(UroToday.com) The 2026 American Society of Clinical Oncology (ASCO) Annual Meeting was host to a kidney and bladder cancers oral abstract session. Dr. Andrea Apolo presented a discussant review entitled “Living Longer, Living Better: Can We Have It All?”, focusing on the rapidly evolving role of antibody-drug conjugates (ADCs) across the urothelial carcinoma disease continuum. Dr. Apolo synthesized findings from three presentations evaluating Nectin-4–targeted ADCs in muscle-invasive and metastatic urothelial carcinoma, while highlighting broader implications for treatment sequencing, toxicity, and future drug development.
The discussion centered on three key abstracts:
- Abstract 4506: Phase II perioperative SHR-A2102 plus adebrelimab in muscle-invasive bladder cancer (MIBC)
- Abstract 4507: Long-term outcomes with enfortumab vedotin (EV) plus pembrolizumab in metastatic urothelial carcinoma
- Abstract 4508: Activity of LY4052031 following prior EV exposure in metastatic urothelial carcinoma
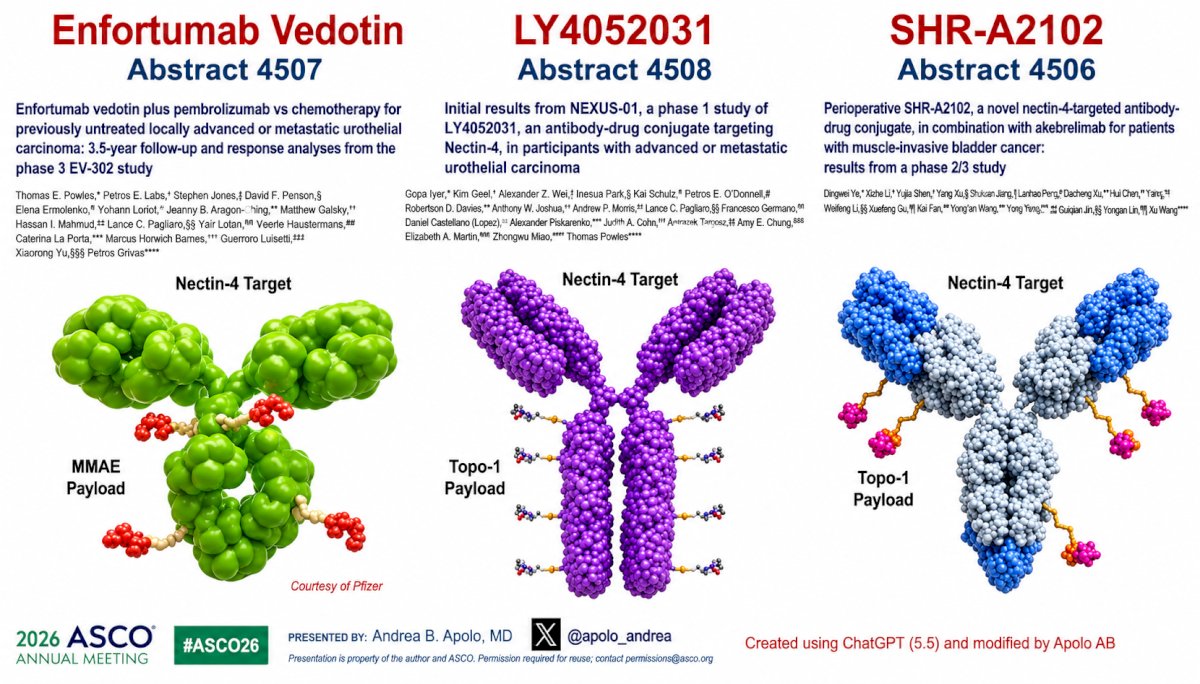
Nectin-4 is a membrane protein involved in cell-cell adhesion that is highly expressed across numerous solid tumors, including urothelial carcinoma. Beyond serving as a marker of tumor biology, Nectin-4 contributes to tumor proliferation, differentiation, migration, and invasion, making it an attractive therapeutic target for ADC development.
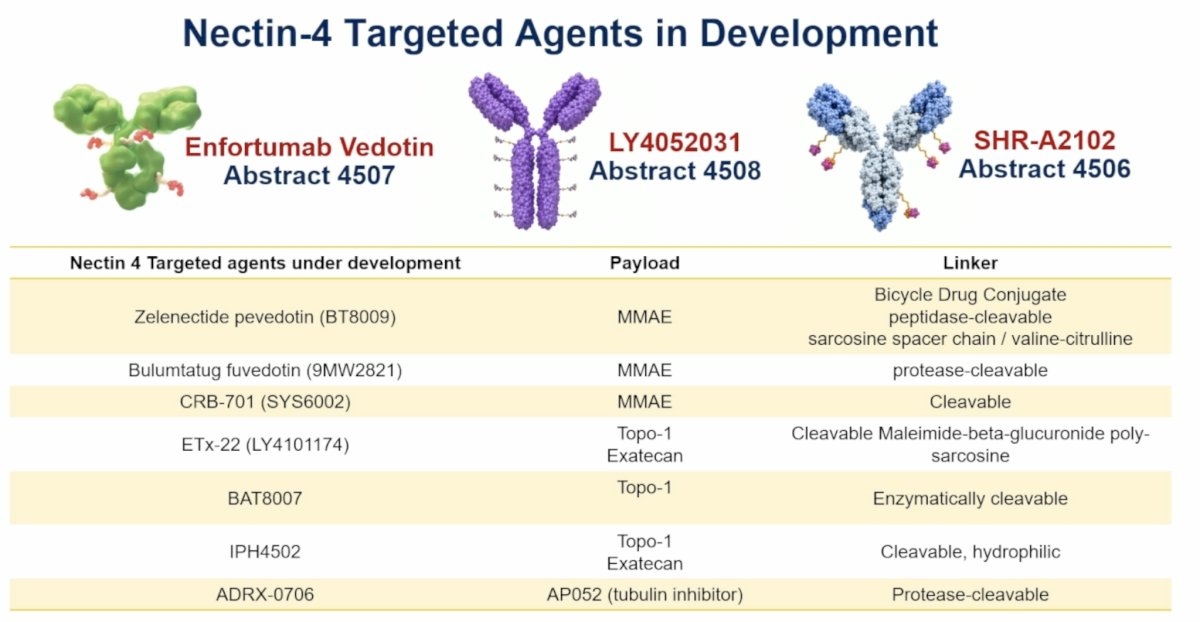
She highlighted that all three abstracts presented during the session target Nectin-4 but employ distinct ADC designs and clinical strategies:
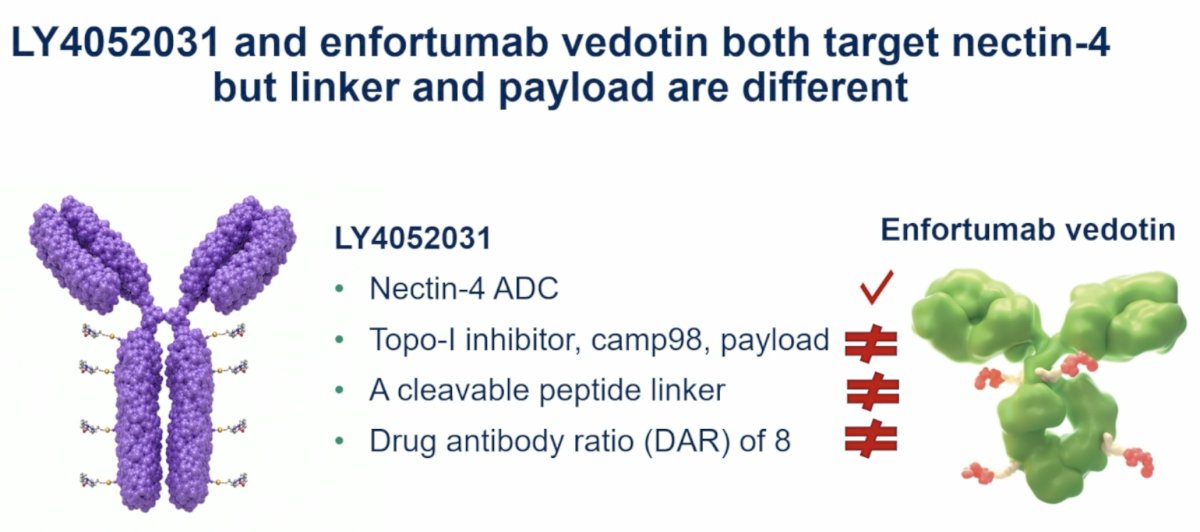
- Enfortumab vedotin utilizes a monomethyl auristatin E (MMAE) payload
- LY4052031 incorporates a Topo-1 inhibitor (camptothecin analog) payload with a cleavable peptide linker and a drug-to-antibody ratio of 8
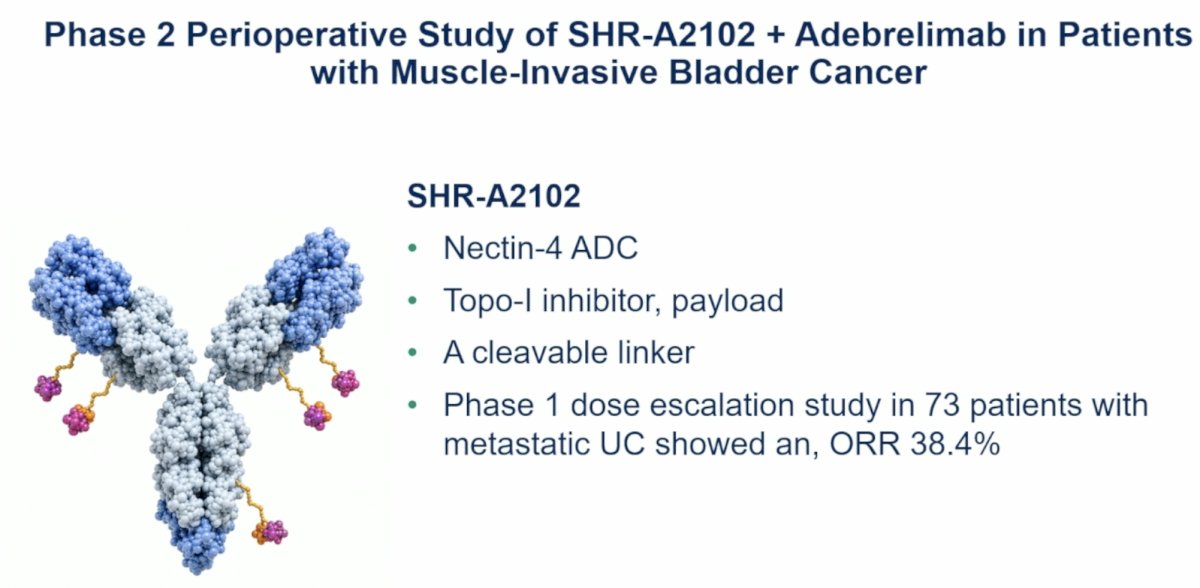
- SHR-A2102 is also a Nectin-4 ADC utilizing a Topo-1 inhibitor payload with a cleavable linker
Long-Term Follow-up of EV-302 Reinforces EV + Pembrolizumab as Standard of Care
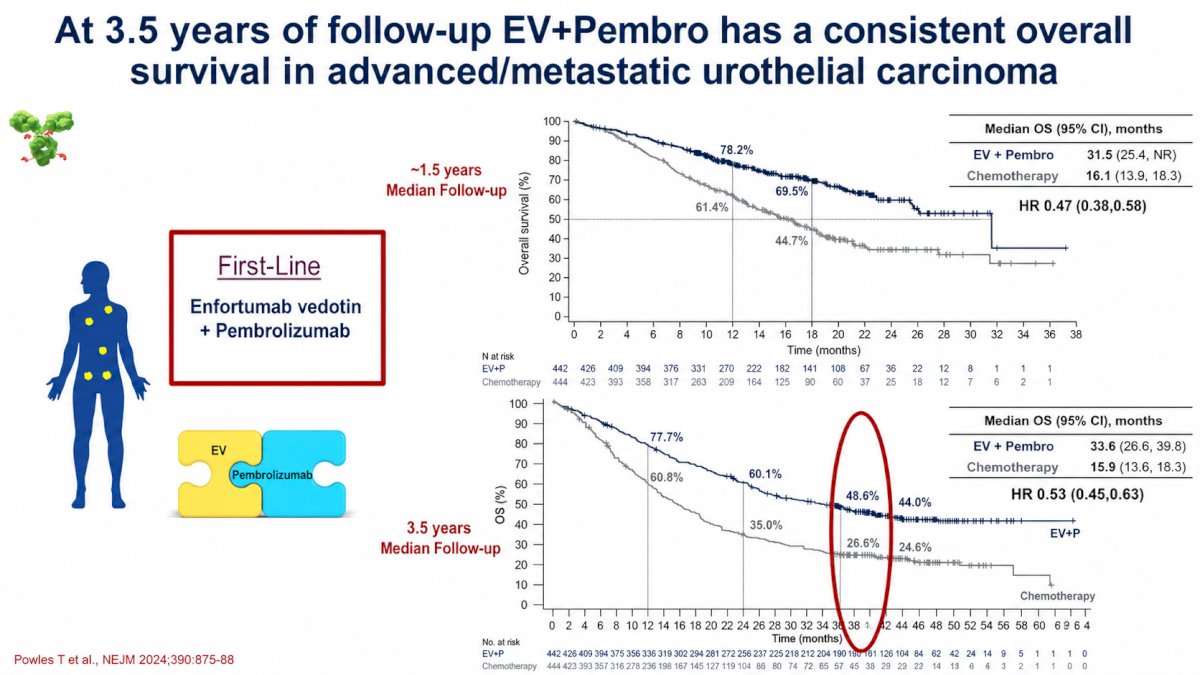
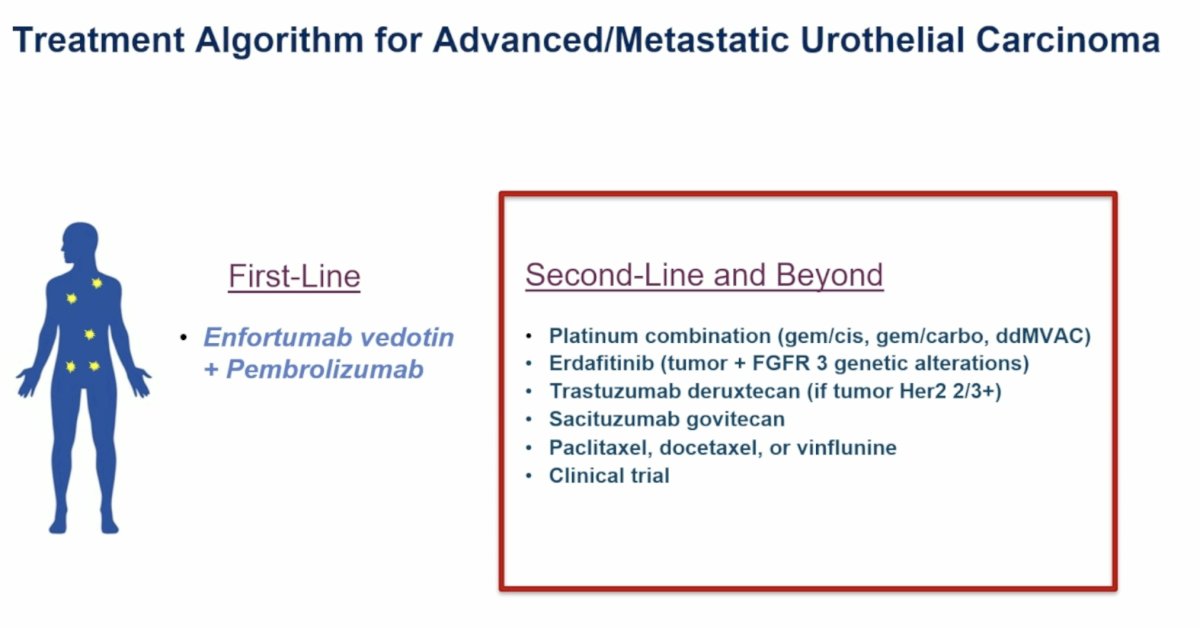
Dr. Apolo reviewed the evolution of the treatment paradigm in advanced urothelial carcinoma, noting that EV-302 established enfortumab vedotin plus pembrolizumab as the standard first-line therapy for patients with locally advanced or metastatic disease.1
With approximately 3.5 years of follow-up now available from EV-302, the survival advantage of EV plus pembrolizumab remains durable. Median overall survival was 33.8 months with EV plus pembrolizumab versus 15.9 months with platinum-based chemotherapy (HR 0.51), representing an approximately 18-month improvement in median survival.
Dr. Apolo emphasized that these long-term results confirm the durability of benefit and reinforce EV plus pembrolizumab as the preferred frontline standard of care in metastatic urothelial carcinoma.
One of the most notable findings discussed was the depth and durability of complete responses. Among 437 patients treated with EV plus pembrolizumab:
- 295 patients (67.5%) achieved an objective response
- 133 patients (30.4%) achieved a complete response
- 162 patients (37.1%) achieved a partial response
Importantly, Dr. Apolo highlighted that a substantial proportion of complete responders initially achieved a partial response before subsequently converting to a complete response during continued therapy.
Patients who converted from partial response to complete response demonstrated remarkably favorable long-term outcomes, with overall survival exceeding 80% at 3.5 years, comparable to patients who achieved an initial complete response. These findings suggest that continued treatment can deepen responses over time and that patients achieving a partial response should not necessarily be viewed as having reached their maximal benefit.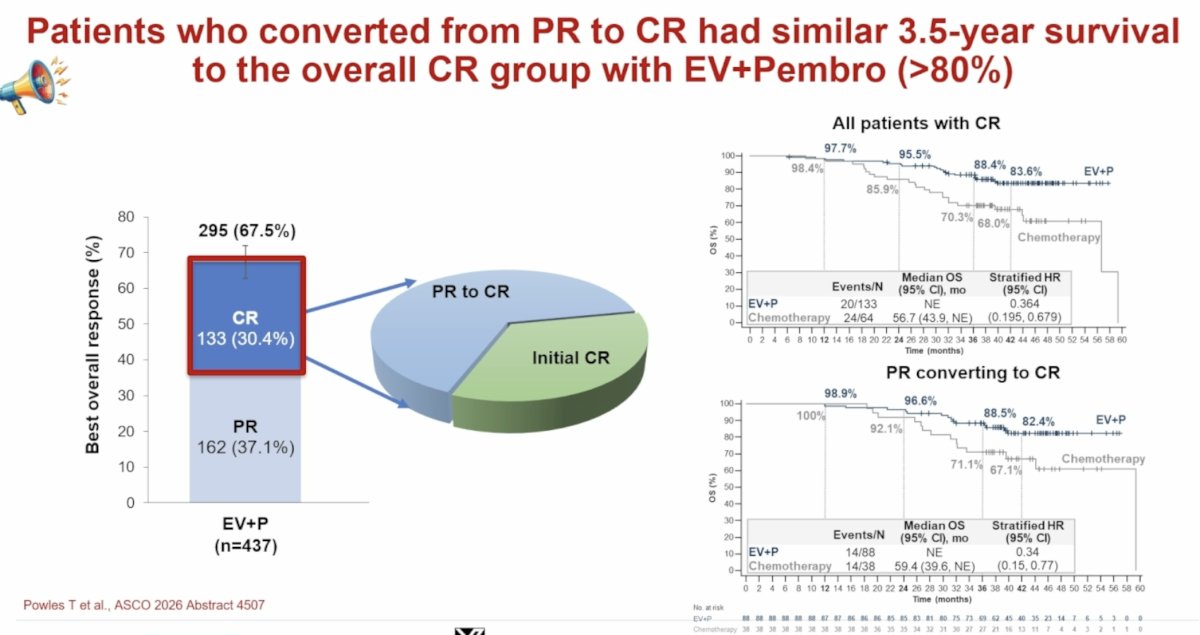
Duration of Therapy Remains an Important Unanswered Question
While emphasizing the success of EV plus pembrolizumab, Dr. Apolo also identified treatment duration as an important unresolved issue.
She noted that among EV-treated patients:
- 42% remained on therapy for at least 1 year
- 23% remained on therapy for at least 2 years
- Median EV duration reached 22.3 months among those treated for ≥2 years
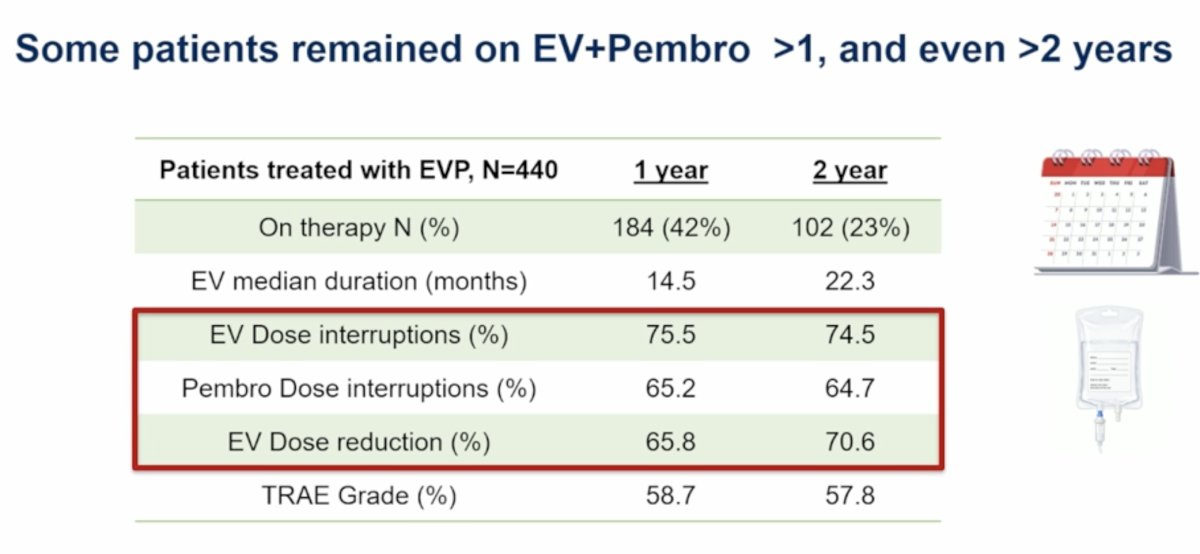
Long-term treatment was associated with frequent dose modifications:
- EV dose interruptions occurred in approximately 75%
- Pembrolizumab interruptions occurred in approximately 65%
- EV dose reductions occurred in approximately 70%
- These observations raised several clinically important questions:
- Do patients need to remain on EV for prolonged periods to maintain benefit?
- Can biomarkers such as circulating tumor DNA identify patients who can safely discontinue therapy?
- What is the optimal treatment duration for patients achieving complete responses?
To address these questions, Dr. Apolo highlighted the ongoing phase 2 IMPROVE study. This trial enrolls patients with locally advanced or metastatic urothelial carcinoma and administers six cycles of induction EV plus pembrolizumab. Patients achieving CR or PR transition to pembrolizumab maintenance for up to two years, while EV may be reintroduced upon progression. The primary endpoint is 18-month progression-free survival.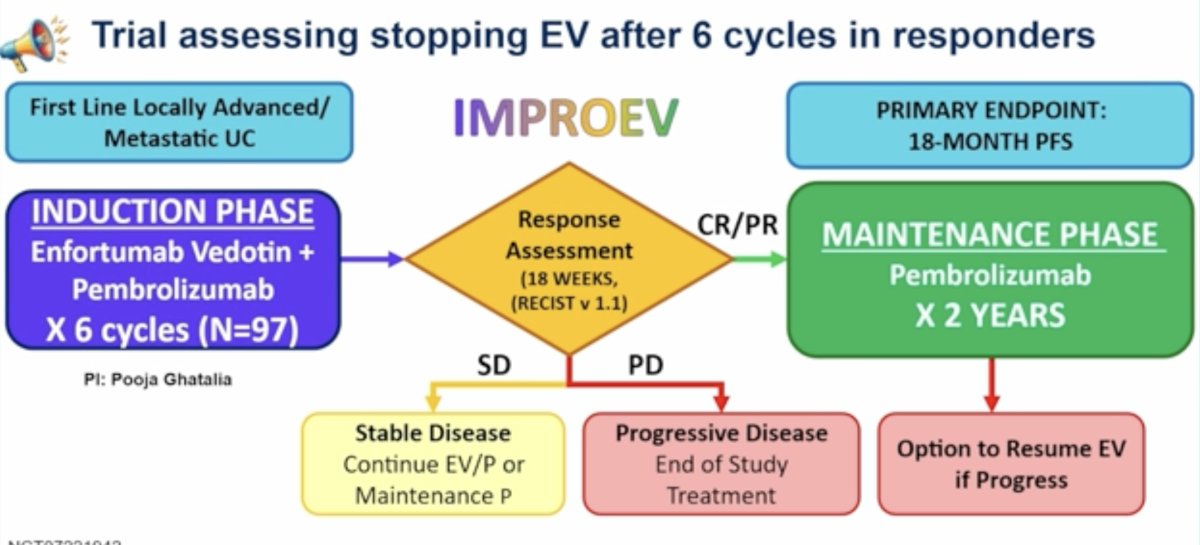
Activity of LY4052031 Following Enfortumab Vedotin
Dr. Apolo next discussed LY4052031, a novel Nectin-4–targeted ADC utilizing a Topo-1 inhibitor payload.. Although LY4052031 targets the same antigen as enfortumab vedotin, important mechanistic differences exist. Compared with EV, LY4052031 employs:
- A distinct Topo-1 inhibitor payload
- A different linker technology
- A higher drug-to-antibody ratio
A major challenge during early development involved treatment-related toxicity associated with reduced CYP2D6 activity. Three early deaths prompted prospective CYP2D6 genotyping, which subsequently became integrated into study enrollment. Patients with low CYP2D6 activity scores demonstrated increased risks of mucositis, febrile neutropenia, and sepsis.
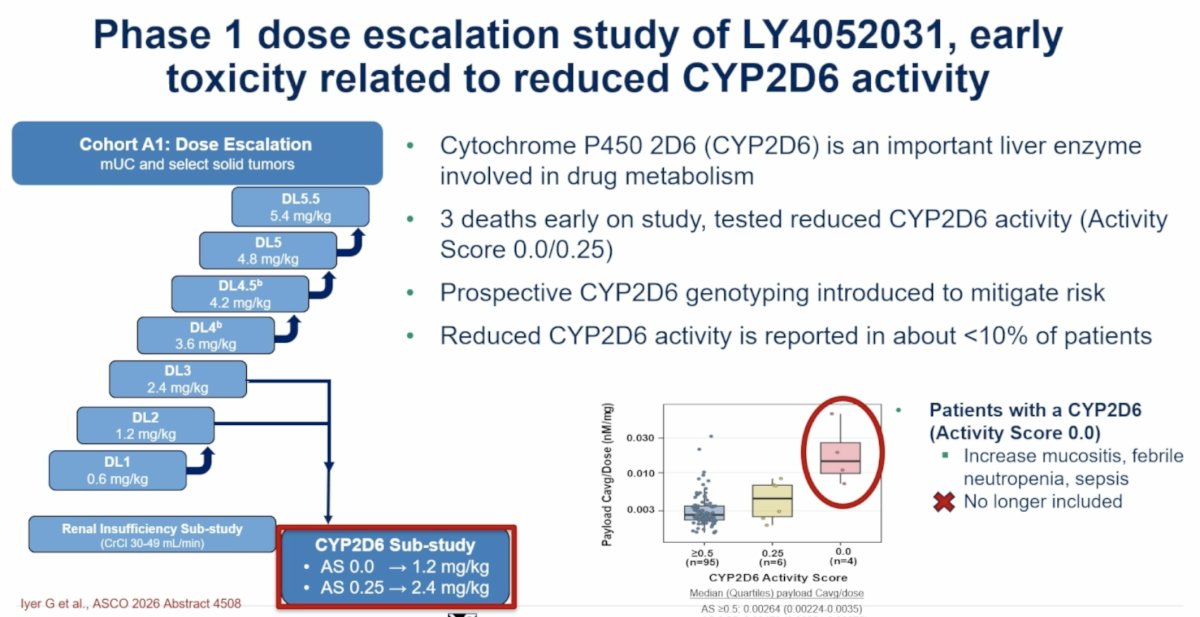
Dr. Apolo emphasized that future development of LY4052031 requires germline CYP2D6 testing to exclude patients with low activity scores.
Among 107 patients with metastatic urothelial carcinoma treated during dose escalation:
- 72 had received prior EV
- 42 had received EV plus pembrolizumab
- 99 had received prior immunotherapy
- 25 had received prior Topo-1–based therapy
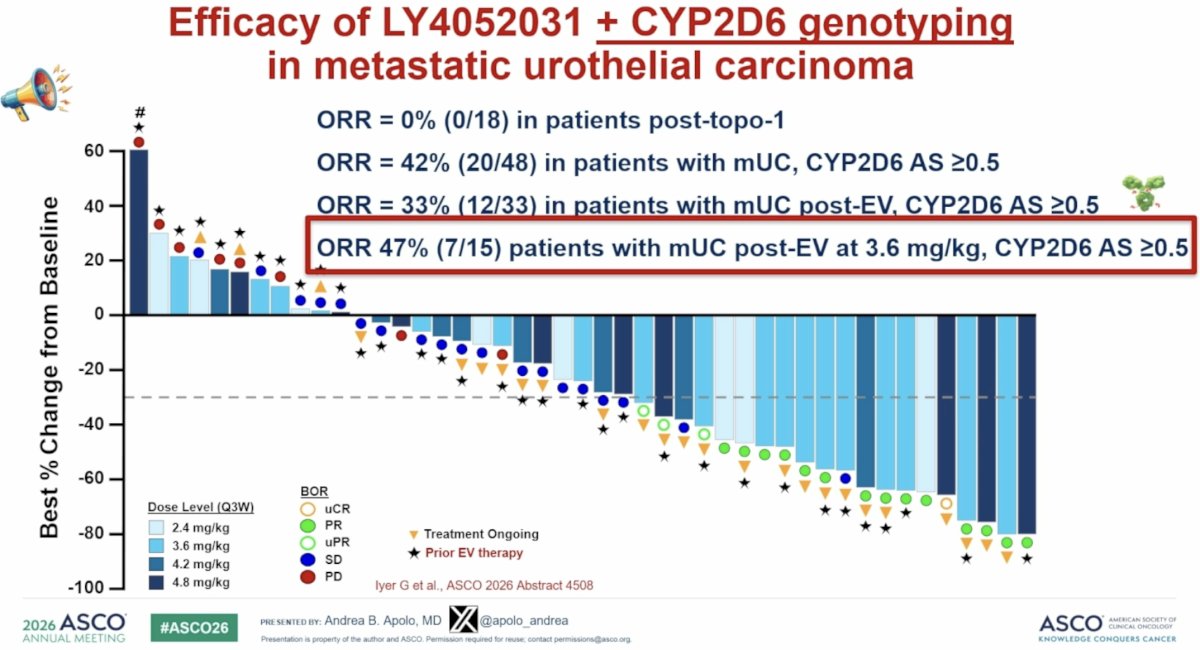
One of the most clinically important findings was the observation that LY4052031 retained activity following prior EV exposure. Among patients with metastatic urothelial carcinoma and prior EV treatment who received LY4052031 at 3.6 mg/kg and had CYP2D6 activity scores ≥0.5, the objective response rate reached 47% (7/15 patients).
In contrast, no responses were observed among patients previously exposed to Topo-1 ADCs.
Dr. Apolo framed these findings within the broader biology of ADC resistance. Potential mechanisms include:
- Antigen loss or impaired internalization
- Payload efflux or clearance
- Target alterations
- Anti-apoptotic signaling pathways
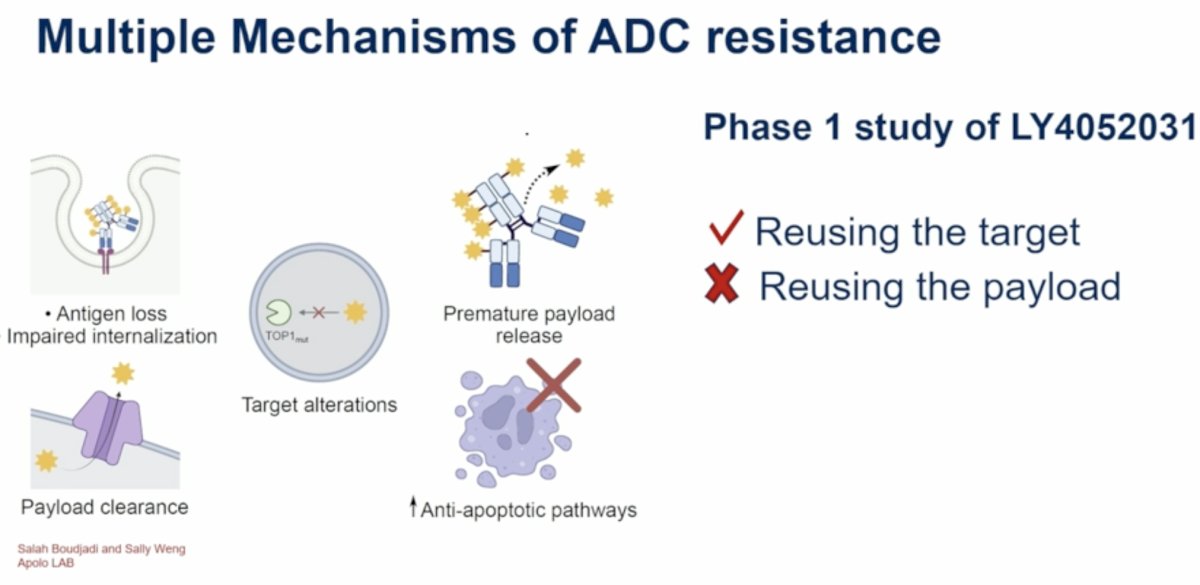
The LY4052031 results suggest that resistance may not necessarily occur at the level of Nectin-4 itself. Rather, patients may remain sensitive to continued targeting of Nectin-4, provided a different payload is employed.
She summarized this concept succinctly as “reusing the target but not reusing the payload.”
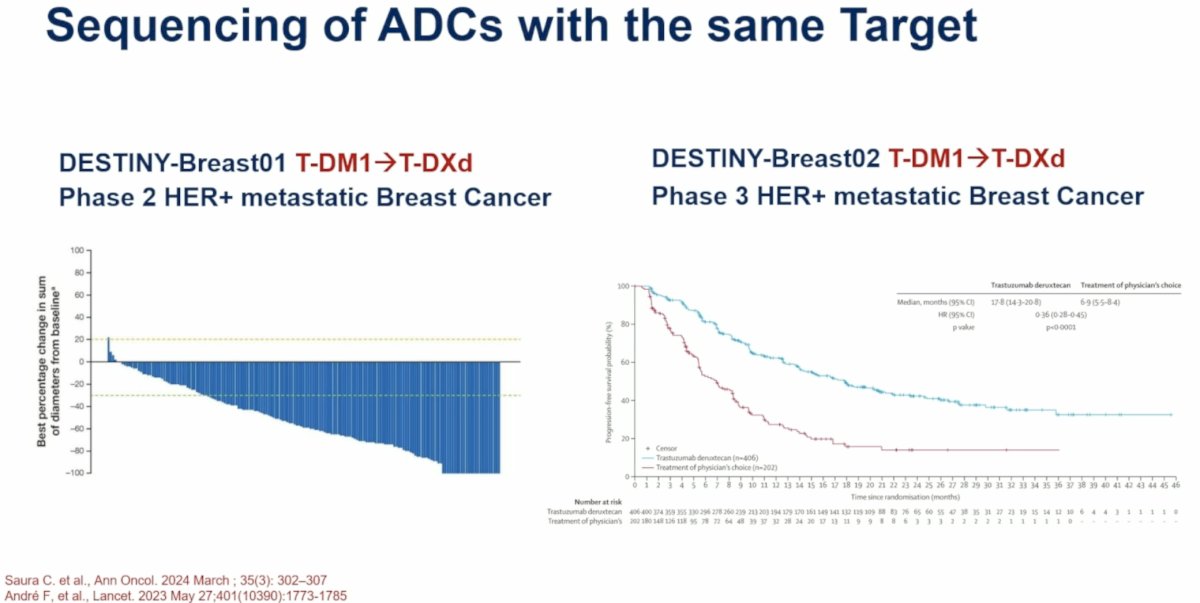
To support this concept, Dr. Apolo referenced the DESTINY-Breast studies, which demonstrated meaningful activity when trastuzumab deruxtecan was administered after prior HER2-directed ADC exposure in breast cancer. These data provide a precedent for sequential ADC therapy directed against the same antigen.
Early Perioperative Activity of SHR-A2102 Plus Adebrelimab in Muscle-Invasive Bladder Cancer
Dr. Apolo concluded by discussing SHR-A2102, a Nectin-4–targeted ADC with a Topo-1 inhibitor payload evaluated in combination with the PD-L1 inhibitor adebrelimab in muscle-invasive bladder cancer.
The phase 2 perioperative study enrolled 37 patients with MIBC and creatinine clearance ≥30 mL/min. Patients received:
- Four cycles of neoadjuvant SHR-A2102 plus adebrelimab every three weeks
- Radical cystectomy
- Five cycles of adjuvant SHR-A2102 and thirteen cycles of adebrelimab
The primary endpoints were pathologic complete response and selection of the recommended phase 3 dose.
Dr. Apolo placed these results in the context of ongoing perioperative Nectin-4–directed studies, including EV-304/KEYNOTE-B15, EV-303/KEYNOTE-905, and VOLGA.
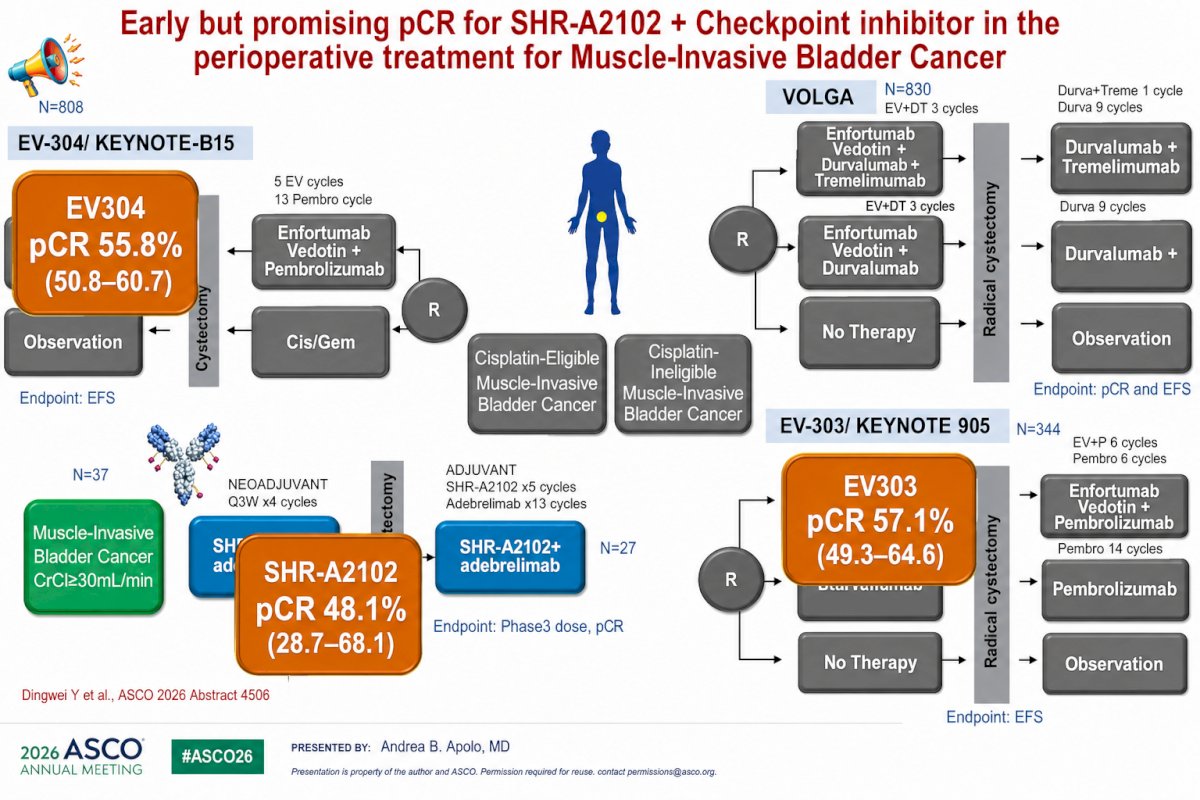
The observed pCR rate of 48.1% (95% CI: 28.7–68.1) compared favorably with rates reported in contemporary perioperative EV-based studies:
- EV-304/KEYNOTE-B15: 55.8%
- EV-303/KEYNOTE-905: 57.1%
Although acknowledging the limitations of cross-trial comparisons and the small sample size, Dr. Apolo described the results as encouraging and supportive of continued development.
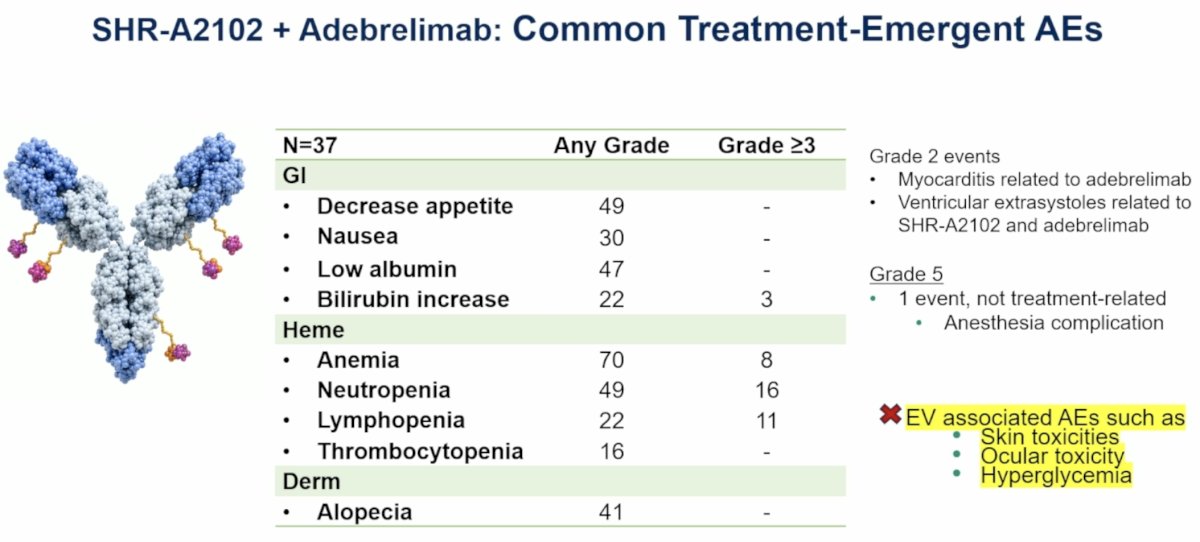
Safety appeared distinct from that typically observed with enfortumab vedotin. Common adverse events included:
- Anemia (70%)
- Neutropenia (49%)
- Decreased appetite (49%)
- Low albumin (47%)
- Alopecia (41%)
- Nausea (30%)
Importantly, adverse events commonly associated with EV—including skin toxicity, ocular toxicity, and hyperglycemia—were not prominent. Two grade 2 cardiac events were reported, including myocarditis attributed to adebrelimab and ventricular extrasystoles attributed to the combination. One grade 5 anesthesia-related complication was considered unrelated to treatment.
Dr. Apolo noted that a phase 3 study is currently being developed and may provide important opportunities for biomarker discovery and future bladder-preservation strategies.
Dr. Apolo concluded by integrating these findings into the evolving urothelial carcinoma treatment landscape. For metastatic disease, EV plus pembrolizumab remains the established first-line standard based on durable survival improvements and long-term complete responses.
For patients progressing after frontline therapy, an expanding group of targeted therapies remains available, including:
- Erdafitinib for FGFR3-altered tumors
- Trastuzumab deruxtecan for HER2-positive disease
- Sacituzumab govitecan
- Chemotherapy options
- Clinical trials
The LY4052031 data suggest that Nectin-4 remains a valid therapeutic target even after EV exposure, provided alternative payloads are utilized. Meanwhile, SHR-A2102 demonstrates the potential to move Nectin-4–directed ADC therapy earlier into the disease course in muscle-invasive bladder cancer.
Dr. Apolo summarized the session with three principal take-home messages:
- Enfortumab vedotin continues to deliver durable overall survival benefits and remains the standard first-line therapy for metastatic urothelial carcinoma.
- LY4052031 demonstrates meaningful activity following prior EV exposure, supporting continued development of sequential Nectin-4–targeted ADC strategies.
- SHR-A2102 plus adebrelimab demonstrates encouraging perioperative activity in muscle-invasive bladder cancer and warrants further evaluation in phase 3 testing.
Presented by: Andrea B. Apolo, MD, Chief, Bladder Cancer Section, Genitourinary Malignancies Branch, Center for Cancer Research, National Cancer Institute, Bethesda, MD
Written by: Rashid K. Sayyid, MD, MSc, Assistant Professor, Urologic Oncologist, Department of Urology at The University of Arizona and Banner University Medical Center, Tucson, AZ – @rksayyid on X during the American Society of Clinical Oncology Genitourinary (ASCO) Annual Meeting held in Chicago, IL between May 29th and June 1st, 2026
References: