(UroToday.com) The 2026 ASCO annual meeting featured a urothelial carcinoma rapid abstract session and a presentation by Dr. Maria De Santis discussing the 5-year overall survival analysis and patient-reported outcomes from POTOMAC assessing durvalumab in combination with BCG induction and maintenance therapy for BCG-naïve, high-risk non-muscle invasive bladder cancer.
Patients with high-risk non-muscle invasive bladder cancer potentially face a lifelong disease burden with substantial quality of life implications. In the phase 3 POTOMAC study (NCT03528694), 1 year of durvalumab in combination with BCG (induction + maintenance) resulted in a statistically significant and clinically meaningful improvement in disease-free survival versus BCG (induction + maintenance) alone, with a manageable safety profile, in patients with BCG-naive, high-risk non-muscle invasive bladder cancer.1 Additionally, at AUA 2026, Dr. Neal Shore reported a few cystectomies and a favorable trend for cystectomy-free survival in the durvalumab arm. At the ASCO 2026 annual meeting, Dr. De Santis reported a planned updated 5-year overall survival analysis and patient-reported outcomes.
Eligible patients were randomized 1:1:1 to durvalumab + BCG (induction + maintenance), durvalumab + BCG (induction only), or BCG (induction + maintenance):
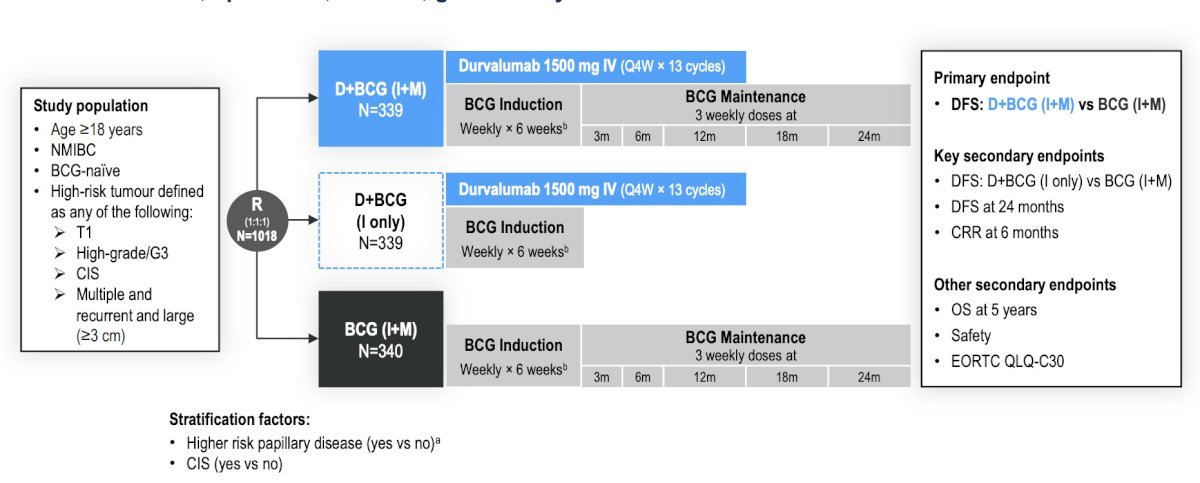
Secondary endpoints included 5-year overall survival and patient-reported outcomes, evaluated every 8 weeks by EORTC QLQ-C30 and every 4 weeks by EORTC QLQ-NMIBC24 and PRO-CTCAE. Prespecified priority subscales were global health status/quality of life (GHS/QoL), physical functioning, and fatigue for QLQ-C30; and urinary symptoms, intravesical treatment issues, future perspective/worries, and sexual functioning for QLQ-NMIBC24:
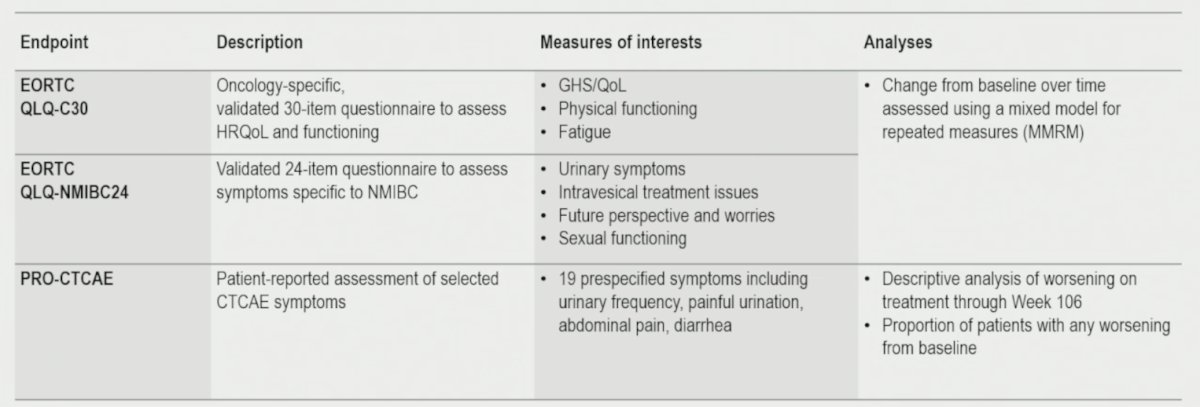
Change from baseline (mixed model for repeated measures) was assessed, with a ±10-point score considered clinically meaningful.
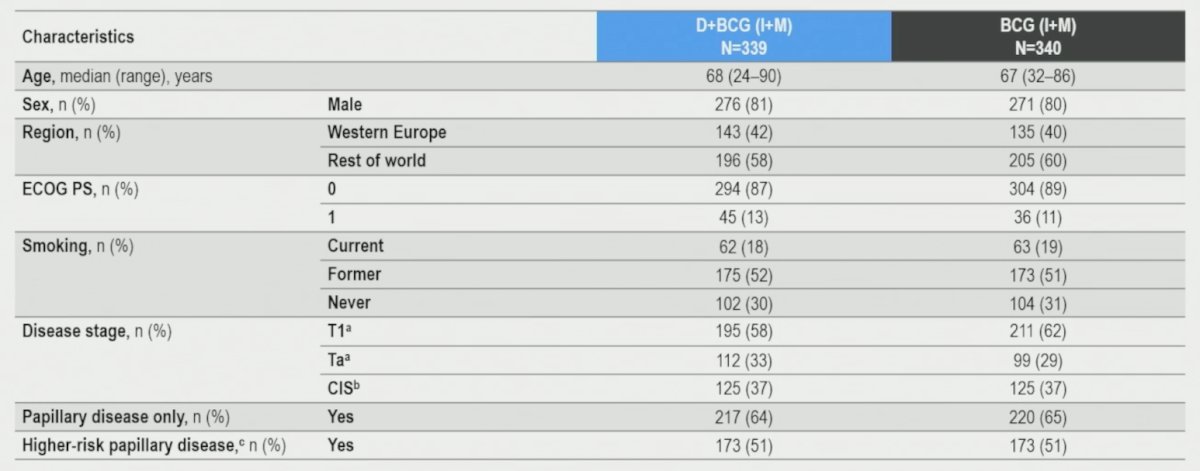
The following table highlights the baseline characteristics among patients in the intention-to-treat population:
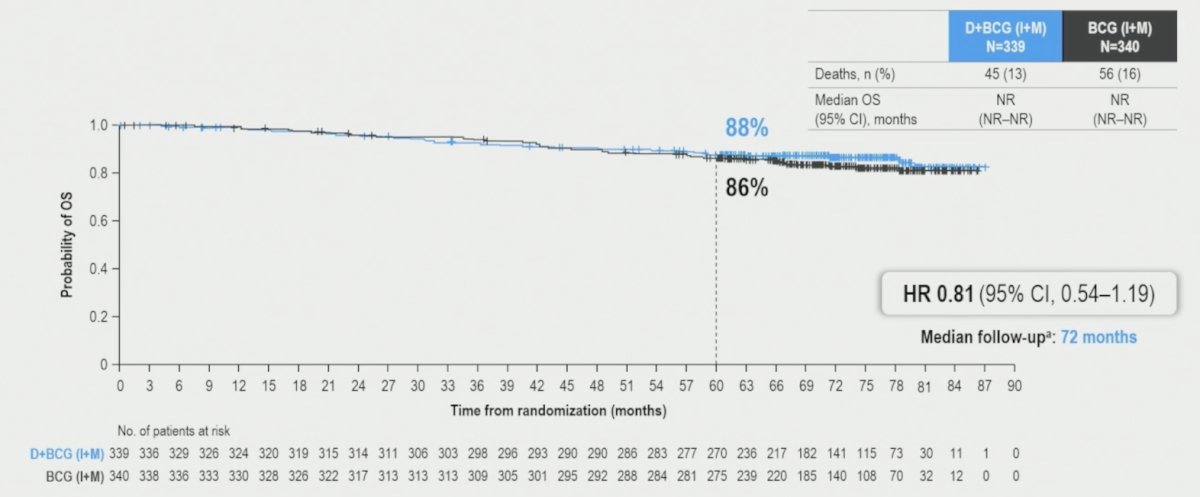
At data cutoff October 3, 2025 (median follow-up 72 months), the overall survival HR was 0.81 (95% CI, 0.54–1.19) with a 5-year overall survival rate of 87.6% (95% CI, 83.5%–90.8%) for durvalumab + BCG (induction + maintenance) versus 86.3% (95% CI, 82.1%–89.6%) for BCG (induction + maintenance). The median overall survival was not reached in either arm:
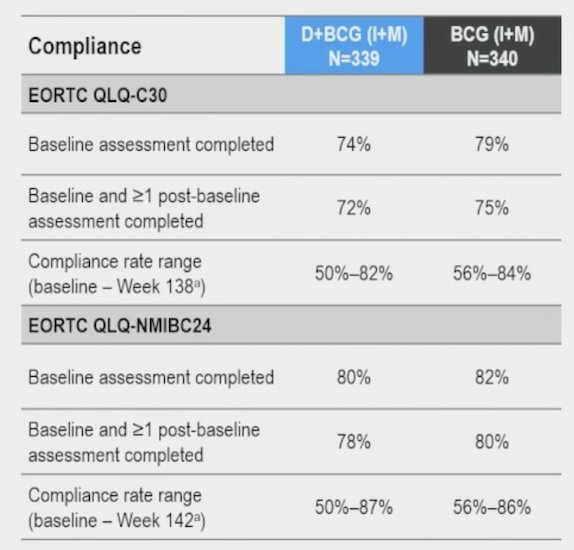
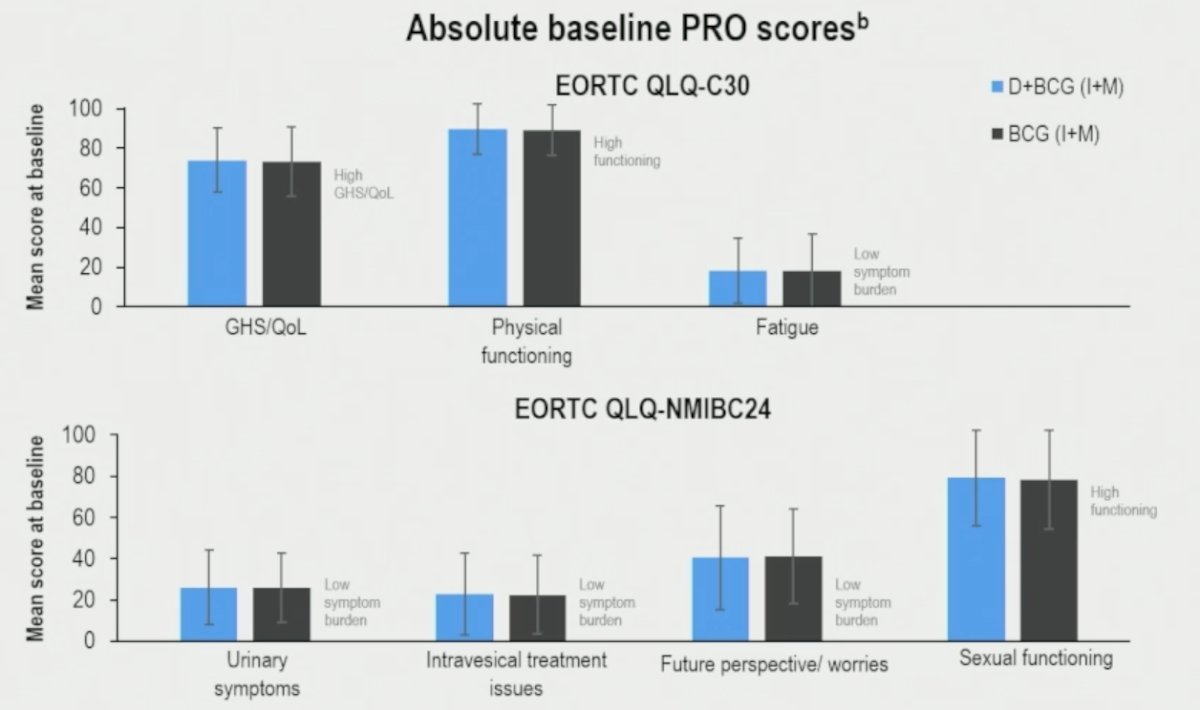
For patient-reported outcome analyses (data cutoff April 3, 2025), QLQ-C30 and QLQ-NMIBC24 baseline compliance rates were ≥74% and ≥79%, respectively, with similar baseline scores between arms:
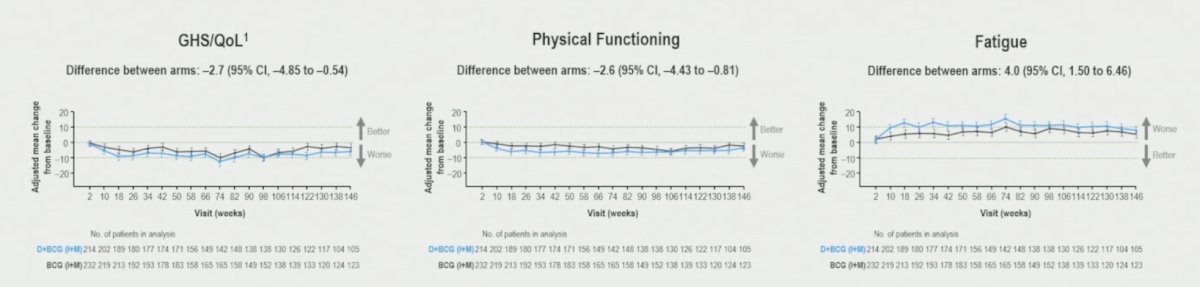
Overall, both arms showed deterioration in QLQ-C30 adjusted mean change from baseline scores, with suggested clinically meaningful deterioration for fatigue with durvalumab + BCG (induction + maintenance), however the difference between arms was small:
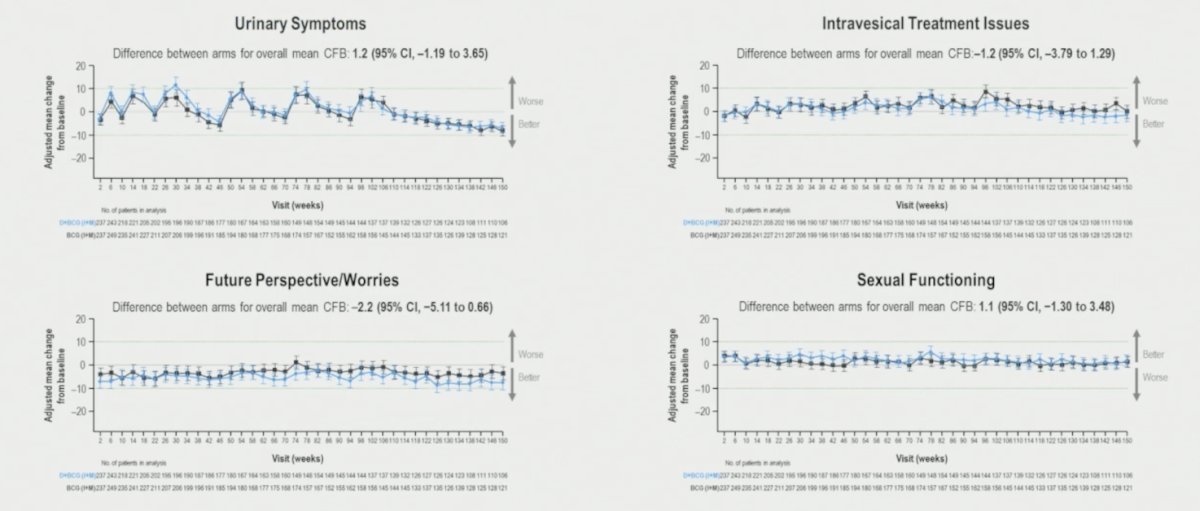
Overall, QLQ-NMIBC24 adjusted mean change from baseline scores were numerically small and similar between arms:
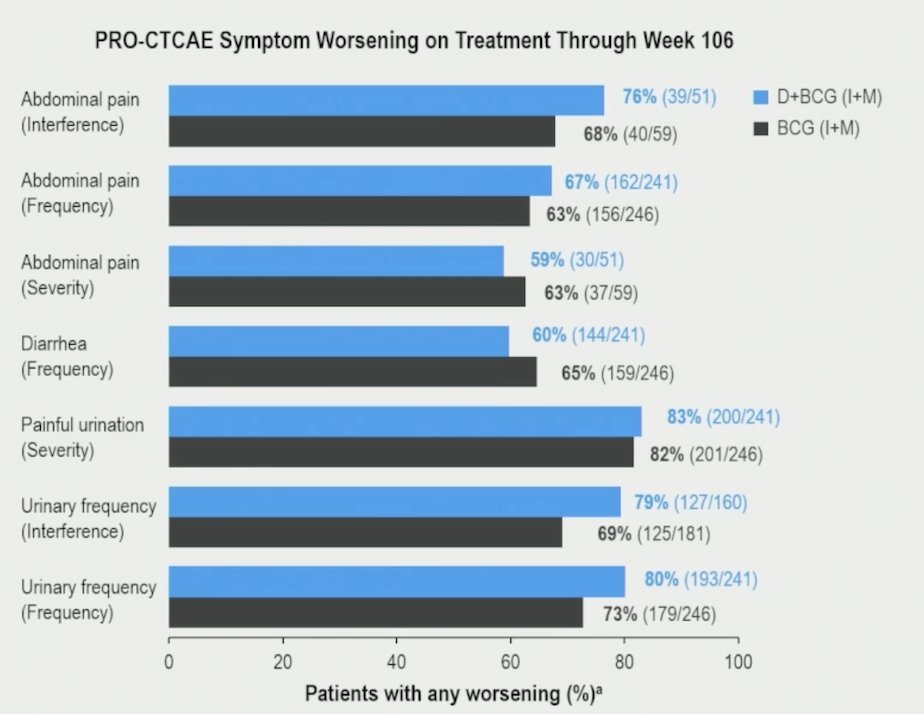
Across abdominal pain, diarrhea, and painful urination, rates of PRO-CTCAE worsening were similar between treatment arms through week 106, consistent with the shared BCG treatment backbone. For urinary frequency, rates of PRO-CTCAE worsening were numerically higher in the durvalumab + BCG arm (80%) versus the BCG arm (73%), with a difference <= 10%:
Dr. De Santis concluded her presentation discussing the 5-year overall survival analysis and patient-reported outcomes from POTOMAC with the following take-home points:
- At the planned 5-year overall survival analysis, the addition of durvalumab to BCG (induction + maintenance) continued to show no detriment to overall survival (HR 0.81, 95% CI 0.54-1.19)
- The addition of durvalumab to BCG (induction + maintenance) did not have a major impact on patient-reported quality of life, with generally similar patient-reported outcomes between the treatment arms
- These data further support 1 year of durvalumab in combination with BCG induction and maintenance as a new treatment for patients with BCG-naïve, high-risk non-muscle invasive bladder cancer
Presented by: Maria De Santis, MD, PhD, Medical Oncologist, Section Head, Interdisciplinary GU-Oncology, Charité Universitätsmedizin Berlin, Berlin, Germany; Paracelsus Medizinische Privatuniversität, Salzburg, Austria; University of Warwick, Warwick, England
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Associate Professor of Urology, Georgia Cancer Center, Wellstar MCG Health, @zklaassen_md on Twitter during the American Society of Clinical Oncology Genitourinary (ASCO) Annual Meeting held in Chicago, IL between May 29th and June 1st, 2026
Reference: