(UroToday.com) The 2026 American Society of Clinical Oncology Genitourinary (ASCO) Annual Meeting held in Chicago, IL between May 29-June 2, 2026, was host to the Kidney and Bladder Cancer - Posters. Dr. Toni K. Choueiri presented Abstract TPS4636: PEAK-1: A randomized, double-blind, active-control, multicenter phase 3 trial of casdatifan and cabozantinib versus placebo and cabozantinib in patients with advanced clear cell RCC.
Dr Choueiri began by highlighting that clear cell renal cell carcinoma (cRCC) remains the most common histologic subtype of renal cancer, accounting for approximately 70–80% of all cases and carrying a poor prognosis. While the introduction of immune-oncology–based combinations has significantly improved outcomes in the frontline setting, therapeutic options following progression remain limited, with second-line treatment largely relying on tyrosine kinase inhibitor monotherapy. As a result, there continues to be a significant unmet need for more effective therapies for patients with advanced cRCC progressing after prior immune-oncology treatment.
A key biologic hallmark of cRCC is dysregulation of the von Hippel-Lindau pathway, with up to 90% of tumors harboring VHL inactivation. (1-3) Loss of VHL function results in accumulation of hypoxia-inducible factor subunits, particularly HIF-2α, promoting transcriptional programs that drive tumor growth, angiogenesis, and tumor survival. These findings have established HIF-2α as a validated therapeutic target in cRCC. Casdatifan is a potent, selective, orally bioavailable small-molecule HIF-2α inhibitor with a potentially improved pharmacodynamic profile compared with other agents in the class, and early studies have demonstrated encouraging monotherapy activity in advanced cRCC.1-3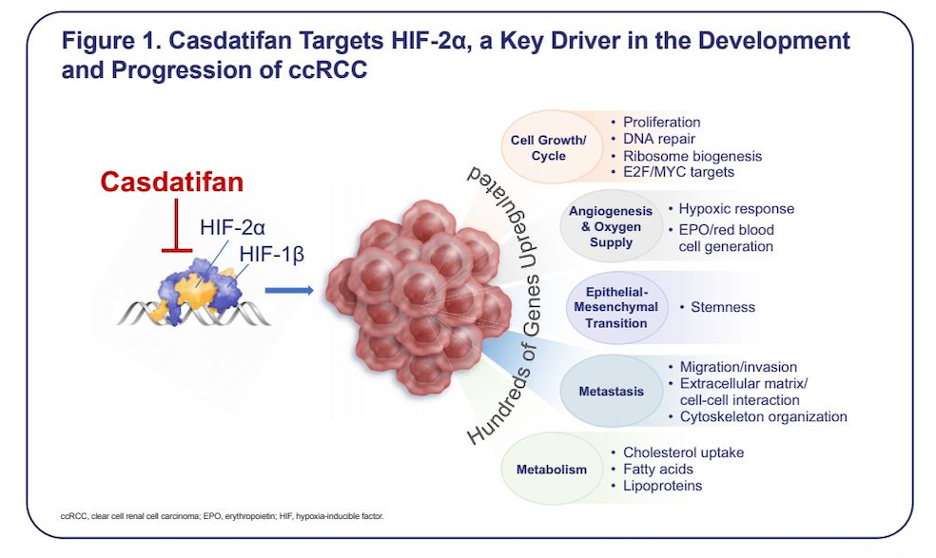
The rationale for combining casdatifan with cabozantinib is based on their complementary mechanisms of action. Cabozantinib, a multitargeted VEGFR tyrosine kinase inhibitor, remains a standard second-line therapy in advanced cRCC. (4) In the ongoing phase 1 ARC-20 study, the combination of casdatifan plus cabozantinib demonstrated encouraging antitumor activity and a manageable safety profile in heavily pretreated patients. As of March 14, 2025, with a median follow-up of 5.3 months, the confirmed objective response rate was 46% (95% CI 25.6–67.2), without evidence of overlapping toxicities. Most anemia and hypoxia events resolved without requiring dose modification. Based on these findings, investigators developed PEAK-1, the first phase 3 trial evaluating casdatifan plus cabozantinib in patients with advanced cRCC following prior immune-oncology therapy.
Dr. Choueiri presented the design of PEAK-1 (NCT07011719), an ongoing phase 3, randomized, active-controlled, double-blind, global multicenter trial evaluating casdatifan in combination with cabozantinib in patients with advanced or metastatic ccRCC who progressed on or after prior anti–PD-1/PD-L1 therapy.
Approximately 720 patients are planned for enrollment and will be randomized in a 2:1 fashion to receive either:
- Casdatifan 100 mg once daily plus cabozantinib 60 mg once daily
- Placebo plus cabozantinib 60 mg once daily
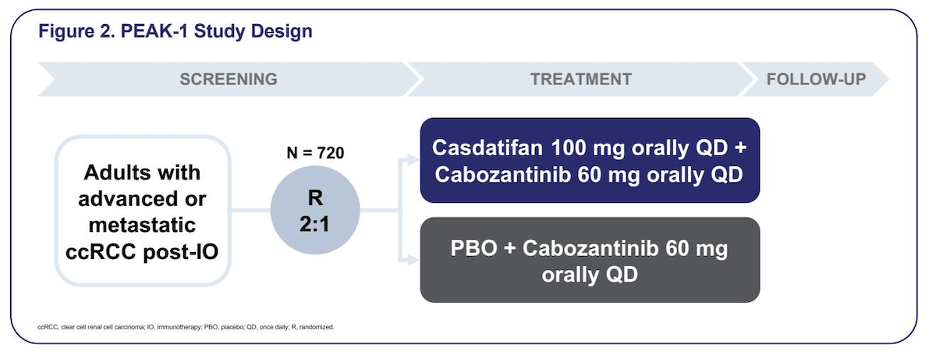
Importantly, crossover between treatment arms is not permitted. Recruitment for the PEAK-1 study is planned across multiple global regions, including Asia, Australia and New Zealand, Europe, Latin America, and North America, supporting broad international enrollment and enhancing the generalizability of the study findings.

Eligible patients must have confirmed advanced or metastatic ccRCC and prior exposure to anti–PD-1 or anti–PD-L1 therapy as part of their most recent regimen, either in the adjuvant setting or first-line metastatic setting in combination with anti–CTLA-4 therapy or a VEGFR-TKI. Patients may have received no more than one prior metastatic regimen. Additional eligibility criteria include Karnofsky Performance Status ≥80%, measurable disease per RECIST 1.1, and adequate organ and marrow function.
Key exclusion criteria include prior treatment with a HIF-2α inhibitor or cabozantinib, ongoing treatment with moderate or strong CYP3A4 inducers, and uncontrolled hypertension despite the use of ≥3 antihypertensive agents. Key inclusion and exclusion criteria are summarized below: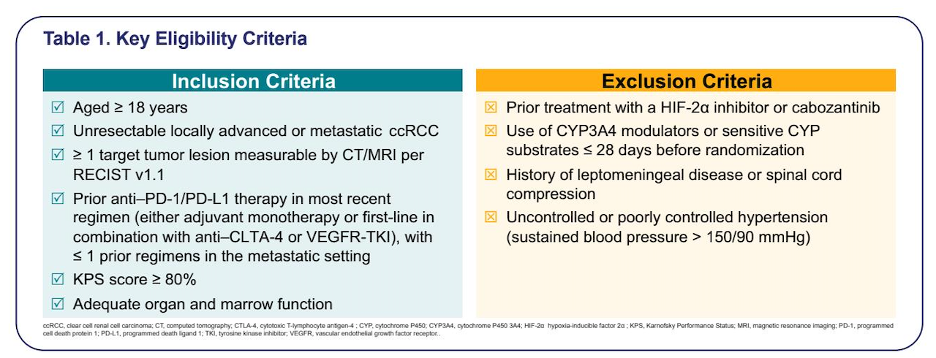
Patients will be stratified according to:
- Geographic region (North America vs Western Europe vs rest of world)
- Prior VEGFR-TKI exposure
- IMDC risk category (favorable vs intermediate/poor)
The primary endpoint is progression-free survival by blinded independent central review per RECIST 1.1. Secondary endpoints include overall survival, objective response rate, duration of response, disease control rate, safety, and patient-reported outcomes using the NFKSI-DRS instrument and are described in detail below: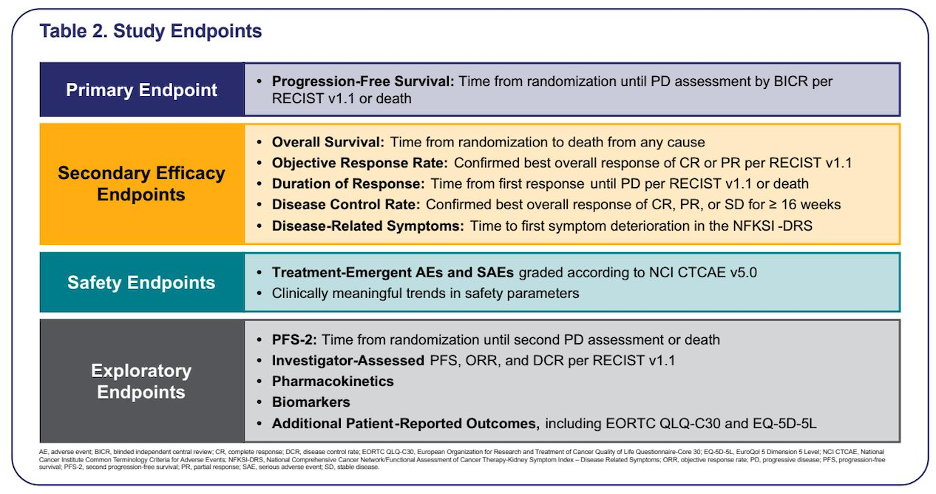
Dr. Choueiri concluded that PEAK-1 is currently the only phase 3 study evaluating the combination of a HIF-2α inhibitor plus a TKI in ccRCC and may help define a novel post-immunotherapy treatment strategy in this disease space.
Presented by: Toni K. Choueiri, MD, Dana Farber Cancer Institute, Boston, MA
Written by: Julian Chavarriaga, MD, Clinical Assistant Professor, Urologic Oncologist, Department of Urology at Penn State Health @chavarriagaj on X during the American Society of Clinical Oncology Genitourinary (ASCO) Annual Meeting held in Chicago, IL between May 29th and June 1st, 2026