(UroToday.com) The 2026 ASCO annual meeting featured an oral abstract kidney cancer session and a presentation by Dr. Toni Choueiri discussing a ctDNA analysis in participants with renal cell carcinoma (RCC) treated with adjuvant pembrolizumab in the KEYNOTE-564 trial. In the phase 3 KEYNOTE-564 trial, adjuvant pembrolizumab was superior to placebo in participants with clear cell RCC at increased risk of recurrence post nephrectomy:1,2 disease free survival HR 0.71, 95% CI 0.59-0.86; overall survival HR 0.66, 95% CI 0.48-0.90. ctDNA is a promising blood based biomarker for early disease detection and identification of patients at highest risk of recurrence in other tumor types, however data on the prevalence and utility of ctDNA in high risk resected RCC remain limited. At the 2026 ASCO annual meeting, Dr. Choueiri and colleagues reported an analysis of pretreatment and on-treatment ctDNA (using 2 versions of a ctDNA assay with different sensitivities) with clinical outcomes in KEYNOTE-564.
Participants with clear cell RCC at increased risk of recurrence post nephrectomy were randomized 1:1 to pembrolizumab or placebo. ctDNA was evaluated using Natera’s Signatera RUO tissue-exome-based 16-plex and 64-plex ctDNA assays. The primary objectives of this analysis were to evaluate the association of baseline ctDNA status and ctDNA status change from baseline to cycle 5 day 1 (C5D1) with disease free survival:
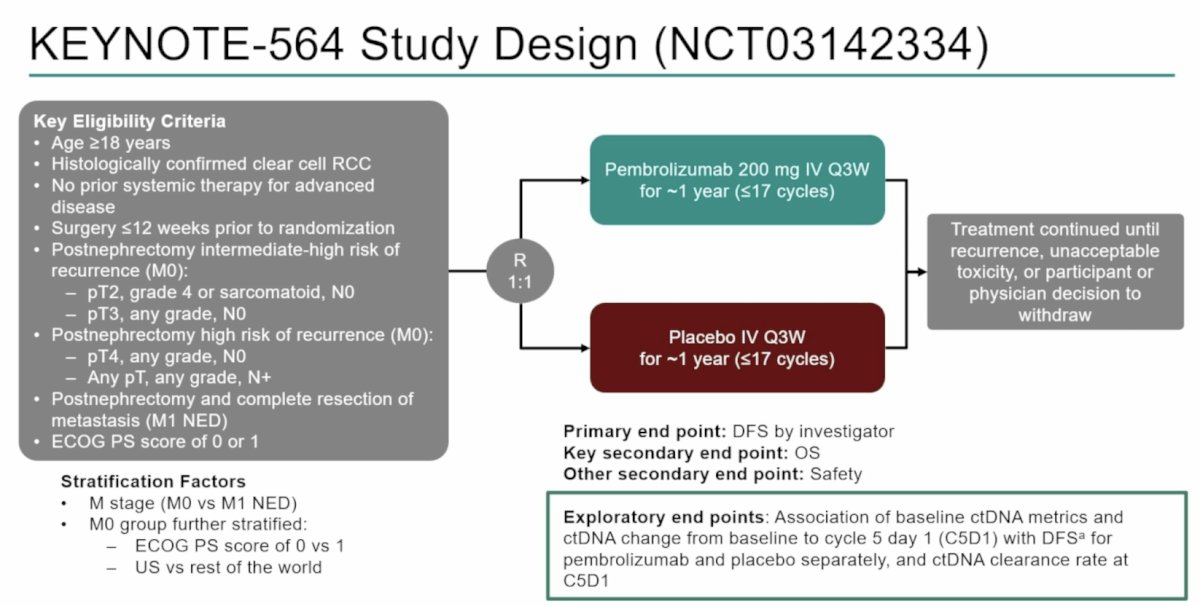
Significance was prespecified at multiplicity-adjusted α = 0.05. Sensitivity (percentage of ctDNA-positive participants among all participants with a disease free survival event) and specificity (percentage of ctDNA-negative participants among all participants without a disease free survival event) to predict disease free survival were also evaluated.
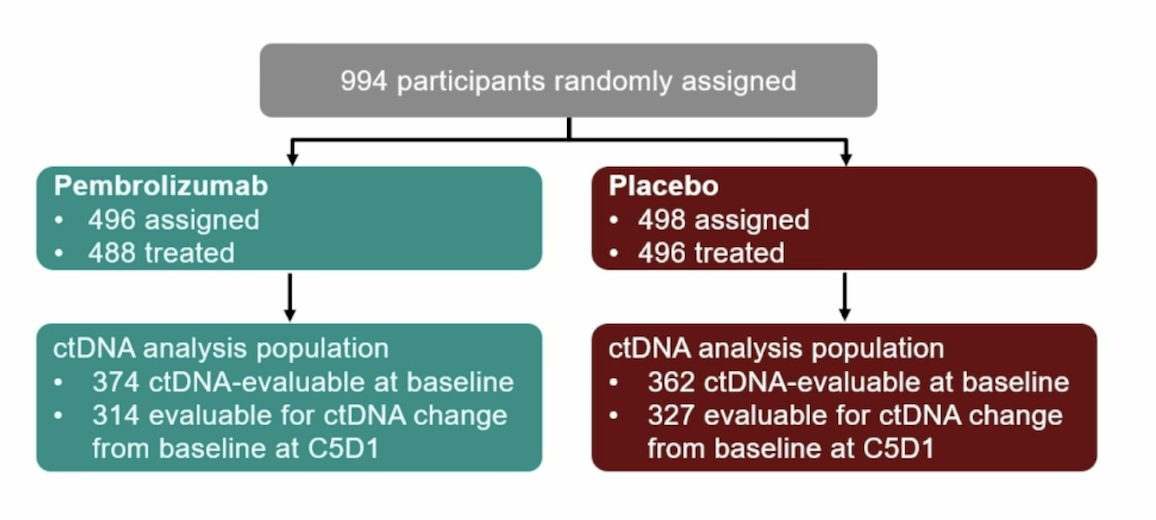
There were 994 participants randomized to pembrolizumab (n = 496) or placebo (n = 498). ctDNA samples from 736 participants (pembrolizumab n = 374; placebo n = 362) were analyzed at baseline and from 641 participants at C5D1 (pembrolizumab n = 314; placebo n = 327) using both assays:
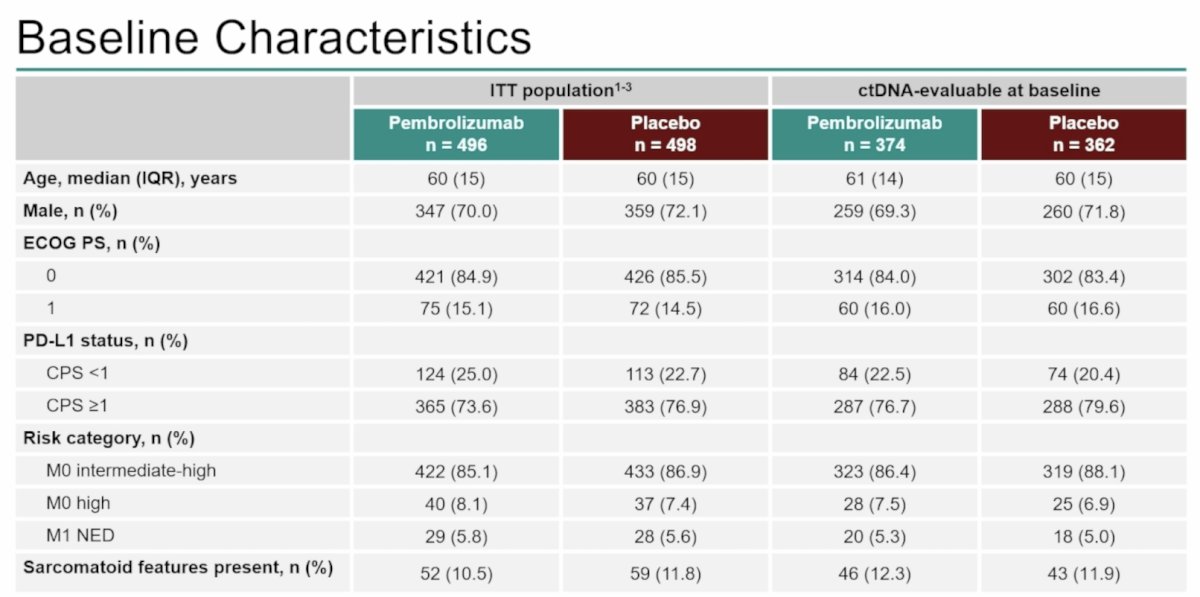
The baseline characteristics, as previously described, were well balanced between the two groups:
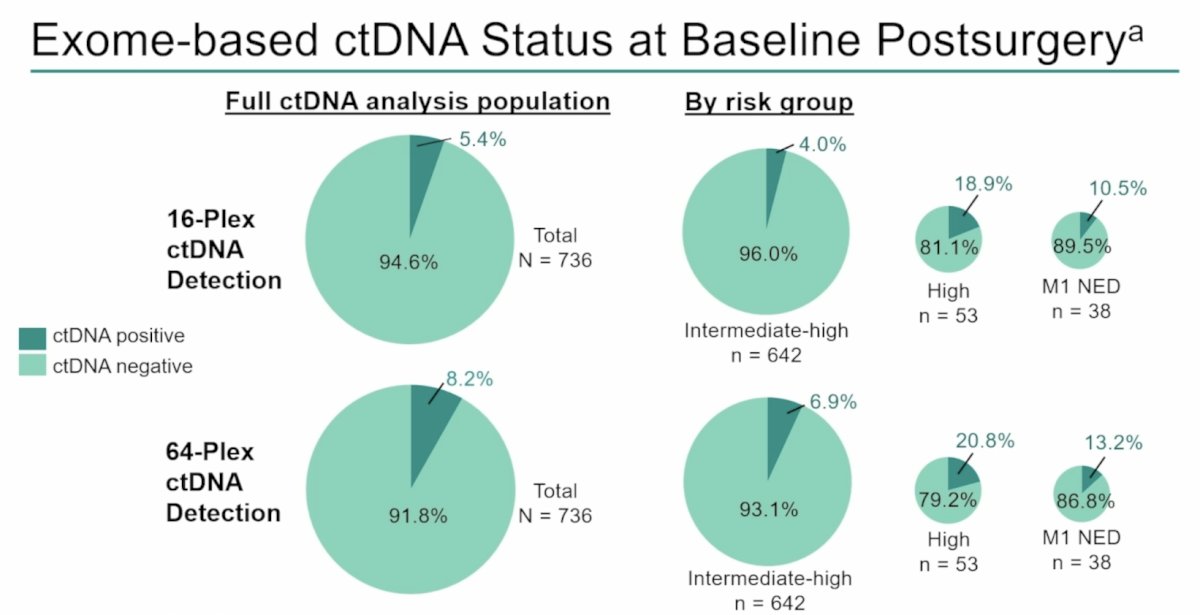
The median study follow-up was 69.5 months (range 60.2-86.9). In both treatment arms, ctDNA was detectable at baseline in 40 participants (5.4%) using the 16-plex assay and 60 participants (8.2%) using the 64-plex assay. By risk group, using the 16-plex assay, ctDNA was detectable at baseline in 26 of 642 (4.0%) intermediate-high risk participants, 10 of 53 (18.9%) high-risk participants, and 4 of 38 (10.5%) M1 NED participants. Using the 64-plex assay, ctDNA was detectable in 44 of 642 (6.9%) intermediate-high risk participants, 11 of 53 (20.8%) high-risk participants, and 5 of 38 (13.2%) M1 NED participants:
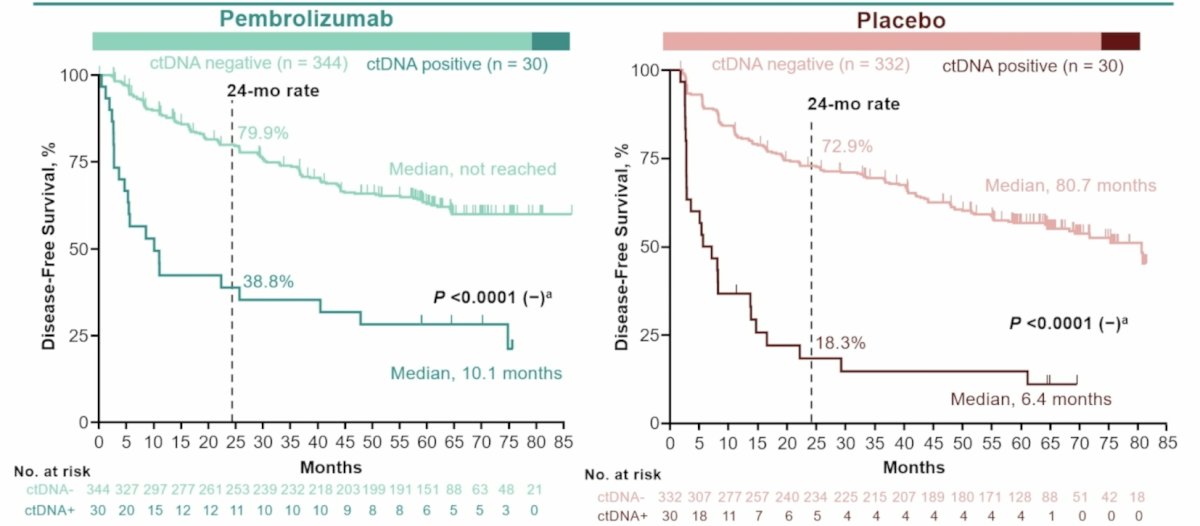
For both assays, ctDNA positivity was negatively associated with disease free survival in both pembrolizumab and placebo arms (both p-values < 0.0001):
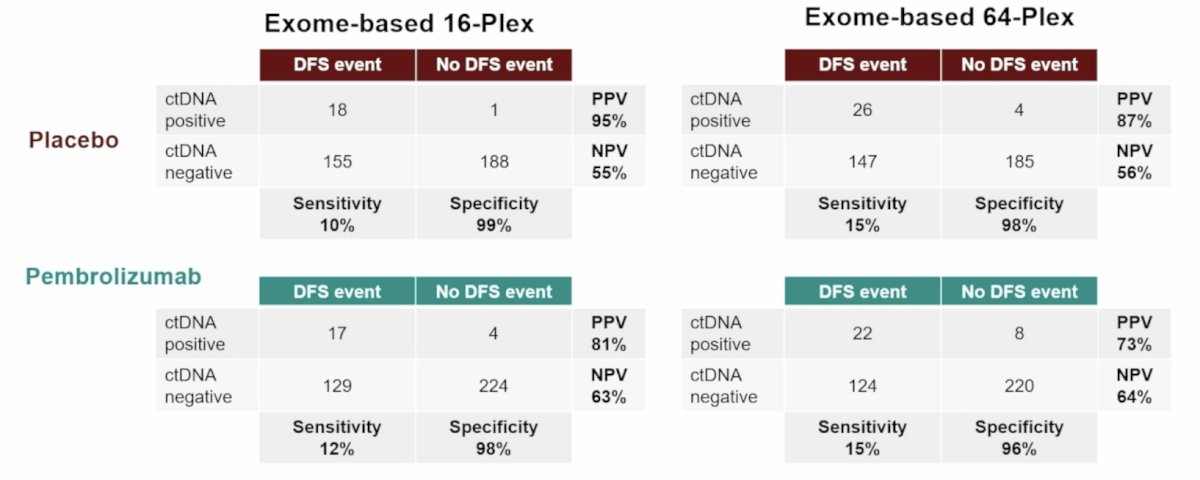
ctDNA status at baseline showed low sensitivity and high specificity to predict disease free survival in both treatment arms:
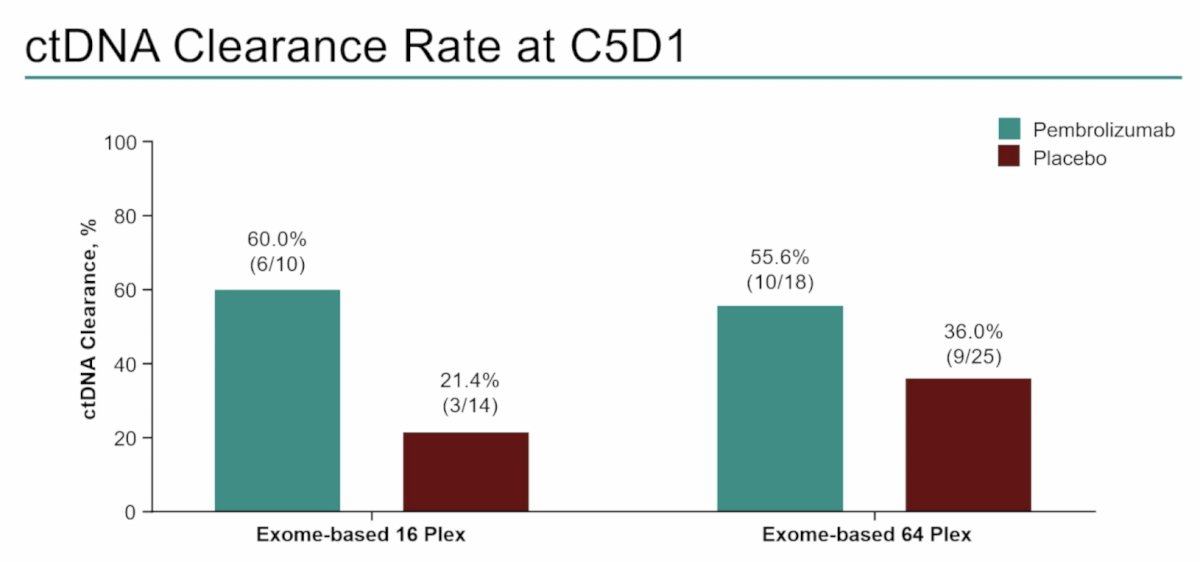
Of participants with detectable ctDNA at baseline and evaluable ctDNA at C5D1, ctDNA clearance at C5D1 occurred in 6 of 10 participants in the pembrolizumab arm and 3 of 14 participants in the placebo arm using the 16-plex assay, and 10 of 18 participants in the pembrolizumab arm and 9 of 25 participants in the placebo arm using the 64-plex assay:
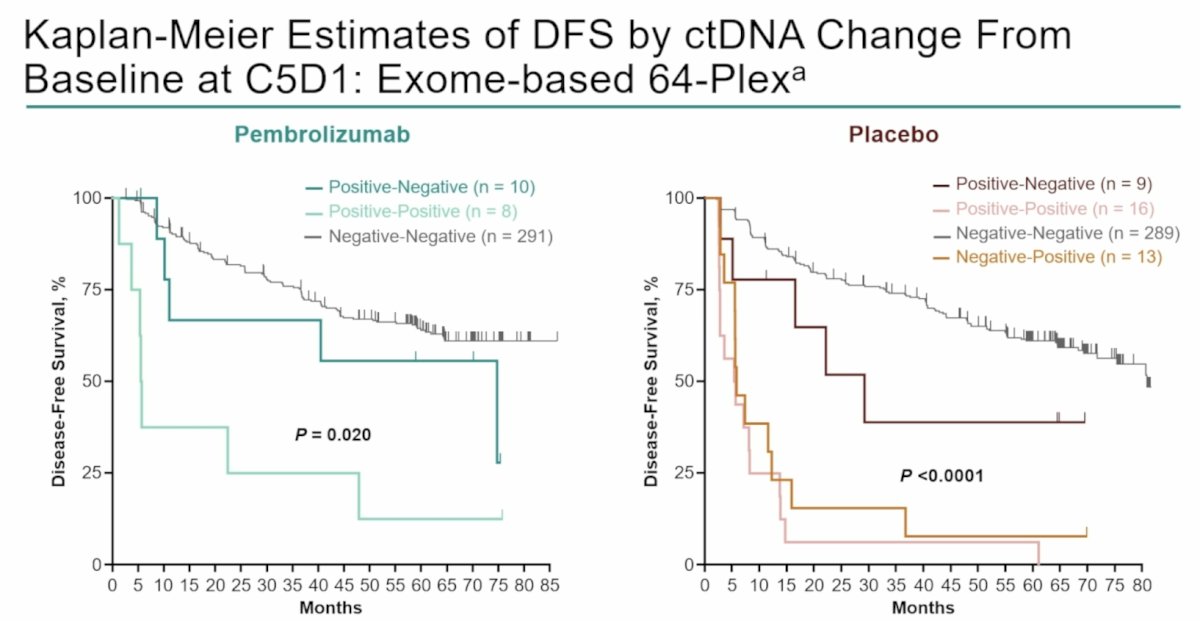
In both assays, ctDNA change from baseline at C5D1 was associated with disease free survival for both pembrolizumab (p = 0.020) and placebo arms (p < 0.0001):
Dr. Choueiri concluded his presentation discussing a ctDNA analysis in participants with RCC treated with adjuvant pembrolizumab in the KEYNOTE-564 trial with the following take home points:
- Following surgery in RCC, the ctDNA positivity rate and sensitivity of ctDNA exome-based testing at baseline were very low, although the specificity of ctDNA for recurrence was high
- ctDNA positivity at baseline was associated with worse disease free survival in both the pembrolizumab and placebo arms, irrespective of the number of variants (16 versus 64) utilized to test for ctDNA
- Pembrolizumab led to improved outcomes regardless of baseline ctDNA positivity
- The ctDNA clearance rate at C5D1 was higher in the pembrolizumab arm than in the placebo arm, which is consistent with the observed efficacy benefit of adjuvant pembrolizumab over placebo in the overall intention to treat population
- A higher ctDNA positivity rate resulted from 64-plex ctDNA testing as compared to 16-plex ctDNA testing
- These data highlight the limitations of low ctDNA positivity rate in high-risk resected clear cell RCC and do not support the routine use of current ctDNA technology (exome-based) to select patients at increased risk of recurrence post nephrectomy for adjuvant pembrolizumab therapy
Presented by: Toni K. Choueiri, MD, Dana Farber Cancer Center, Boston, MA
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Associate Professor of Urology, Georgia Cancer Center, Wellstar MCG Health, @zklaassen_md on Twitter during the American Society of Clinical Oncology Genitourinary (ASCO) Annual Meeting held in Chicago, IL between May 29th and June 1st, 2026
References:
- Choueiri TK, Tomczak P, Park SH, et al. Adjuvant Pembrolizumab after Nephrectomy in Renal-Cell Carcinoma. N Engl J Med. 2021 Aug 19;385(8):683-694.
- Choueiri TK, Tomczak P, Park SH, et al. Overall Survival with Adjuvant Pembrolizumab in Renal-Cell Carcinoma. N Engl J Med. 2024 Apr 18;390(15):1359-1371.