(UroToday.com) The 2026 American Society of Clinical Oncology (ASCO) Annual Meeting was host to a kidney and bladder cancers poster session. Dr. Andrea Malgeri presented a reconstructed individual patient data (IPD) analysis of the NIAGARA trial1 assessing the magnitude and timing of clinical benefit associated with pathologic complete responses (pCR) in perioperative muscle-invasive bladder cancer (MIBC).
pCR is widely used as an early efficacy endpoint in perioperative bladder cancer trials, although its association with long-term outcomes remains poorly validated. The objective of this study was to quantify the magnitude and timing of event-free survival (EFS) and overall survival (OS) benefit associated with pCR in the NIAGARA trial using reconstructed individual patient data (IPD).
Individual patient data were reconstructed from publicly available Kaplan-Meier curves using the IPDfromKM package. NIAGARA randomized patients with MIBC to perioperative durvalumab plus neoadjuvant chemotherapy followed by adjuvant durvalumab or neoadjuvant chemotherapy alone. Treatment effects were assessed using restricted mean survival time (RMST) analyses, with expected average survival time (EAST) used to estimate the absolute benefit associated with pCR. Time-to-benefit (TTB) was defined as the earliest time point at which RMST exceeded one month. EFS and OS were compared between patients who achieved pCR and those who did not across treatment arms.
Restricted mean survival time analyses demonstrated that achievement of pCR was associated with significant EFS and OS gains in both treatment arms (Table 1). In the durvalumab plus chemotherapy arm (Durva-CG), pCR was associated with an EFS gain of 5.87 months (95% CI 4.78–6.96; p<0.0001) and an OS gain of 5.32 months (95% CI 3.89–6.74; p<0.0001) compared to patients without pCR. Time-to-benefit was reached at 9 months for EFS and 22 months for OS. Similarly, in the chemotherapy-alone arm (CG), pCR was associated with an EFS gain of 5.63 months (95% CI 4.49–6.77; p<0.0001) and an OS gain of 5.89 months (95% CI 4.30–7.47; p<0.0001), with time-to-benefit achieved at 9 months for EFS and 20 months for OS.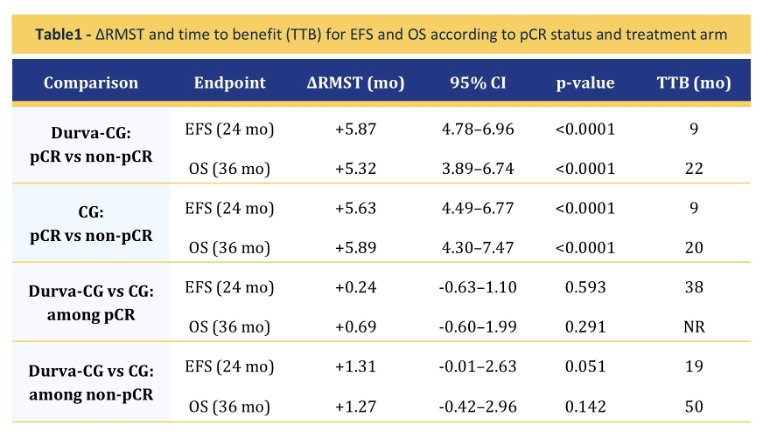
Direct comparisons between treatment arms according to pCR status demonstrated no significant differences in outcomes among patients who achieved pCR. Among pCR responders, the difference in EFS between Durva-CG and CG was 0.24 months (95% CI −0.63 to 1.10; p=0.593), while the difference in OS was 0.69 months (95% CI −0.60 to 1.99; p=0.291). Similarly, among patients who did not achieve pCR, no significant differences were observed between treatment arms for EFS.
The reconstructed survival analyses further quantified the magnitude and timing of benefit associated with pCR. As illustrated in Figure 1, the EFS benefit associated with pCR emerged earlier than the OS benefit. The earliest time point at which the absolute EFS benefit exceeded one month occurred at approximately 9 months, whereas the corresponding OS benefit emerged later, at 22 months. The reconstructed EFS and OS curves demonstrated progressively greater survival gains over time among patients achieving pCR, with larger absolute gains observed in the durvalumab-containing arm.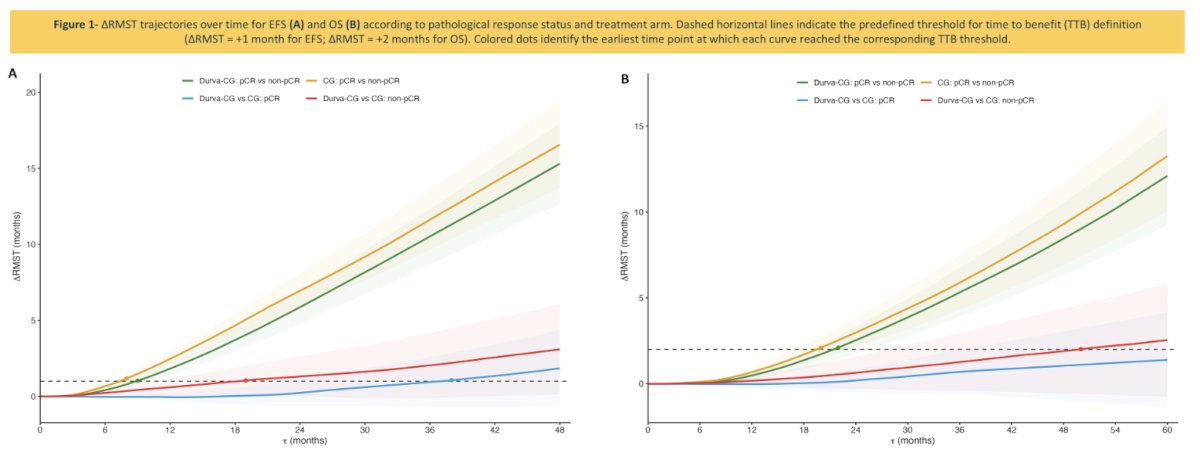
The investigators concluded that, using reconstructed individual patient data from the NIAGARA trial, pCR was associated with a large and early EFS benefit and a later but substantial OS benefit. pCR in perioperative MIBC remained associated with long-term survival benefit across treatment arms. Importantly, the absence of significant survival differences between treatment arms among patients who achieved pCR or among those who did not achieve pCR suggests that long-term survival differences may be predominantly driven by pCR achievement itself rather than treatment-related modulation within pCR prognostic response strata.
Presented by: Andrea Malgeri, MD, Resident Physician, Medical Oncology, Università Campus Bio-Medico di Roma, Rome, Italy
Written by: Rashid K. Sayyid, MD, MSc, Assistant Professor, Urologic Oncologist, Department of Urology at The University of Arizona and Banner University Medical Center, Tucson, AZ – @rksayyid on X during the American Society of Clinical Oncology Genitourinary (ASCO) Annual Meeting held in Chicago, IL between May 29th and June 1st, 2026
Reference: