastases or a single fully resected soft tissue metastasis. A total of 790 patients were randomized in a 3:2:2 ratio to:
- Durvalumab 1,500 mg plus tremelimumab 75 mg administered at day 1 and week 4, followed by durvalumab for one year (n=225)
- Durvalumab monotherapy 1,500 mg for one year (n=225)
- Active monitoring (n=340)
All analyses were conducted in the intention-to-treat population.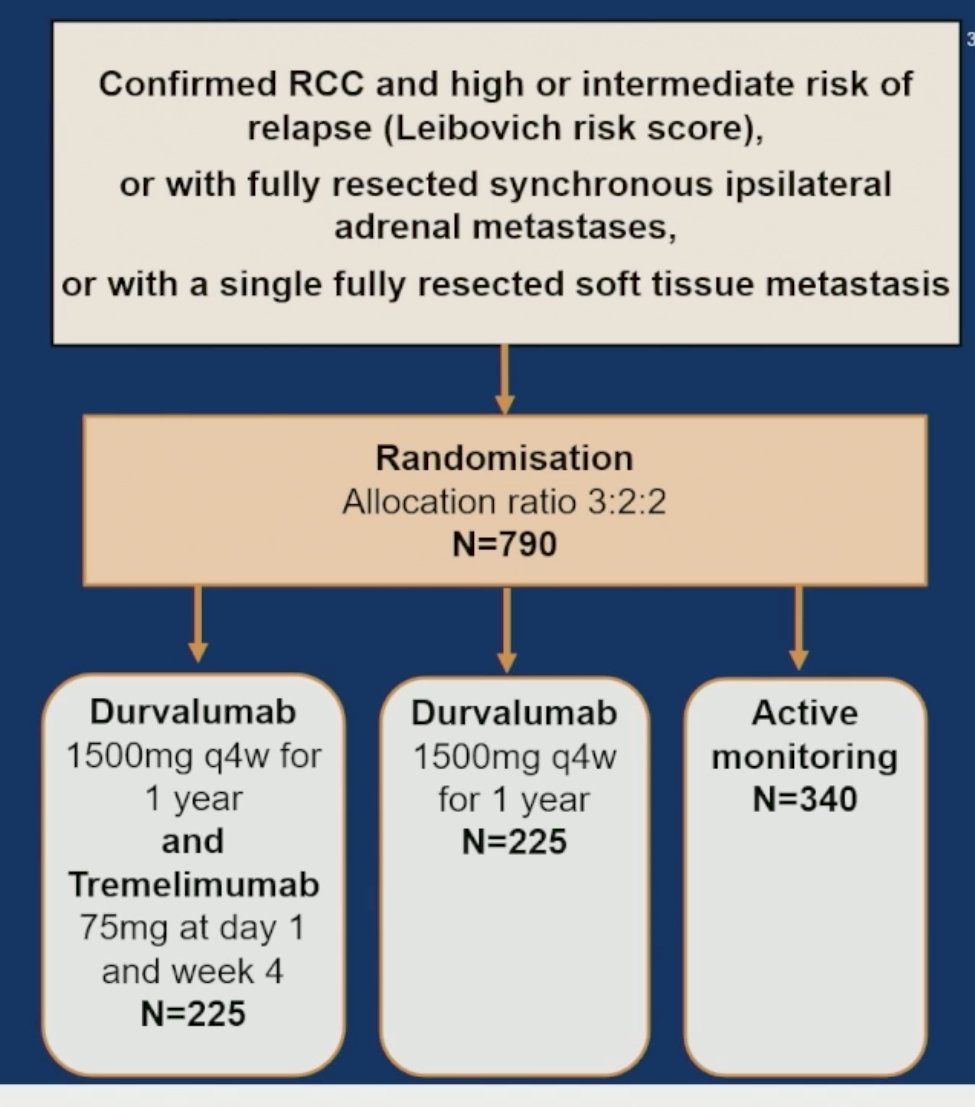
Risk stratification was based on the Leibovich score, which incorporates pathological T category, nodal status, tumor size, nuclear grade, and histologic tumor necrosis. Intermediate-risk disease was defined by intermediate Leibovich scores, whereas higher-risk disease included patients with high Leibovich scores and M1 NED disease.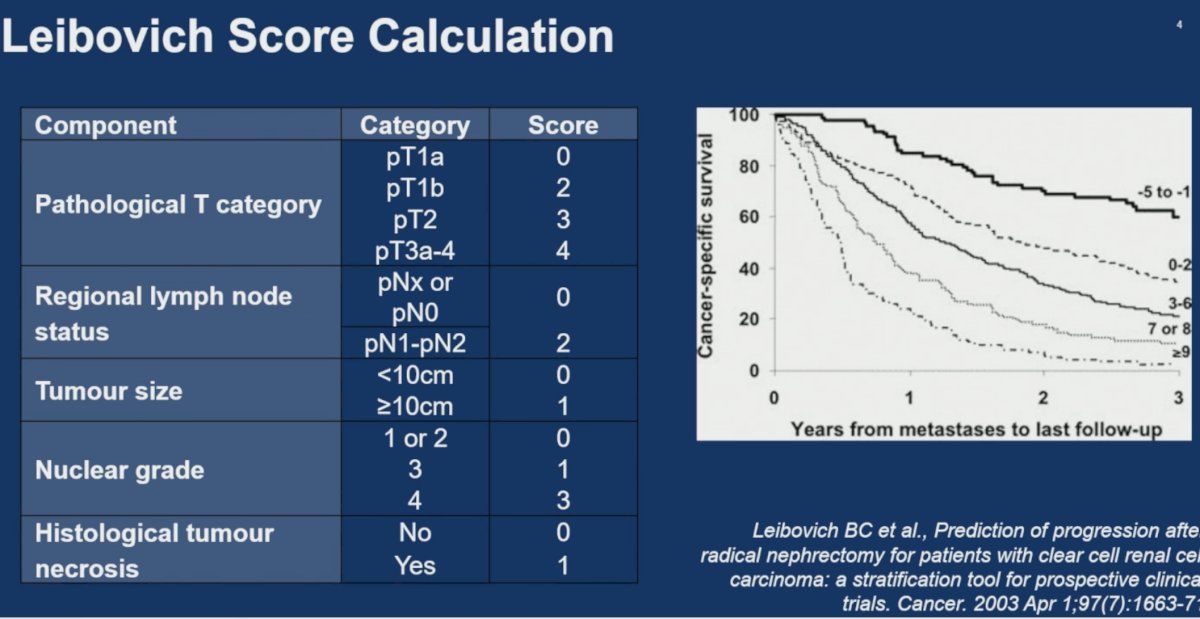
Among the 790 randomized patients, 225 were assigned to durvalumab plus tremelimumab, 225 to durvalumab monotherapy, and 340 to active monitoring. A total of 207 patients in the combination arm and 215 patients in the durvalumab arm received allocated treatment. In the primary analysis population, DFS events occurred in 43 patients in the durvalumab plus tremelimumab arm, 53 patients in the durvalumab arm, and 94 and 102 patients, respectively, in the active-monitoring comparator analyses.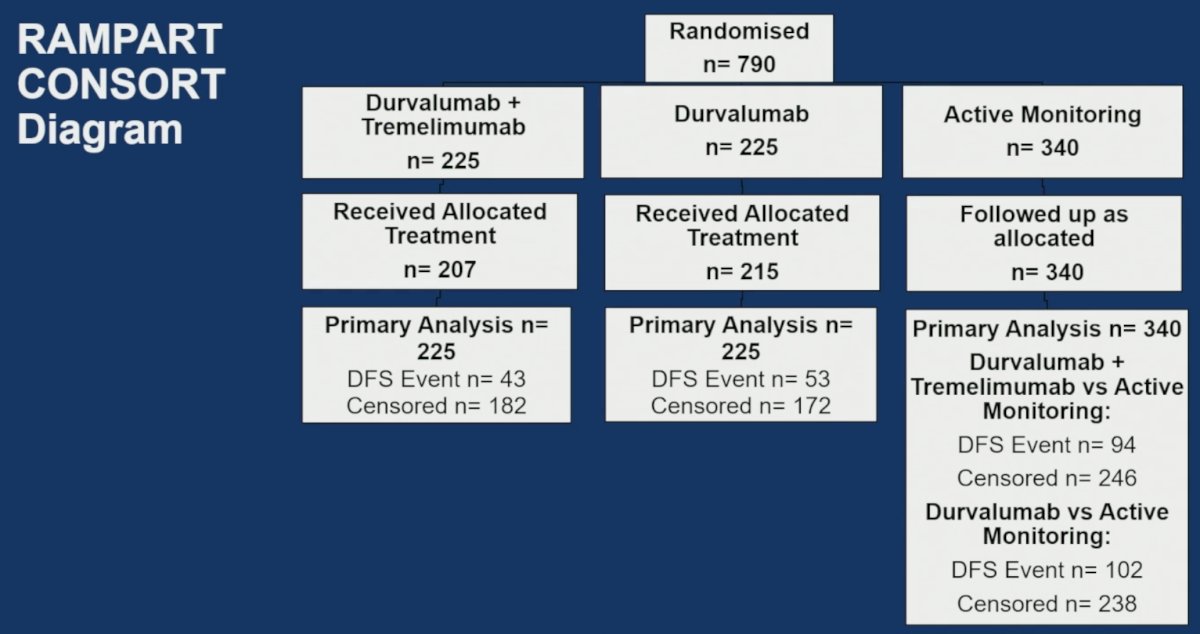
Baseline characteristics were well balanced across treatment groups. Mean age was 59–60 years. Male patients comprised 71–73% of the study cohort. 84–86% of patients had clear-cell histology. Intermediate-risk Leibovich disease was present in 44–46% of patients, while high-risk Leibovich disease accounted for 49–51%. M1 NED disease represented 4–5% of enrolled patients. Most patients had pT3 disease (72–75%)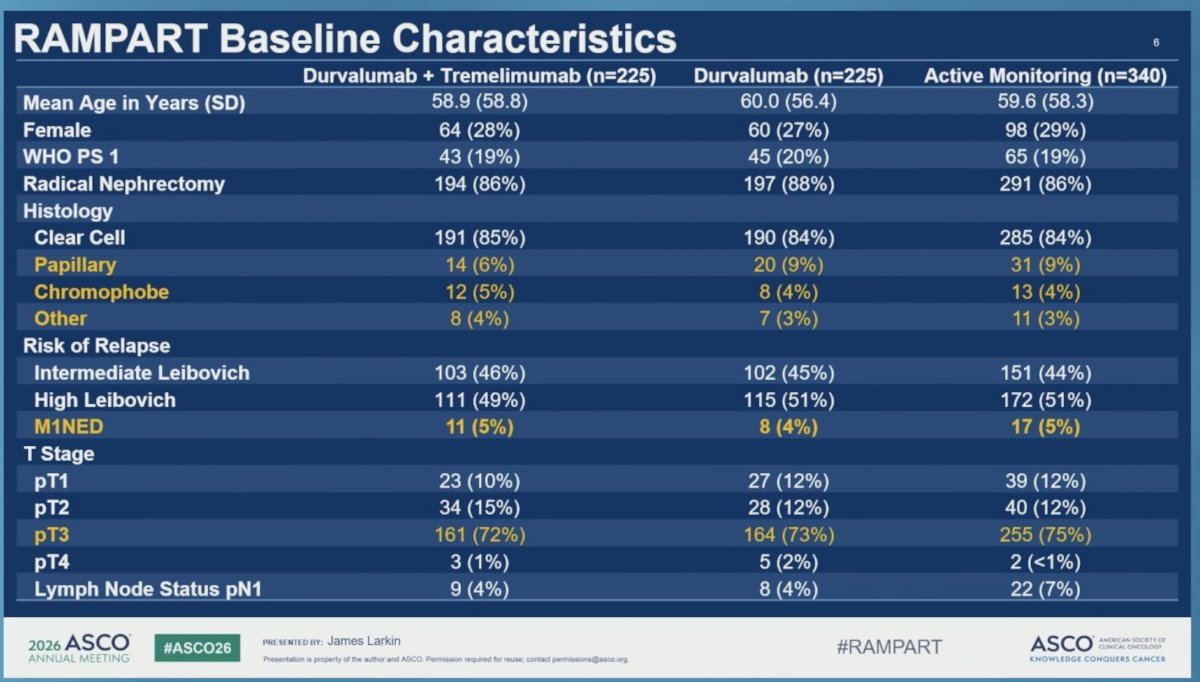
The statistical considerations were as follows: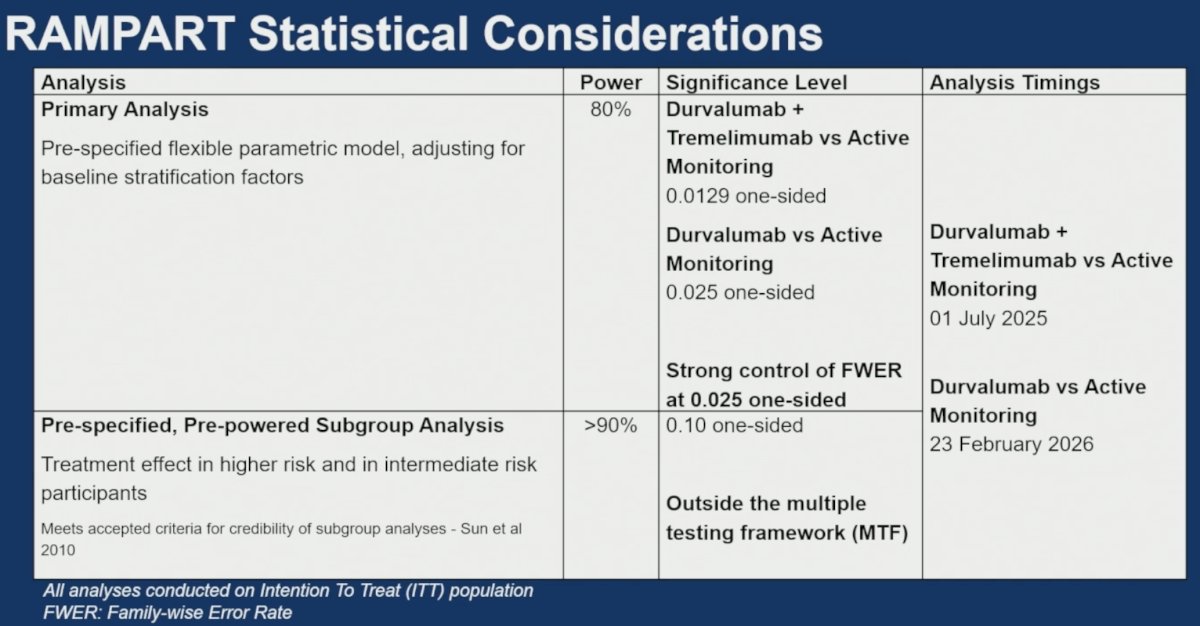
The primary DFS analysis was conducted with a median follow-up of 3.5 years. Three-year DFS rates were:
- 80% for durvalumab plus tremelimumab
- 78% for durvalumab
- 72% for active monitoring
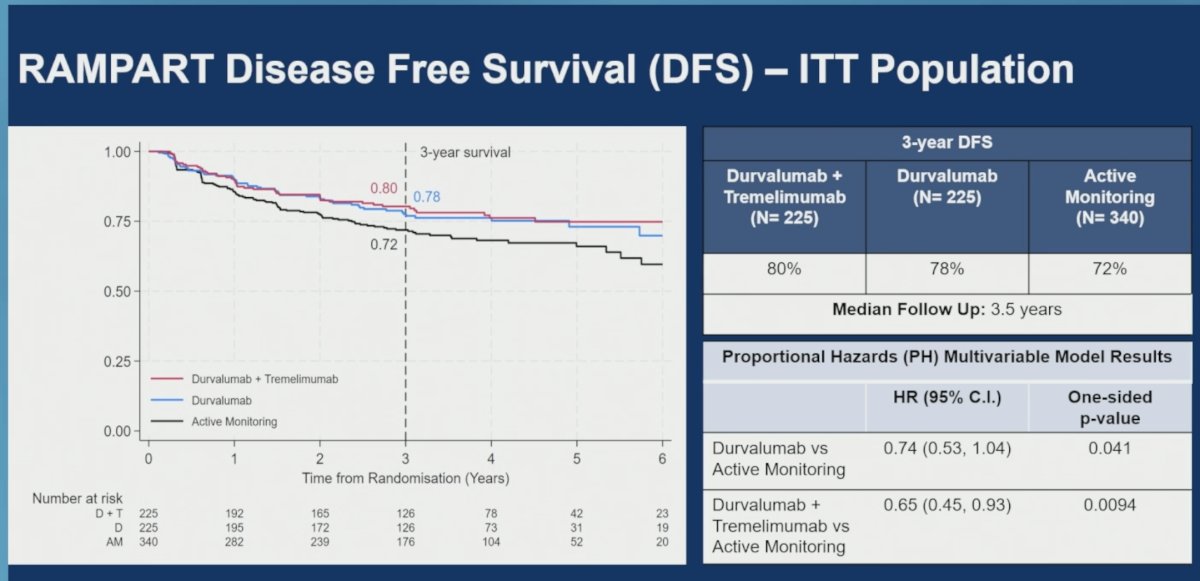
For durvalumab monotherapy versus active monitoring, the multivariable proportional hazards model yielded a hazard ratio of 0.74 (95% CI: 0.53–1.04; one-sided p=0.041). Although numerically favorable, this did not meet the pre-specified statistical threshold required for significance.
For durvalumab plus tremelimumab versus active monitoring, DFS was significantly improved, with a hazard ratio of 0.65 (95% CI: 0.45–0.93; one-sided p=0.0094). The Kaplan-Meier curves showed persistent divergence throughout follow-up, supporting a durable DFS benefit for the combination regimen.
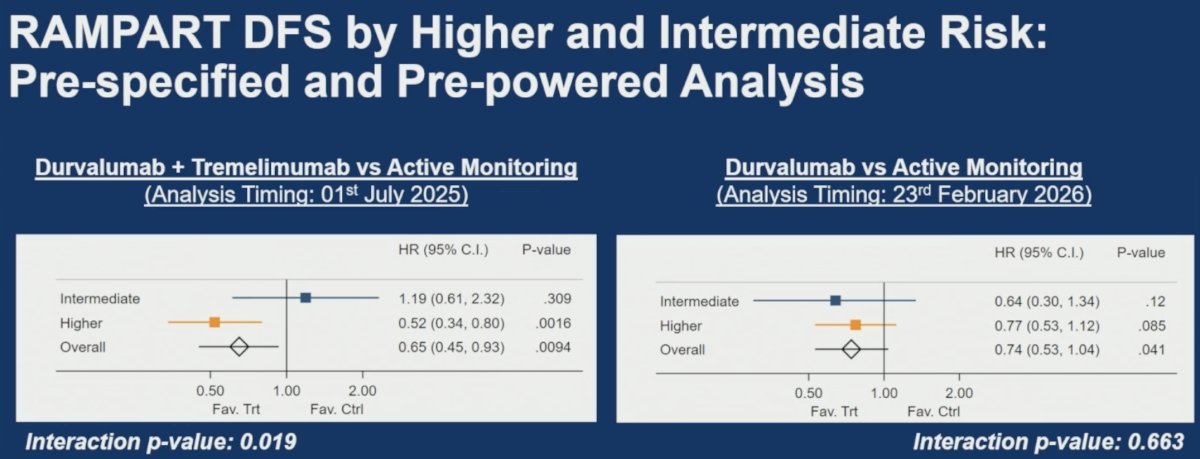
A pre-specified, pre-powered subgroup analysis evaluated treatment effects according to baseline relapse risk. For durvalumab plus tremelimumab versus active monitoring:
- Intermediate-risk subgroup: HR 1.19 (95% CI: 0.61–2.32)
- Higher-risk subgroup: HR 0.52 (95% CI: 0.34–0.80)
- Overall: HR 0.65 (95% CI: 0.45–0.93)
- Interaction p-value = 0.019
- These findings demonstrated that the DFS benefit of combination therapy was concentrated in patients at higher risk of recurrence.
For durvalumab versus active monitoring:
- Intermediate-risk subgroup: HR 0.64 (95% CI: 0.30–1.34)
- Higher-risk subgroup: HR 0.77 (95% CI: 0.53–1.12)
- Overall: HR 0.74 (95% CI: 0.53–1.04)
- Interaction p-value = 0.663
- No evidence of differential treatment effect according to baseline risk was observed with durvalumab monotherapy.
Among patients with higher-risk disease, including high Leibovich and M1 NED patients, the Kaplan-Meier curves demonstrated the greatest benefit for combination therapy. Three-year DFS rates were 76% for durvalumab plus tremelimumab, 66% for durvalumab, and 61% for active monitoring. In this subgroup, the hazard ratio for durvalumab plus tremelimumab versus active monitoring was 0.52 (95% CI: 0.34–0.80; p=0.0016), whereas the hazard ratio for durvalumab monotherapy versus active monitoring was 0.77 (95% CI: 0.53–1.12; p=0.085).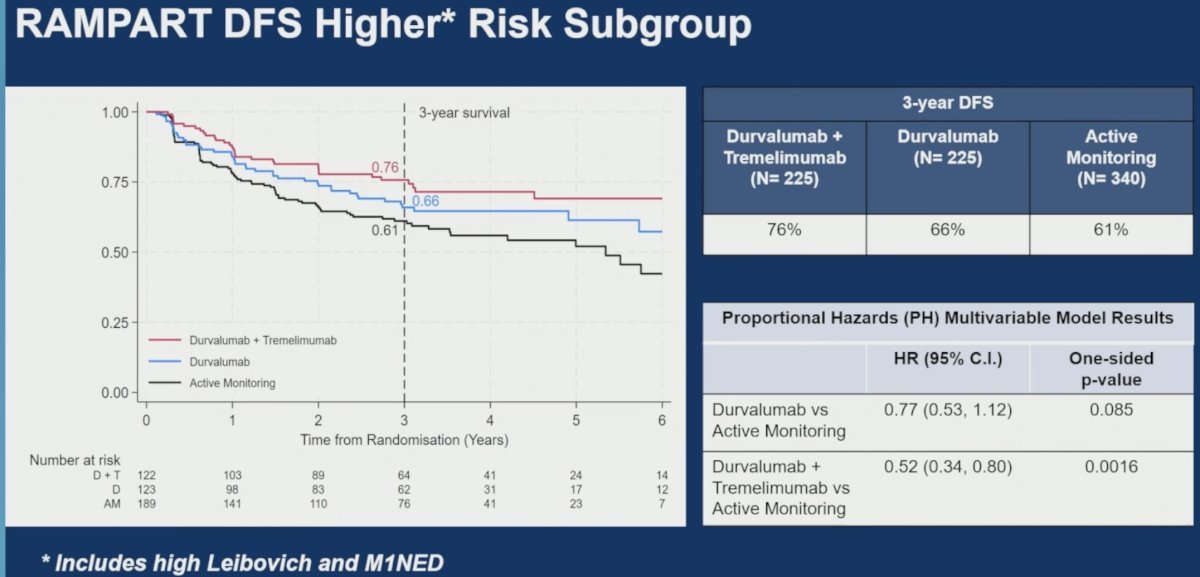
In contrast, among patients with intermediate Leibovich-risk disease, three-year DFS rates were 86%, 92%, and 85% for durvalumab plus tremelimumab, durvalumab, and active monitoring, respectively. Hazard ratios were 1.19 (95% CI: 0.61–2.32; p=0.309) for durvalumab plus tremelimumab and 0.64 (95% CI: 0.30–1.34; p=0.12) for durvalumab versus active monitoring, indicating no apparent DFS benefit in this lower-risk population.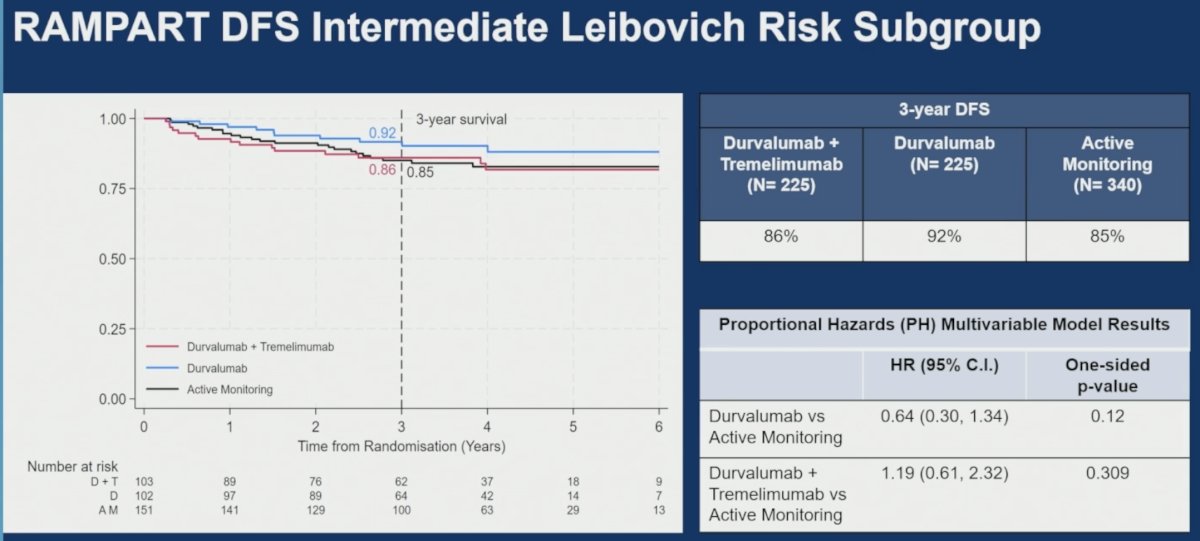
Exploratory subgroup analyses evaluating age, sex, M1 NED status, nephrectomy type, histology, and cytoreductive nephrectomy generally demonstrated consistency with the overall treatment effects. Forest plots showed no major heterogeneity across clinical subgroups, although confidence intervals widened substantially in smaller patient subsets.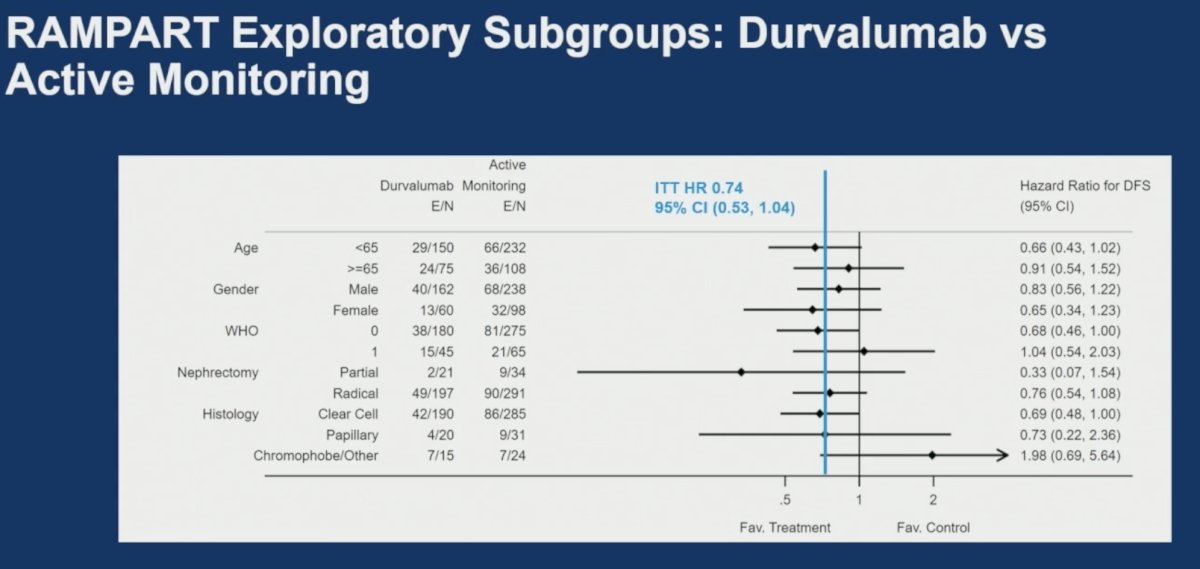
Overall survival data remain immature. Three-year OS rates were 96% for durvalumab plus tremelimumab, 98% for durvalumab, and 96% for active monitoring. For durvalumab versus active monitoring, the hazard ratio was 0.99 (95% CI: 0.52–1.92; one-sided p=0.492). For durvalumab plus tremelimumab versus active monitoring, the hazard ratio was 0.71 (95% CI: 0.34–1.46; one-sided p=0.176). The Kaplan-Meier OS curves remained largely overlapping at the current follow-up duration.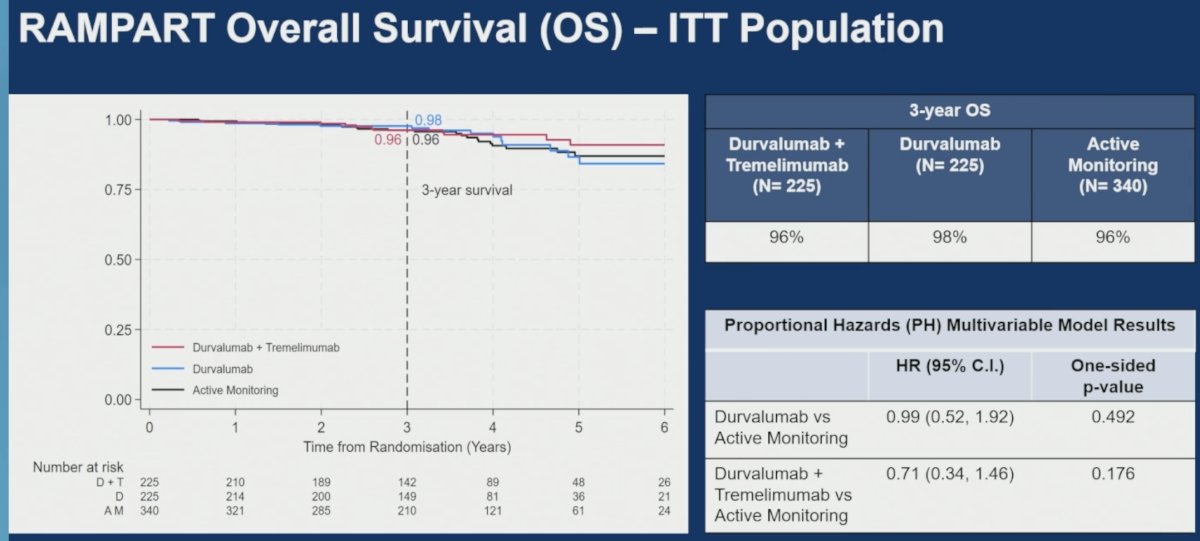
Treatment exposure was substantial in both active-treatment groups. Median treatment duration was 10.9 months (range 0–13.3) for durvalumab plus tremelimumab and 11 months (range 0–15.2) for durvalumab. Patients received a median of eight durvalumab infusions and two tremelimumab infusions in the combination arm and 11 durvalumab infusions in the monotherapy arm. Protocol-defined treatment completion occurred in 23% and 24% of patients for durvalumab and tremelimumab, respectively, in the combination arm and in 32% of patients receiving durvalumab monotherapy.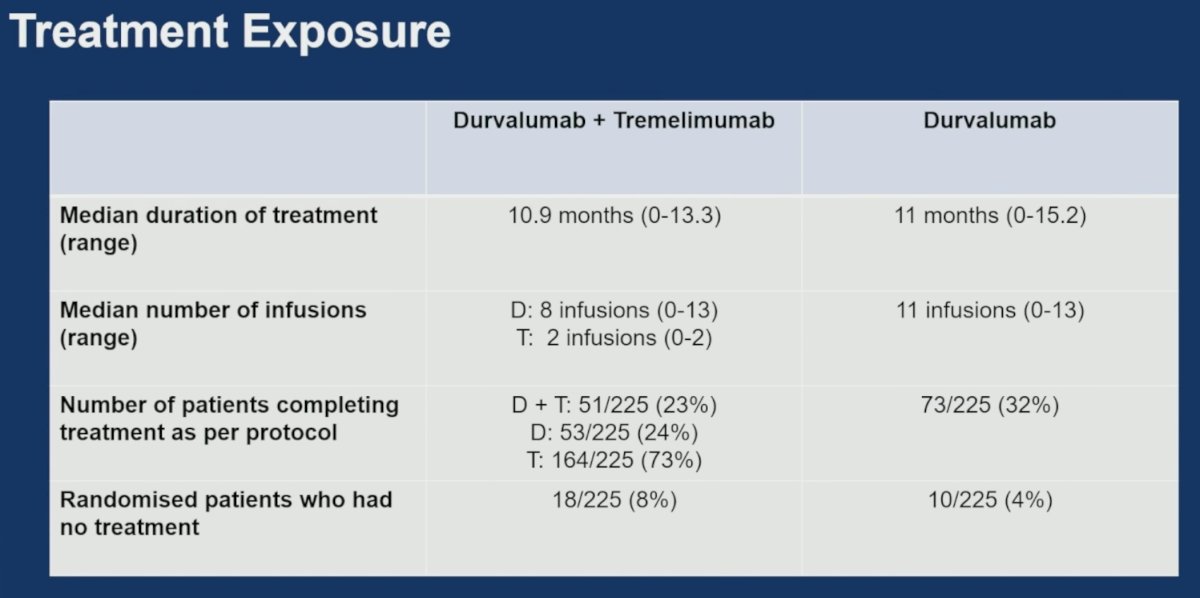
The safety profile was consistent with the known profiles of these agents. The most common all-cause adverse events included fatigue/asthenia, diarrhea/colitis, rash, pruritus, renal impairment, arthralgia, nausea, constipation, abdominal pain, and myalgia/joint stiffness. Higher-grade adverse events were most frequently diarrhea/colitis, myalgia/joint stiffness, transaminitis, hypertension, renal impairment, dyspnea, hypothyroidism, pruritus, adrenal insufficiency, and pulmonary embolism.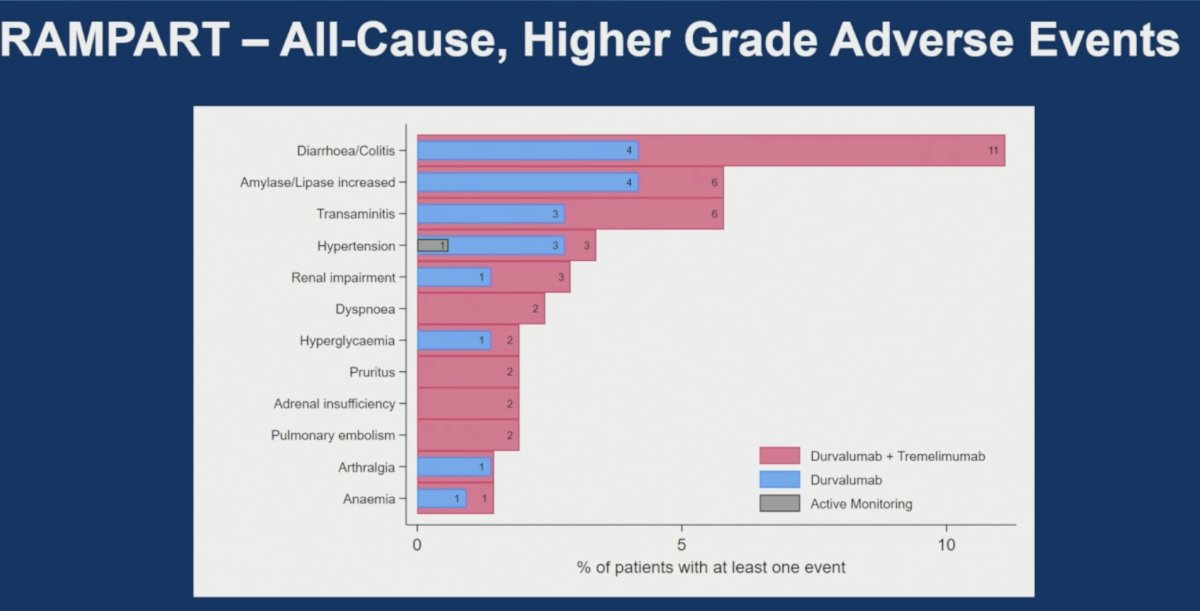
The detailed safety summary demonstrated:
- Any-grade adverse events:
- Durvalumab plus tremelimumab: 201 patients (87%)
- Durvalumab: 199 patients (88%)
- Active monitoring: 219 patients (64%)
- Grade 3–5 adverse events:
- Durvalumab plus tremelimumab: 84 patients (37%)
- Durvalumab: 65 patients (29%)
- Active monitoring: 31 patients (9%)
- Systemic corticosteroid use occurred in approximately 50% of patients receiving combination therapy and 30% receiving durvalumab.
Treatment-related deaths occurred in two patients receiving durvalumab plus tremelimumab and three patients receiving durvalumab. Notably, rare but important immune-mediated fatalities were observed, including fatal myasthenia gravis with durvalumab plus tremelimumab and fatal myocarditis with durvalumab.
Adverse events leading to treatment discontinuation occurred in 66 patients (29%) receiving durvalumab plus tremelimumab and 41 patients (18%) receiving durvalumab. Discontinuation specifically due to durvalumab occurred in 58 patients (26%) in the combination arm and 41 patients (18%) in the monotherapy arm, while tremelimumab-related discontinuation occurred in 30 patients (13%).
Quality-of-life analyses evaluated change in overall health and quality of life (OHQL) from baseline to month 15. No statistically significant or clinically meaningful differences were observed between treatment groups. For durvalumab plus tremelimumab versus active monitoring, the mean difference was 1.0 (95% CI: -4.6 to 6.5; p=0.732). For durvalumab versus active monitoring, the mean difference was -2.4 (95% CI: -7.7 to 2.9; p=0.372). Both results were well below the clinically meaningful difference threshold of 24 points.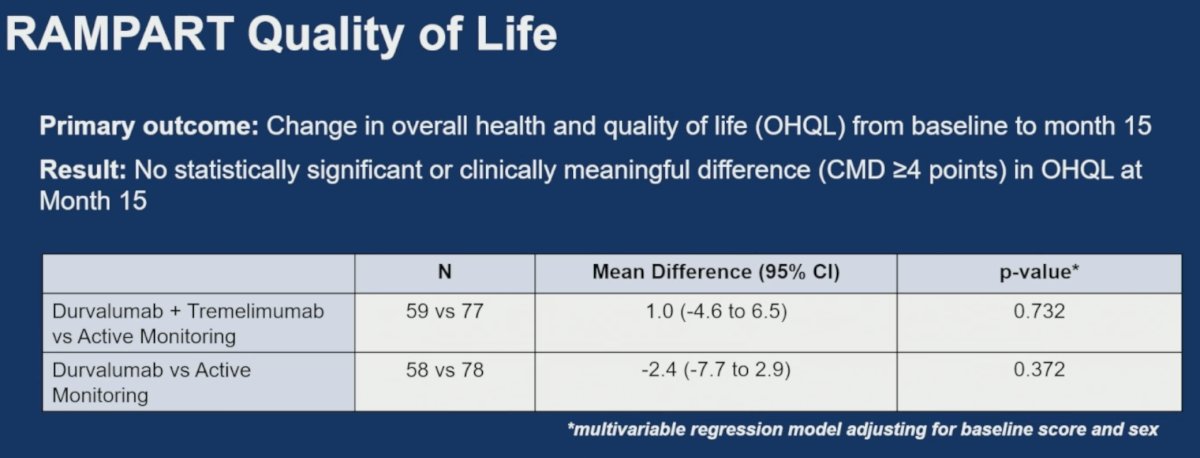
Dr. Larkin concluded his presentation of the RAMPART trial as follows:
- Durvalumab monotherapy following resection of renal cell carcinoma (RCC) showed no statistically significant improvement in Disease Free Survival (DFS) compared with active monitoring.
- Durvalumab plus tremelimumab significantly improved DFS compared with active monitoring.
- Safety findings were consistent with the known profiles of these agents, but rare immune-mediated adverse events, including fatal myocarditis and myasthenia gravis, were observed.
- No evidence of a difference in overall health and quality of life (OHQL) was observed at month 15 with either durvalumab monotherapy or durvalumab plus tremelimumab.
Presented by: James M. Larkin, Professor, The Royal Marsden Hospital, London, UK
Written by: Rashid K. Sayyid, MD, MSc, Assistant Professor, Urologic Oncologist, Department of Urology at The University of Arizona and Banner University Medical Center, Tucson, AZ – @rksayyid on X during the American Society of Clinical Oncology Genitourinary (ASCO) Annual Meeting held in Chicago, IL between May 29th and June 1st, 2026
References:
- Choueiri TK, Tomczak P, Park SH, Venugopal B, Ferguson T, Chang YH, Hajek J, Symeonides SN, Lee JL, Sarwar N, Thiery-Vuillemin A, Gross-Goupil M, Mahave M, Haas NB, Sawrycki P, Gurney H, Chevreau C, Melichar B, Kopyltsov E, Alva A, Burke JM, Doshi G, Topart D, Oudard S, Hammers H, Kitamura H, Bedke J, Perini RF, Zhang P, Imai K, Willemann-Rogerio J, Quinn DI, Powles T; KEYNOTE-564 Investigators. Adjuvant Pembrolizumab after Nephrectomy in Renal-Cell Carcinoma. N Engl J Med. 2021 Aug 19;385(8):683-694. doi: 10.1056/NEJMoa2106391. PMID: 34407342.
- Choueiri TK, Tomczak P, Park SH, Venugopal B, Ferguson T, Symeonides SN, Hajek J, Chang YH, Lee JL, Sarwar N, Haas NB, Gurney H, Sawrycki P, Mahave M, Gross-Goupil M, Zhang T, Burke JM, Doshi G, Melichar B, Kopyltsov E, Alva A, Oudard S, Topart D, Hammers H, Kitamura H, McDermott DF, Silva A, Winquist E, Cornell J, Elfiky A, Burgents JE, Perini RF, Powles T; KEYNOTE-564 Investigators. Overall Survival with Adjuvant Pembrolizumab in Renal-Cell Carcinoma. N Engl J Med. 2024 Apr 18;390(15):1359-1371. doi: 10.1056/NEJMoa2312695. PMID: 38631003.