(UroToday.com) The 2026 American Society of Clinical Oncology (ASCO) Annual Meeting was host to a kidney and bladder cancers poster session. Dr. Jeffrey Zhong presented a UNITE analysis of the effect of on-treatment dose adjustments on the efficacy of enfortumab vedotin + pembrolizumab (EV + pembro) in advanced urothelial carcinoma (aUC).
EV + pembro has become the preferred frontline regimen for patients with locally advanced or metastatic urothelial carcinoma based on the results of the EV-302 trial that demonstrated a significant improvement in overall survival (OS) with EV + pembro versus platinum-based chemotherapy (31.5 versus 16.1 months; HR: 0.47, 95% CI 0.38–0.58).1 However, treatment-related toxicities—including rash, neuropathy, fatigue, and hyperglycemia—commonly lead to EV dose interruptions. Prior analyses of EV monotherapy have suggested that dose adjustments may not adversely affect clinical outcomes, but data evaluating this question in patients receiving EV + pembro combination therapy have remained limited. This study aimed to address that knowledge gap using real-world multicenter data from the UNITE cohort.
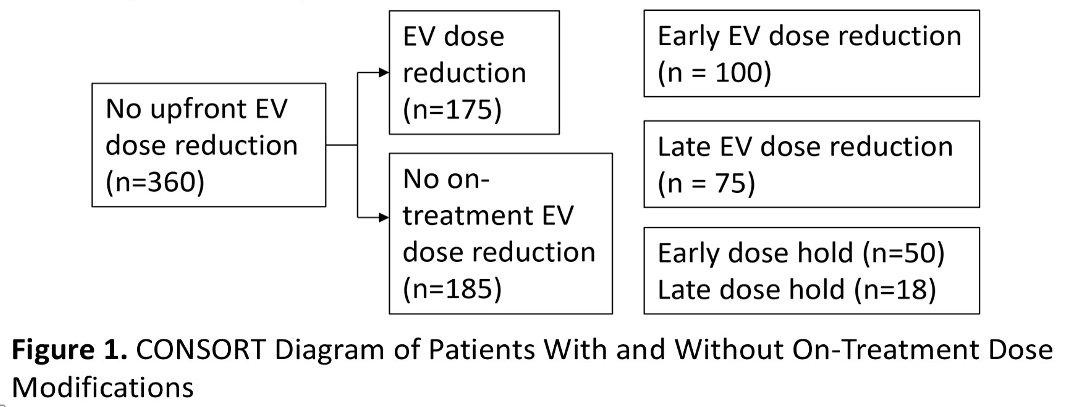
This analysis utilized the multi-institutional UNITE database. Patients treated with first-line EV + pembro were evaluated according to the presence or absence of EV dose reductions (DRs) and dose holds. Patients with upfront EV dose reductions were excluded. Early dose modifications were defined as occurring within 9 weeks of EV + pembro initiation, whereas late dose modifications occurred after 9 weeks. Kaplan-Meier methods and Cox proportional hazards models were used to evaluate investigator-assessed PFS and OS. Multivariable analyses adjusted for age (<75 versus ≥75 years), ECOG performance status (0–1 versus 2–3), hemoglobin (<10 versus ≥10 g/dL), and presence of liver metastases. To minimize immortal time bias, a time-dependent covariate analysis was performed, supplemented by landmark analyses aligned to treatment cycles 2 through 7.
A total of 360 patients receiving EV + pembro without upfront dose reduction were included. Among these patients, 175 (48.6%) experienced at least one EV dose reduction, whereas 185 (51.4%) had no on-treatment dose reduction. Within the dose reduction cohort, 100 patients had an early dose reduction, and 75 patients had a late dose reduction. Dose holds were less common, occurring in 68 patients overall, including 50 early dose holds and 18 late dose holds.
Baseline cohort characteristics demonstrated a median age of 70 years and a median follow-up of 11.7 months (95% CI 10.79–13.08). Most patients were Caucasian (78%), 27% had upper tract primary tumors, 35% had de novo metastatic disease, 77% had ECOG performance status 0–1, 17% had liver metastases, and 78% received EV + pembro in the first-line setting. Notably, 52% of late dose adjustments were attributed to neuropathy.
Paradoxically, EV dose reductions were associated with improved outcomes rather than inferior outcomes. In multivariable and time-dependent analyses, dose reduction was associated with significantly longer PFS and OS compared with no dose reduction:
- PFS: HR 0.47 (95% CI 0.34–0.66; p<0.001)
- OS: HR 0.44 (95% CI 0.29–0.66; p<0.001)
These findings were further supported by landmark analyses aligned to treatment cycles. For PFS, the hazard ratios associated with dose reduction became increasingly favorable with later treatment cycles:
- Cycle 2: HR 0.89 (95% CI 0.46–1.72)
- Cycle 3: HR 1.09 (95% CI 0.66–1.81)
- Cycle 4: HR 1.34 (95% CI 0.76–2.68)
- Cycle 5: HR 1.65 (95% CI 0.74–3.67)
- Cycle 6: HR 2.03 (95% CI 0.68–6.06)
- Cycle 7: HR 2.50 (95% CI 0.61–10.28)

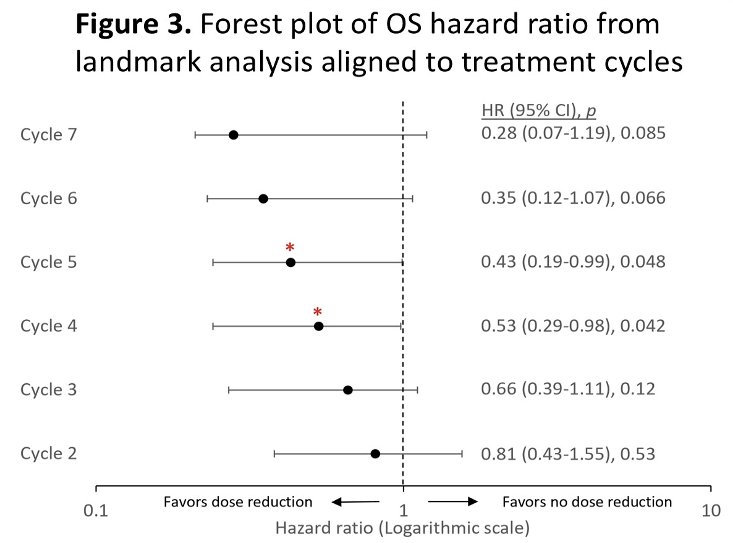
Similarly, OS landmark analyses demonstrated favorable outcomes among patients who underwent dose reductions:
- Cycle 2: HR 0.81 (95% CI 0.43–1.55)
- Cycle 3: HR 0.66 (95% CI 0.39–1.11)
- Cycle 4: HR 0.43 (95% CI 0.19–0.99)
- Cycle 5: HR 0.53 (95% CI 0.29–0.98)
- Cycle 6: HR 0.35 (95% CI 0.12–1.07)
- Cycle 7: HR 0.28 (95% CI 0.07–1.19)
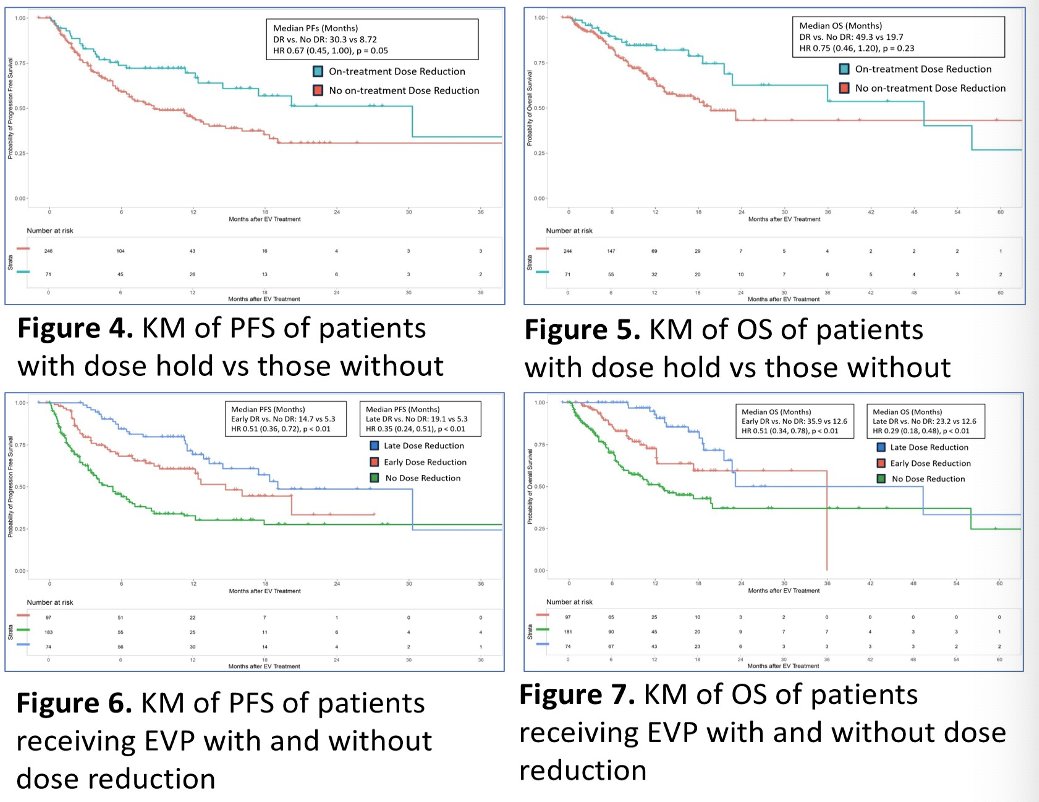
In contrast, dose holds did not significantly impact outcomes. Multivariable and time-dependent analyses demonstrated no statistically significant prolongation of either PFS or OS among patients who experienced dose holds compared with those who did not:
- PFS: HR 0.65 (95% CI 0.40–1.05; p=0.08)
- OS: HR 0.70 (95% CI 0.39–1.27; p=0.24)
Kaplan-Meier analyses further illustrated these findings. Patients who underwent EV dose reductions demonstrated superior PFS and OS compared with those without dose reduction, whereas the survival curves for patients with versus without dose holds largely overlapped. Forest plot analyses showed consistent benefit associated with dose reduction across landmark cycles and clinical subgroups.
The investigators concluded that on-treatment EV dose reductions were not associated with inferior outcomes and were, in fact, associated with significantly improved PFS and OS in patients receiving EV + pembro for advanced urothelial carcinoma. Conversely, dose holds did not significantly affect survival outcomes. These findings suggest that clinically indicated EV dose reductions can be implemented without compromising efficacy and may help optimize treatment tolerability while maintaining favorable oncologic outcomes.
Presented by: Jeffrey Y. Zhong, MD, Resident Physician, University Hospitals, Case Western Reserve University, Cleveland, OH, USA
Written by: Rashid K. Sayyid, MD, MSc, Assistant Professor, Urologic Oncologist, Department of Urology at The University of Arizona and Banner University Medical Center, Tucson, AZ – @rksayyid on X during the American Society of Clinical Oncology Genitourinary (ASCO) Annual Meeting held in Chicago, IL between May 29th and June 1st, 2026
References: