(UroToday.com) The 2026 American Society of Clinical Oncology (ASCO) Annual Meeting was host to a kidney and bladder cancers poster session. Dr. Michal Sternschuss presented an analysis of outcomes with enfortumab vedotin re-challenge after disease progression in metastatic urothelial carcinoma (mUC).
EV, either as monotherapy or in combination with pembrolizumab (EV + pembro), is now an established, front-line treatment option for patients with advanced urothelial carcinoma.1 However, outcomes with EV rechallenge after prior EV exposure and subsequent progression remain poorly characterized, particularly as EV-based therapy increasingly moves into earlier disease settings. This retrospective institutional analysis sought to evaluate the clinical activity of EV rechallenge and identify features associated with potential benefit.
Dr. Sternschuss and colleagues reviewed an institutional database of patients treated with EV monotherapy (n=395) or EV + pembro (n=256) for mUC and identified patients who subsequently underwent EV rechallenge after disease progression. The EV-free interval (EVFI) was defined as the time from the last EV1 dose to the first EV2 dose. The clinical outcomes included investigator-assessed objective response rate (ORR), progression-free survival (PFS), overall survival (OS), and duration of response (DoR).
Among 42 identified patients:
- Median age was 77 years
- 76% were male
- 45% had upper tract primary tumors
- Initial EV regimen (EV1) was EV monotherapy in 62% (n=26) and EV + pembro in 38% (n=16)
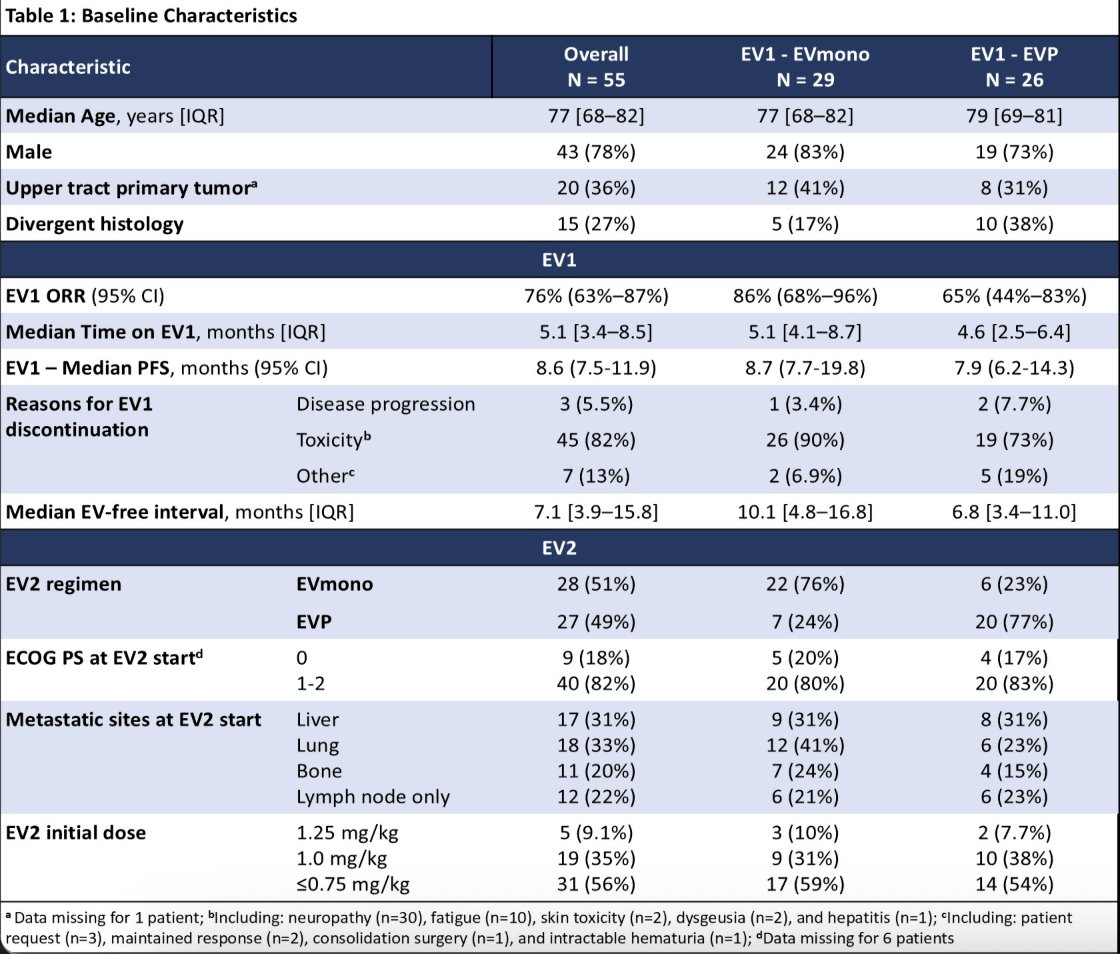
Importantly, most patients discontinued initial EV primarily because of toxicity rather than progression:
- 83% (n=35) stopped EV1 due to toxicity
- Peripheral neuropathy was the predominant reason for discontinuation
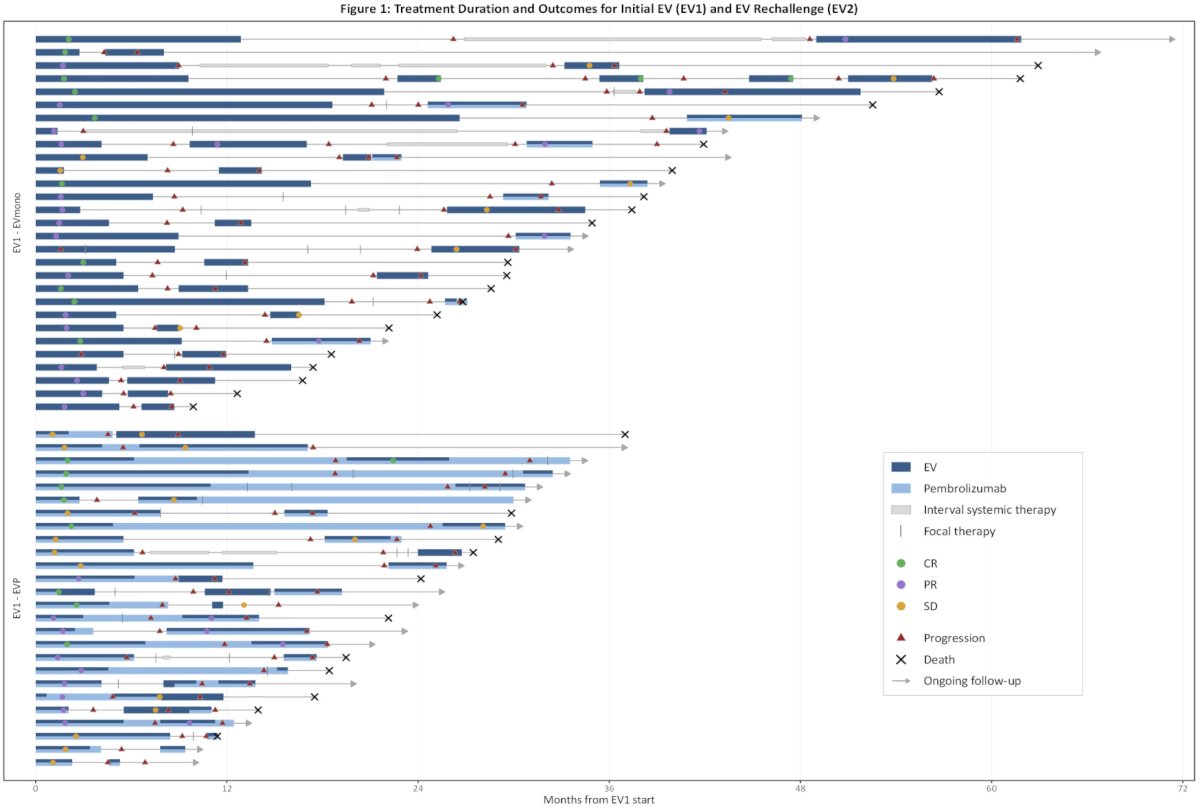
The median follow-up from EV2 initiation was 26 months (95% CI 17–NR). At the time of rechallenge:
- 24% (n=10) switched EV regimens
- EV monotherapy → EV + pembro: n=5
- EV + pembro → EV monotherapy: n=5
- EV2 dosing was reduced in most patients:
- 1.25 mg/kg: 9.5%
- 1.0 mg/kg: 31%
- ≤0.75 mg/kg: 60%
Among response-evaluable patients (n=39), the ORR to EV rechallenge was 21% (8/39; 95% CI 9%–36%), including:
- Complete response: 5% (2 patients)
- Both CRs occurred in patients who had previously achieved CR to EV1
Notably, no responses were observed in:
- Patients with stable disease or progressive disease had the best response to EV1 (0/8)
- Patients with EV1 PFS <6 months (0/11)
Clinical activity appeared enriched among patients with longer EV-free intervals:
- EVFI >12 months:
- ORR 33% (4/12)
- EVFI 6–12 months:
- ORR 31% (4/13)
- EVFI <6 months:
- ORR 0% (0/14)
Interestingly, 5 of 8 responders received EV2 at a reduced dose of 0.75 mg/kg, suggesting that rechallenge activity may still be preserved despite dose attenuation.
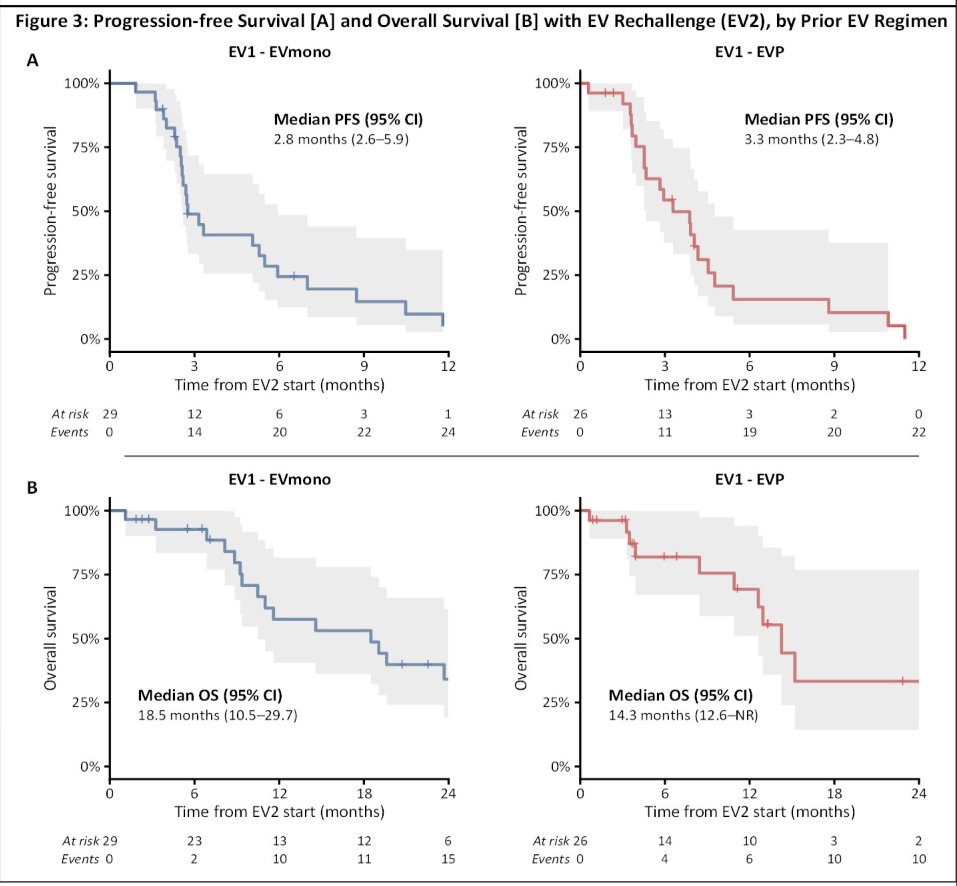
The survival outcomes from EV2 initiation were:
- Median PFS: 2.8 months
- Median OS: 18.5 months
- Median DoR among responders: 7.0 months (95% CI 3.5–NR)
At last follow-up:
- Three patients remained on EV rechallenge
- Thirty-nine patients discontinued EV2 due to:
- Disease progression: 74% (n=29)
- Toxicity: 23% (n=9)
- Patient preference: 2.6% (n=1)
Additional subgroup analyses demonstrated similar EV2 ORRs between patients initially treated with EV monotherapy versus EV + pembro:
- EV1 monotherapy cohort:
- EV2 ORR: 20%
- Median EV2 PFS: 2.7 months
- Median EV2 OS: 18.5 months
- EV + pembro cohort:
- EV2 ORR: 21%
- Median EV2 PFS: 4.1 months
- Median EV2 OS: 15.2 months
The investigators concluded that EV rechallenge demonstrated modest but clinically meaningful activity in a select subset of patients with metastatic urothelial carcinoma, particularly among those with a prior EV benefit and EV-free intervals exceeding 6 months. Importantly, no responses were observed among patients with primary EV resistance or rapid progression on prior EV therapy. These findings highlight the potential importance of treatment-free interval and prior response in selecting patients for EV rechallenge strategies. The authors emphasized that these observations are particularly relevant as efforts continue to mitigate EV toxicity and as recurrence following perioperative EV + pembro becomes an increasingly common clinical scenario.
Presented by: Michal Sternschuss, MD, Medical Oncologist, Memorial Sloan Kettering Cancer Center, New York, NY, USA
Written by: Rashid K. Sayyid, MD, MSc, Assistant Professor, Urologic Oncologist, Department of Urology at The University of Arizona and Banner University Medical Center, Tucson, AZ – @rksayyid on X during the American Society of Clinical Oncology Genitourinary (ASCO) Annual Meeting held in Chicago, IL between May 29th and June 1st, 2026
Reference: