(UroToday.com) The 2026 ASCO annual meeting featured a bladder cancer session and a presentation by Dr. Dawood Hasan discussing rethinking the role of tumor size in bladder preservation by comparing survival outcomes of radical cystectomy and trimodal therapy.
Trimodal therapy, consisting of maximal TURBT followed by chemoradiation, is typically reserved for bladder cancer patients with solitary tumors less than 6 cm, no extensive CIS, and no or unilateral hydronephrosis. The National Comprehensive Cancer Network (NCCN) guidelines specify that optimal candidates for bladder preservation with chemoradiotherapy have tumors less than 6 cm; larger tumors have poorer local control and survival outcomes with bladder-sparing approaches. Understanding how tumor size impacts outcomes can help guide treatment decisions between radical cystectomy and trimodal therapy in bladder cancer patients. At ASCO 2026, Dr. Hasan and colleagues aimed to analyze outcomes of bladder cancer patients receiving multimodal therapy and categorize outcomes of radical cystectomy versus trimodal therapy based on tumor sizes.
This was a retrospective cohort analysis of 33,836 patients with urothelial carcinoma of the bladder with clinical stages T1–T4, N0–N3, M0 from the National Cancer Database (2010–2022). Patients were grouped by treatment received: radical cystectomy alone, neoadjuvant chemotherapy + radical cystectomy, radical cystectomy + adjuvant chemotherapy, and trimodal therapy. Overall survival was estimated by Kaplan–Meier methods, and multivariable Cox regression adjusted for confounders was used to compare overall survival among treatment groups and tumor size categories: <3 cm, 3–6 cm, >6 cm.
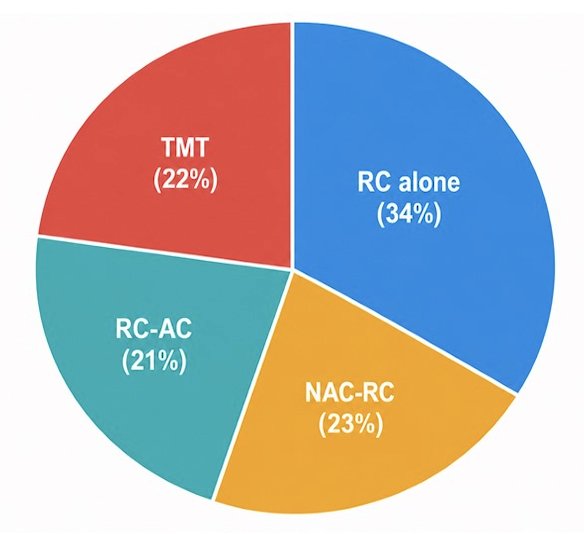
Among 33,836 patients (median age was 68 years), treatment distribution was: radical cystectomy alone (34%), neoadjuvant chemotherapy + radical cystectomy (23%), radical cystectomy + adjuvant chemotherapy (21%), and trimodal therapy (22%):
Tumor size >6 cm versus 3 cm was significantly associated with poor overall survival (HR 1.70, 95% CI 1.62–1.77; p < 0.001). Lymphovascular invasion also independently predicted poorer overall survival (HR 1.94, 95% CI 1.87–2.00, p < 0.001):
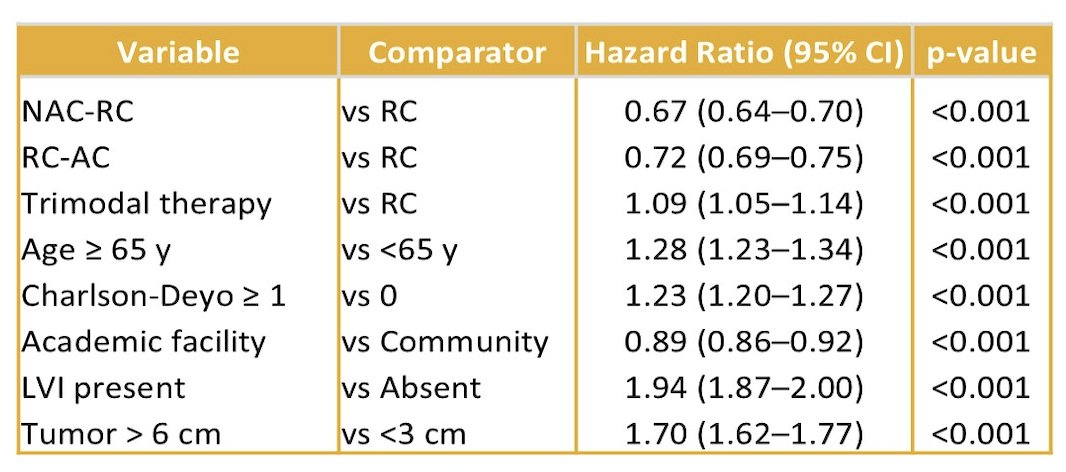
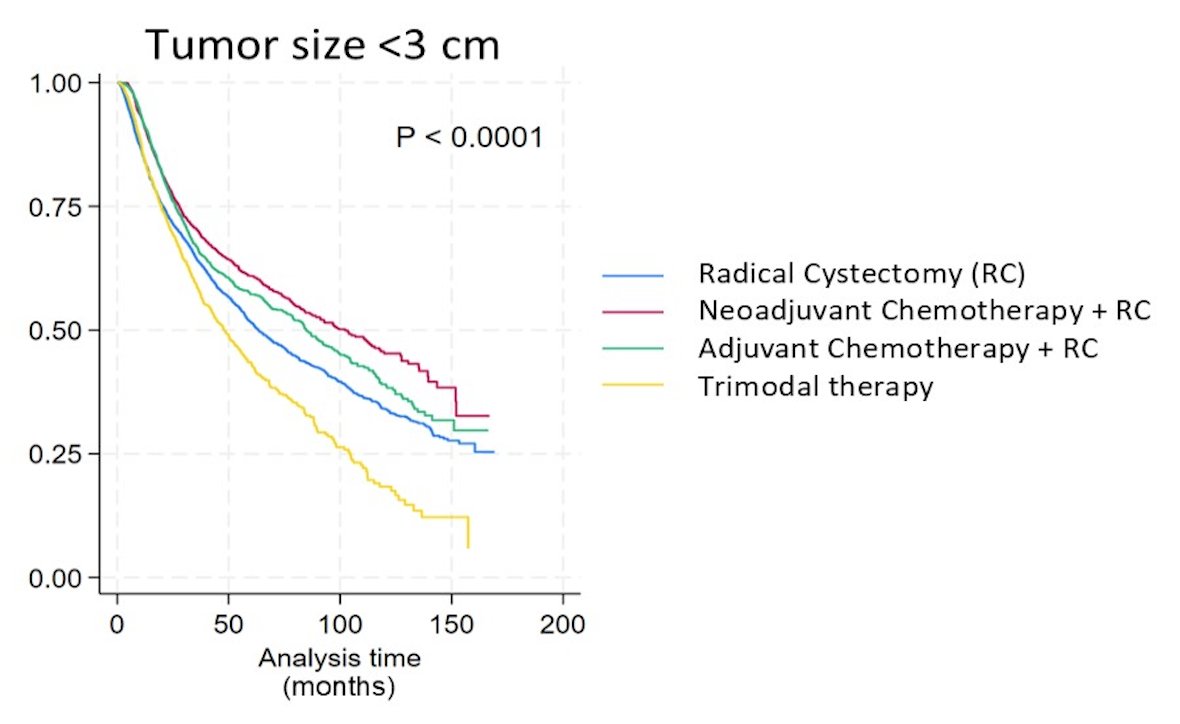
Neoadjuvant chemotherapy + radical cystectomy conferred the greatest overall survival benefit (HR 0.67, 95% CI 0.64–0.70, p = 0.001), and radical cystectomy + adjuvant chemotherapy also improved overall survival (HR 0.72, 95% CI 0.69–0.75, p = 0.001). Radical cystectomy alone and trimodal therapy comparatively had lower survival outcomes. For tumors <3 cm, radical cystectomy was significantly superior to trimodal therapy in overall survival (HR 1.27, 95% CI 1.16–1.39, p < 0.001):
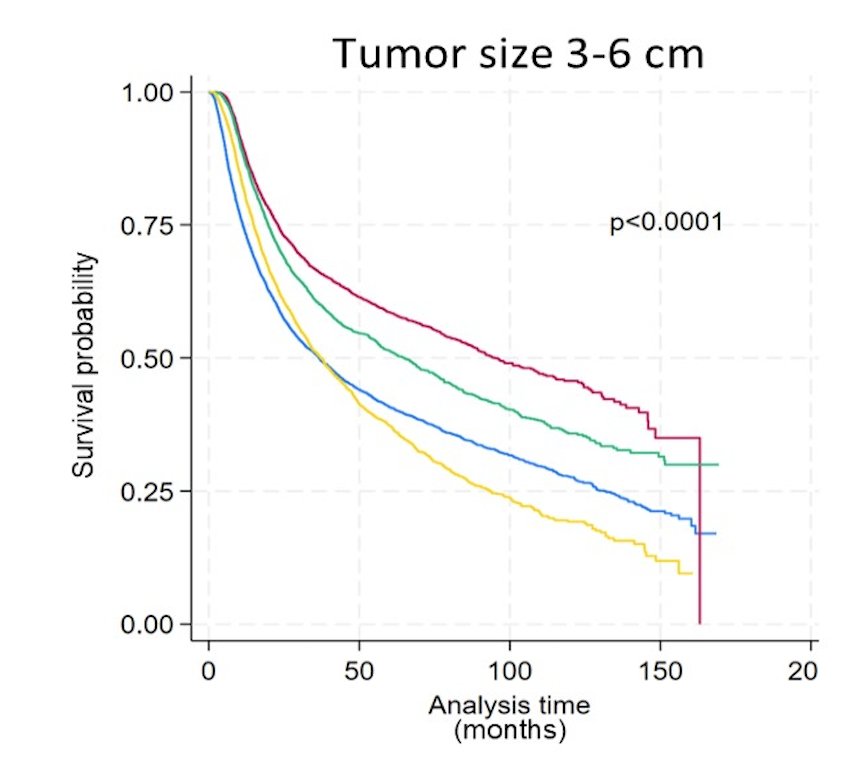
For tumors 3–6 cm, radical cystectomy remained significantly superior to trimodal therapy (HR 1.08, 95% CI 1.03–1.14, p < 0.003):
For tumors >6 cm, there was no significant overall survival difference observed between radical cystectomy and trimodal therapy (HR 0.97, 95% CI 0.88–1.06, p = 0.468).
While neoadjuvant chemotherapy + radical cystectomy remains the standard of care with the highest survival benefits, it is often underutilized due to patient candidacy for chemotherapy. For smaller tumors (<6 cm), surgical removal offers superior outcomes, but for larger tumors (>6 cm), the aggressiveness likely negates surgical advantages, resulting in comparable survival to bladder preservation. These findings support personalized treatment decision-making, emphasizing bladder preservation in large tumors without other contraindications such as hydronephrosis.
Dr. Hasan concluded his presentation discussing rethinking the role of tumor size in bladder preservation by comparing survival outcomes of radical cystectomy and tri-modality therapy with the following take-home points:
- Tumor size is a critical prognostic factor influencing overall survival in bladder cancer treatments
- Neoadjuvant chemotherapy + radical cystectomy provides the greatest survival benefit
- Radical cystectomy is significantly superior to trimodal therapy in tumors smaller than 6 cm
- For tumors larger than 6 cm, no significant survival benefit between radical cystectomy and trimodal therapy was seen in this study
- Bladder preservation strategies should be considered for tumors greater than 6 cm if other contraindications are absent
Presented by: Dawood Hasan, MD, Geisinger Health System, Danville, PA
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Associate Professor of Urology, Georgia Cancer Center, Wellstar MCG Health, @zklaassen_md on Twitter during the American Society of Clinical Oncology Genitourinary (ASCO) Annual Meeting held in Chicago, IL between May 29th and June 1st, 2026