(UroToday.com) The 2026 ASCO annual meeting featured an oral abstract kidney cancer session and a presentation by Dr. Rana McKay discussing the RADICAL trial, a phase 2 randomized trial of radium-223 dichloride and cabozantinib in patients with renal cell carcinoma (RCC) with bone metastases. Bone metastases occur in ~30% of RCC patients and are associated with poor survival, quality of life, and symptomatic skeletal events. Radium-223, an alpha-emitting bone-seeking radioisotope, prolongs survival in advanced prostate cancer. Previously, a pilot study of radium-223 with VEGF tyrosine kinase inhibitors (TKI) in RCC with bone metastases showed safety and early efficacy:1
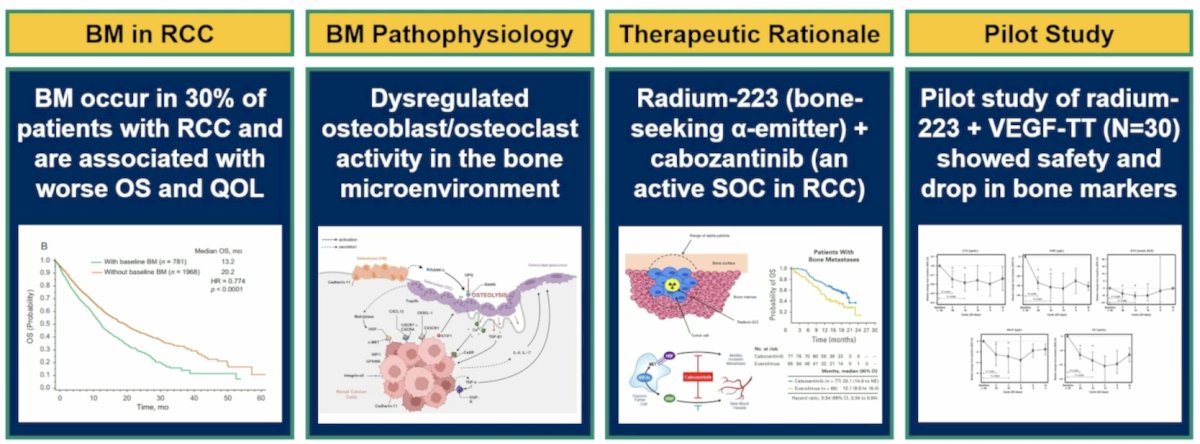
Additionally, cabozantinib is a TKI that has shown efficacy in patients with bone metastases. Thus, RADICAL (NCT04071223) was designed to investigate cabozantinib ± radium-223 in RCC with bone metastases, with the hypothesis that the combination therapy would improve symptomatic skeletal event free survival compared to cabozantinib alone.
This open label multicenter study enrolled RCC patients with ≥1 symptomatic bone metastasis not previously irradiated and Karnofsky performance status ≥60%. Prior therapies were allowed, and the non-clear cell population was limited to 20%. Randomization was 1:1 to cabozantinib with (Arm A) or without (Arm B) radium-223, stratified by osteoclast targeted therapy, prior therapy, baseline opioid use, and IMDC risk. In Arm A, cabozantinib was given as 40 mg daily cycle 1 and 60 mg thereafter, if tolerated. Radium-223 was 1.49 microcurie/kg IV every 28 days for 6 doses. In Arm B, cabozantinib was 60 mg daily. The primary endpoint was symptomatic skeletal event free survival, and secondary endpoints were safety, objective response rate, progression free survival, and overall survival:
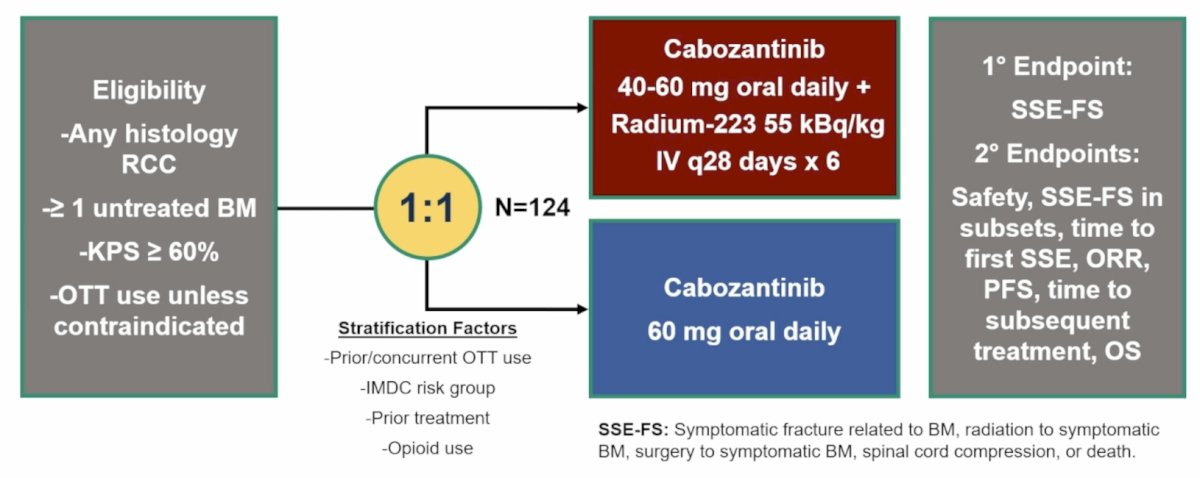
The study was designed with 85% power to detect improvement in 6-month symptomatic skeletal event free survival from 65% to 78% (one-sided α = 0.05. There was a single prespecified interim analysis (futility only), which was triggered when 50% of expected symptomatic skeletal event free survival events had been observed. The Wieand rule was employed, which was recommended to stop for futility if the hazard ratio was > 1.0. The database was locked on March 2, 2026.
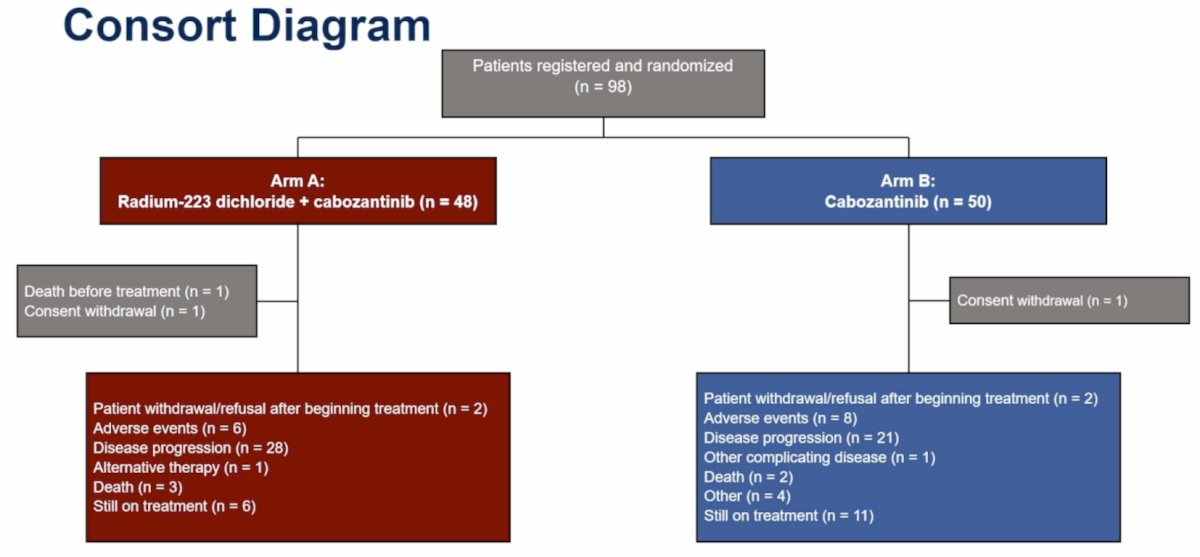
From December 2019 to September 2025, 98 patients were enrolled and evaluable for the interim analysis:
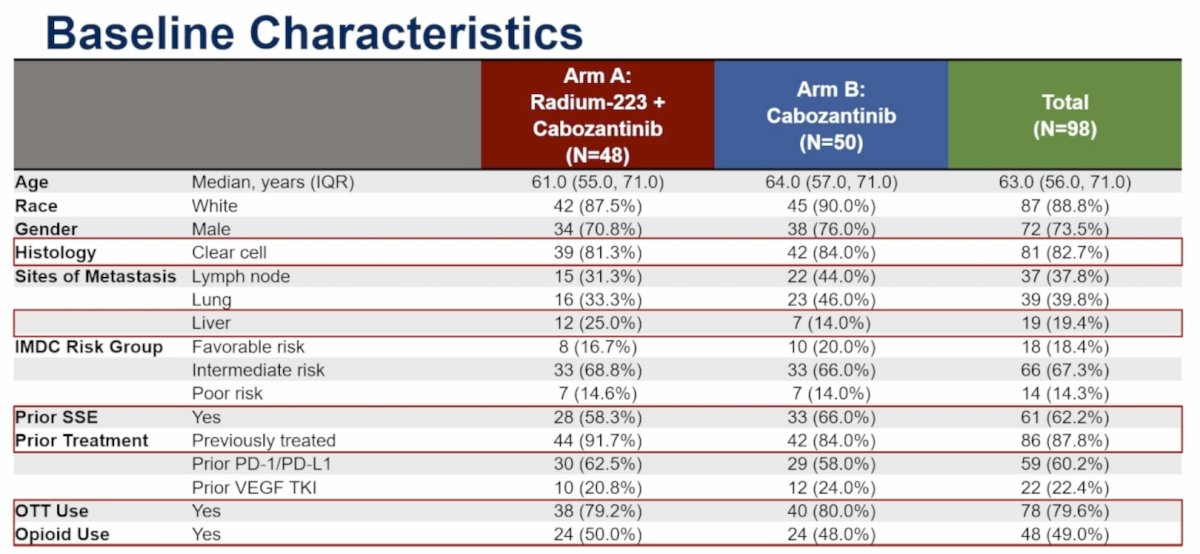
The median age was 63 years (IQR 56-71), 72.3% were male, 88.8% were White, and 82.7% had clear cell histology. Overall, 12.2% were treatment naïve, 79.6% received osteoclast targeted therapy, and 49.0% had baseline opioid use. Regarding IMDC risk, 18.4% were favorable, 67.3% were intermediate, and 14.3% were poor:
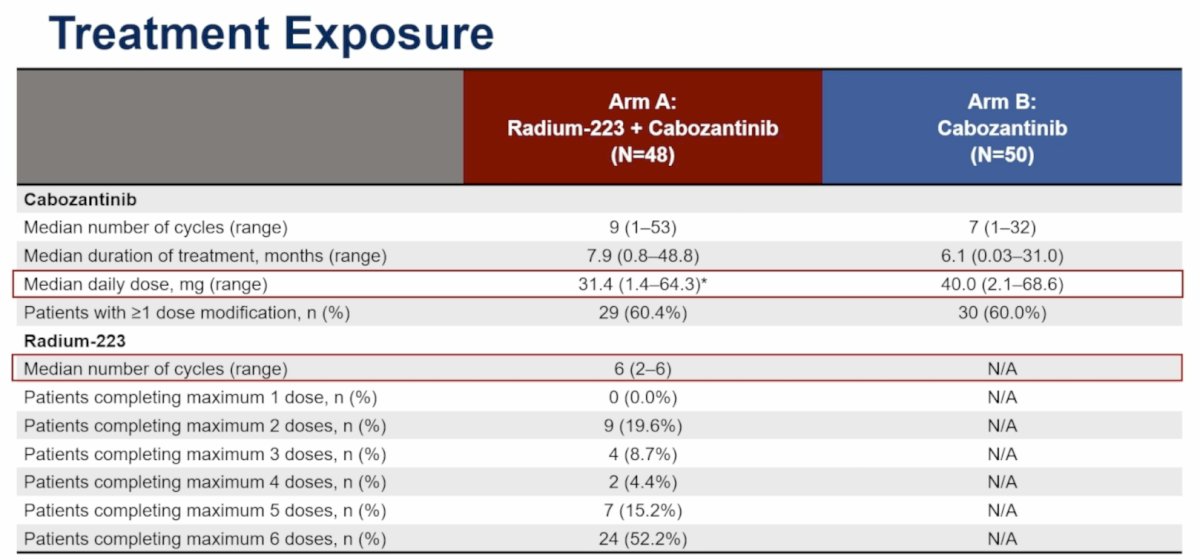
The median cabozantinib dose in Arm A was 31.4 mg (IQR 1.4-64.3) and 40.0 mg (IQR 2.1-68.6) in Arm B; median radium-223 cycles were 6 (IQR 2-6):
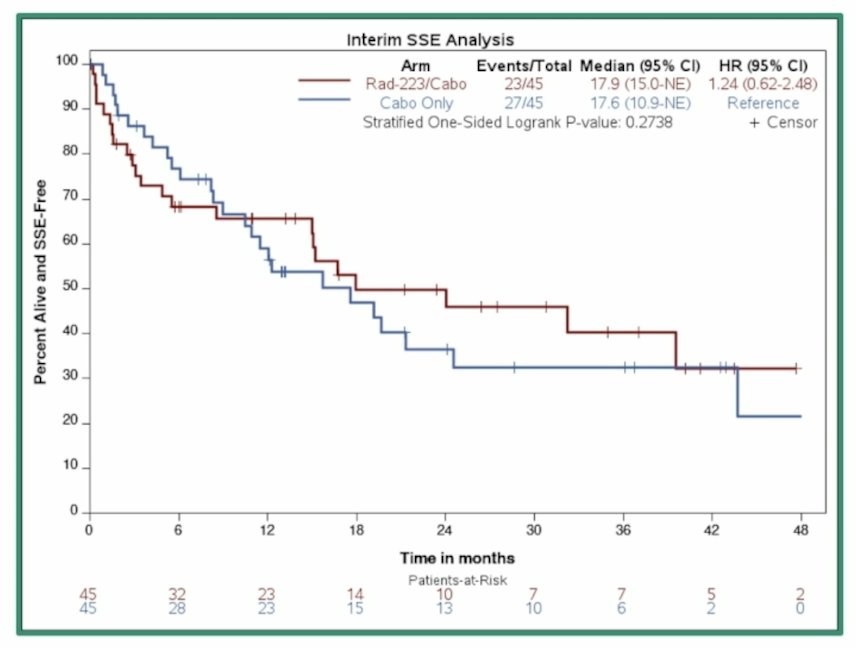
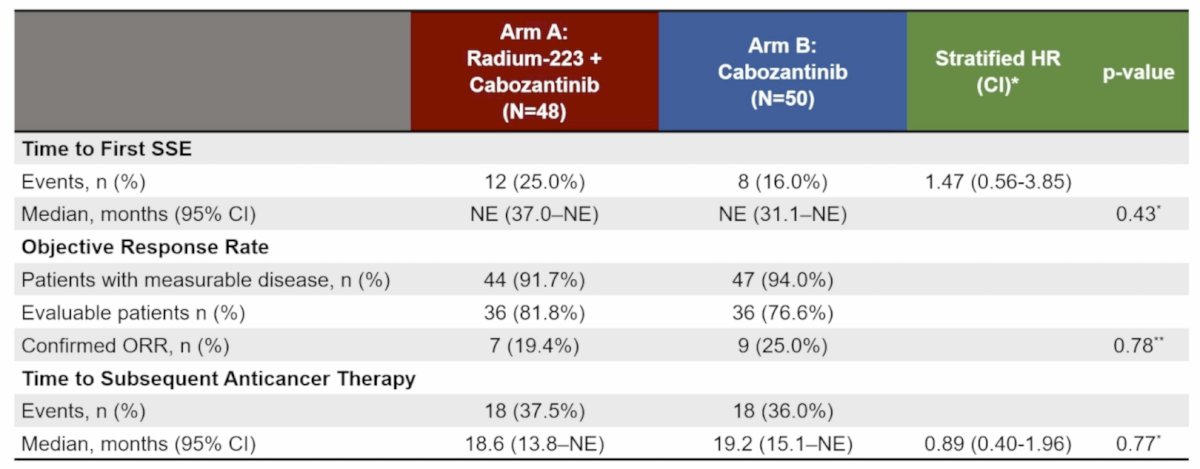
Over a median follow-up of 13.1 (range 0.1-49.4) months with 50 events (n = 90), 17 symptomatic skeletal events (Arm A: 10; Arm B: 7) and 33 deaths (Arm A: 13; Arm B: 20) had occurred. For symptomatic skeletal event free survival, the stratified hazard ratio was 1.24 (95% CI 0.62-2.48), crossing the Wieand futility boundary (HR > 1.0):
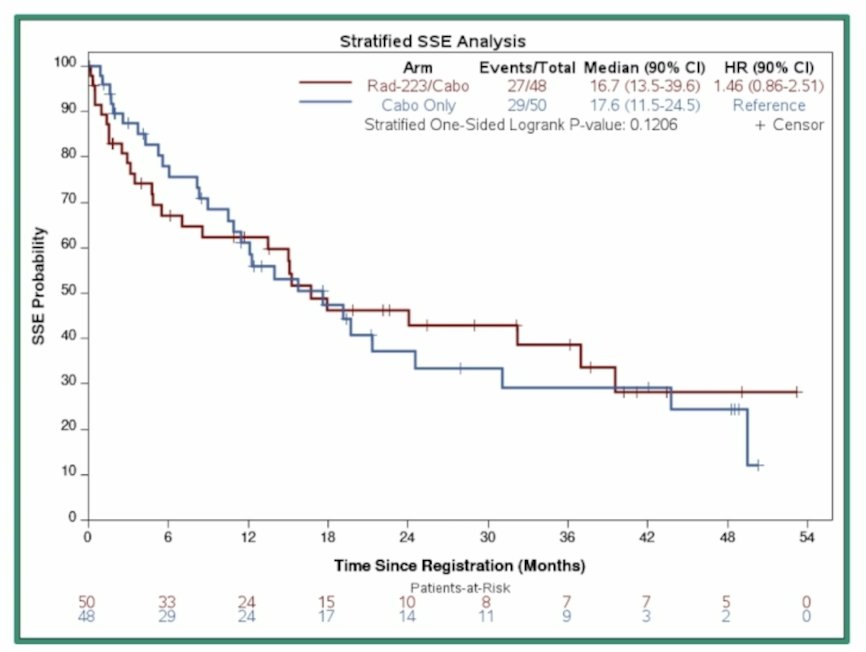
As such, the trial was recommended by the DSMB to close with 98 patients enrolled. Among all enrolled patients, for symptomatic skeletal event free survival, the stratified hazard ratio was 1.46 (90% CI 0.86-2.51):
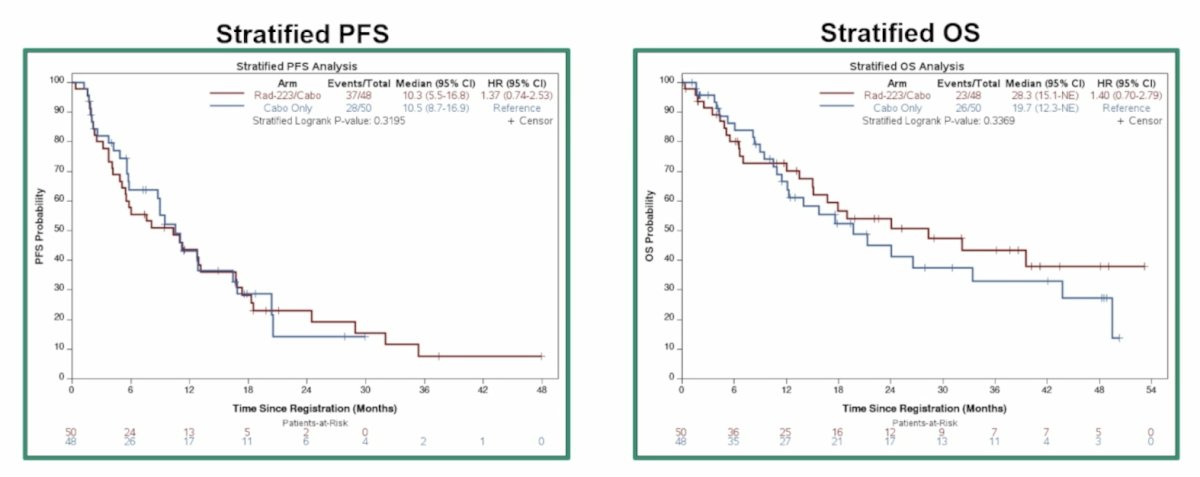
Subgroup analyses for symptomatic skeletal event free survival across IMDC risk, osteoclast targeted therapy use, prior treatment status, and baseline opioid use did not identify any subgroup with a consistent benefit favoring the combination. Among all patients, the stratified progression free survival hazard ratio was 1.37 (95% CI 0.74-2.53), and was 1.40 (95% CI 0.70-2.79) for overall survival:
Among patients evaluable for response, there was an objective response rate of 19.4% for Arm A and 25.0% for Arm B:
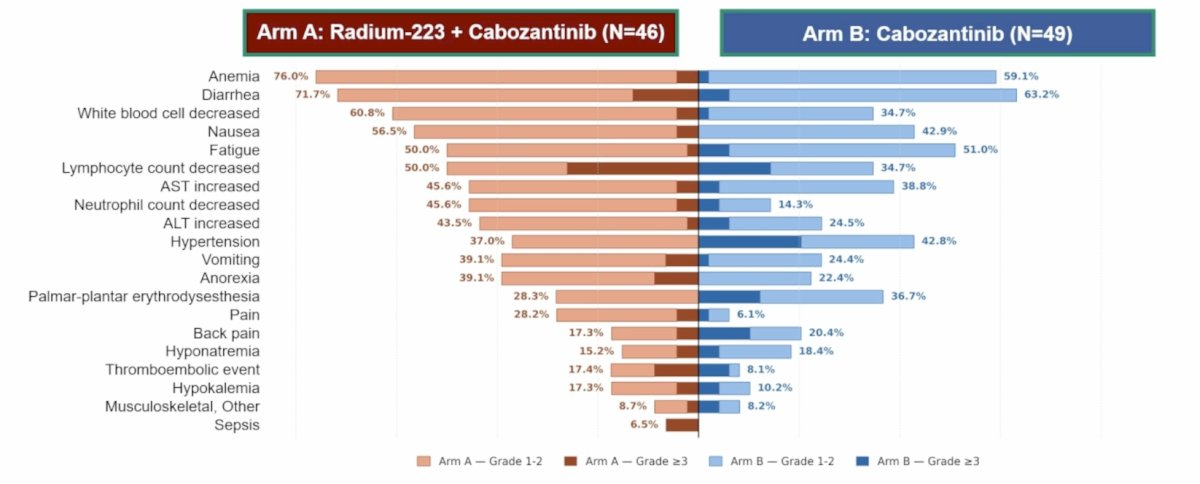
Any grade treatment related adverse events were 97.7% in Arm A and 93.2% in Arm B, and grade ≥3 treatment related adverse events were 65.9% in Arm A and 56.8% in Arm B:
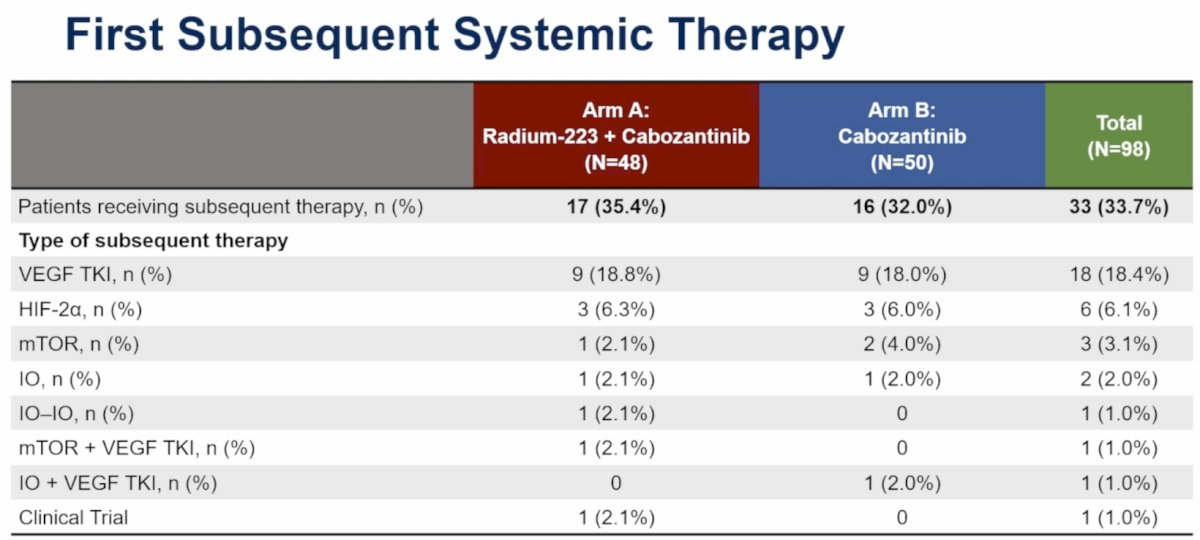
Overall, 35.4% of patients in Arm A and 32.0% of patients in Arm B received a subsequent systemic therapy, most commonly VEGF TKI in both groups (18.8% versus 18.0%):
Dr. McKay noted several limitations of the RADICAL trial:
- Prolonged accrual period: Coincided with major evolution in the RCC treatment landscape, including widespread adoption of immune checkpoint inhibitor-based combinations as first line standard of care
- Over-parameterized model: Four stratification factors relative to a modest sample size led to unstable stratified HR estimates, with substantial divergence from unstratified analyses (stratified HR 1.46 versus unstratified 0.97 for symptomatic skeletal event free survival)
- Low overall symptomatic skeletal event rate: The majority of patients had experienced a prior symptomatic skeletal event and were receiving concurrent osteoclast targeted therapy at baseline, both of which may have mitigated the risk of incident symptomatic skeletal events during the trial, limiting the primary endpoint's ability to detect a treatment effect
Dr. McKay concluded her presentation discussing the RADICAL trial with the following take home points:
- While most patients had a symptomatic skeletal event prior to enrollment, the rate of on trial symptomatic skeletal events was low
- The combination demonstrated no benefit in symptomatic skeletal event free survival, however the overall survival curves diverge after 1 year and remain separated
- The combination was tolerable with a manageable safety profile consistent with the known toxicities of each agent
Presented by: Rana R. McKay, MD, University of California – San Diego, San Diego, CA
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Associate Professor of Urology, Georgia Cancer Center, Wellstar MCG Health, @zklaassen_md on Twitter during the American Society of Clinical Oncology Genitourinary (ASCO) Annual Meeting held in Chicago, IL between May 29th and June 1st, 2026
References:
- McKay RR, Bosse D, Gray KP, et al. Radium-223 dichloride in combination with vascular endothelial growth factor-targeting therapy in advanced renal cell carcinoma with bone metastases. Clin Cancer Res. 2018 Sep 1;24(17):4081-4088.