(UroToday.com) The 2026 American Society of Clinical Oncology (ASCO) Annual Meeting was host to a State-of-the-Art session on advances in the perioperative management of bladder and kidney cancers. Dr. C.K. Cornelia Ding presented a state-of-the-art review entitled “Clinical Applications of Pathologic Biomarkers in Genitourinary Cancers,” highlighting both established and emerging pathology biomarkers across genitourinary malignancies, with a particular focus on the integration of artificial intelligence-driven pathology tools into clinical practice.
Dr. Ding began by outlining three key principles that clinicians should keep in mind when utilizing pathology biomarkers in GU oncology:
- There is no single perfect assay for common biomarkers, and clinicians must understand the strengths and limitations of each testing modality.
- Many biomarker assays are not standardized across laboratories, creating variability in interpretation and performance.
- Close collaboration with pathologists is essential to assess tissue quantity and quality and to prioritize biomarkers most relevant to clinical decision-making.
Dr. Ding first reviewed MSI-H/dMMR tumors. Microsatellite instability arises from defects in DNA mismatch repair proteins (MLH1, PMS2, MSH2, and MSH6), leading to instability within short tandem repeat DNA sequences. These tumors are clinically relevant because immune checkpoint inhibitors are approved for patients with unresectable or metastatic MSI-H/dMMR solid tumors.
Within GU malignancies, MSI-H/dMMR prevalence varies by disease type:
- Prostate cancer: 3–12%
- Upper tract urothelial carcinoma: 3–11%
- Bladder urothelial carcinoma: 1–3%
- Renal cell carcinoma: ~1%
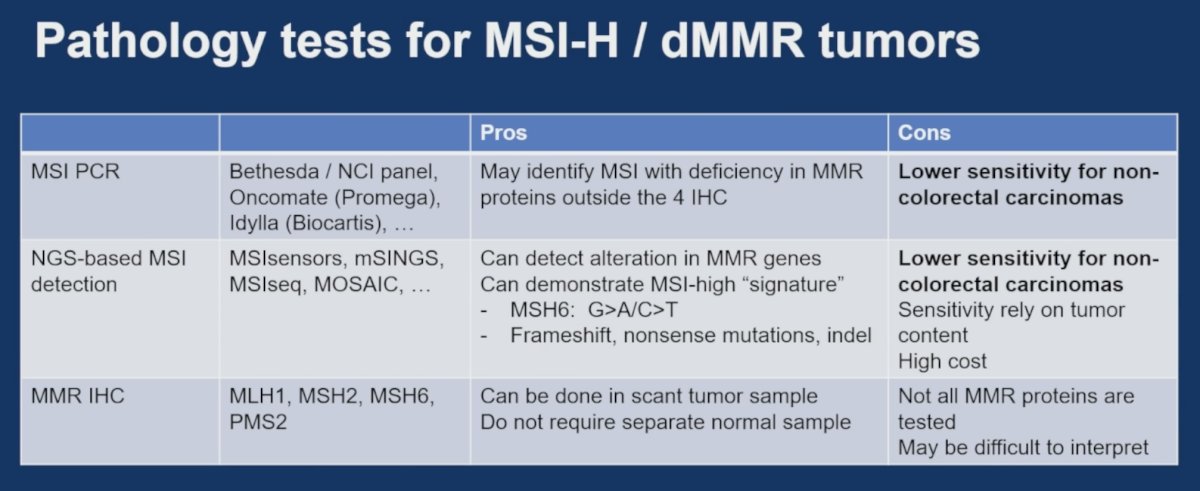
Dr. Ding reviewed the currently available pathology testing approaches for MSI-H/dMMR assessment:
- MSI PCR assays (Bethesda/NCI panel, Oncomate, Idylla) may identify MSI resulting from MMR deficiencies beyond the four proteins routinely evaluated by IHC, although sensitivity is lower in non-colorectal malignancies.
- NGS-based MSI detection platforms (MSIsensors, mSINGS, MSIseq, MOSAIC) can detect MMR gene alterations, MSI-high mutational signatures, and associated frameshift, nonsense, and indel mutations. However, these assays are dependent on tumor content, are more costly, and also demonstrate lower sensitivity in non-colorectal tumors.
- MMR immunohistochemistry evaluates MLH1, MSH2, MSH6, and PMS2 expression and offers several practical advantages, including use on scant tumor samples and elimination of the need for a matched normal specimen. Limitations include incomplete assessment of all MMR abnormalities and challenges in interpretation.
To illustrate these challenges, Dr. Ding presented examples of MSH6 staining in prostate cancers with validated MSH2 loss and MSI-high status across four institutions. Marked variability in staining intensity and patterns was observed, with some cases appearing equivocal and others demonstrating minimal staining of non-tumor tissue, underscoring the potential difficulties associated with interpretation.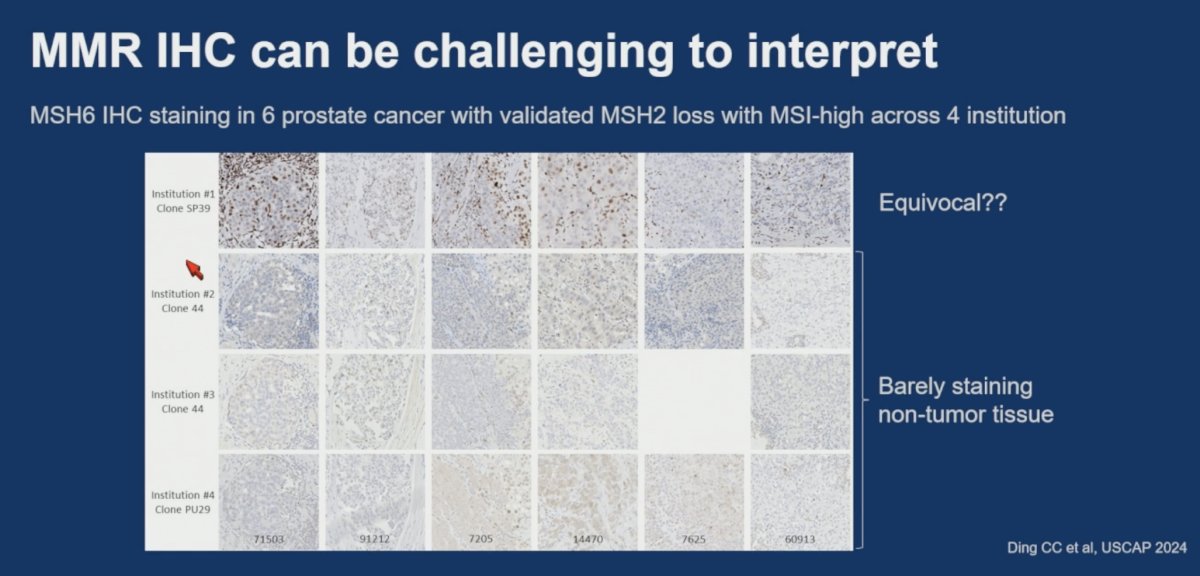
Dr. Ding concluded that no single test is ideal. For patients with limited tissue, MMR IHC may be preferred, whereas those with strong clinical suspicion may benefit from more than one testing modality.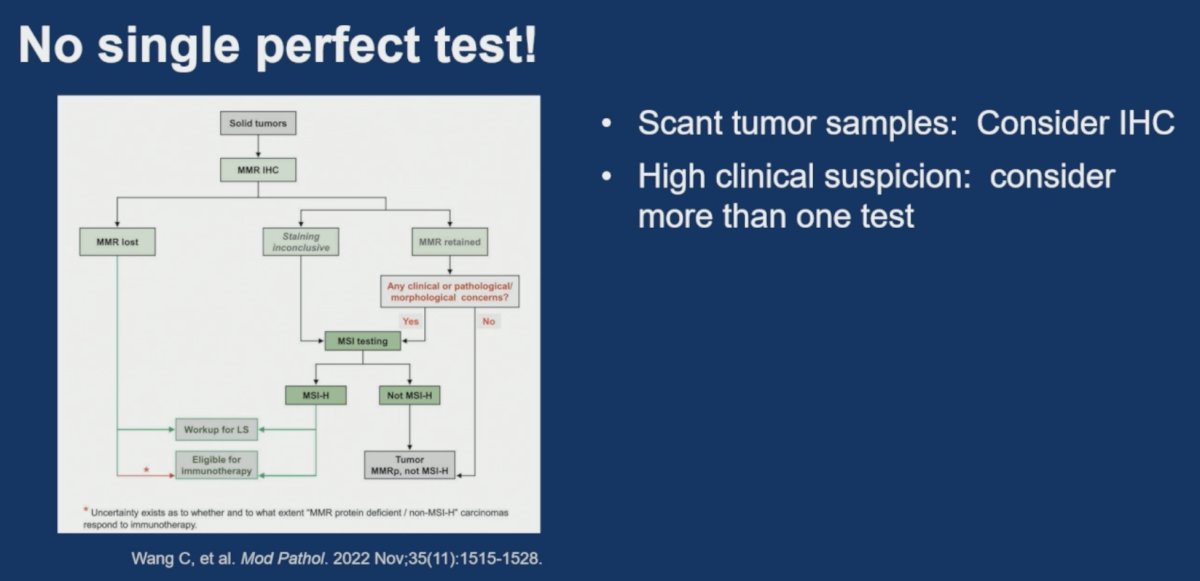
HER2 (ERBB2)
Dr. Ding next discussed HER2, which has become increasingly relevant following tissue-agnostic approval of trastuzumab deruxtecan (T-DXd) for advanced HER2-positive solid tumors. Additional HER2-directed antibody-drug conjugates, including trastuzumab emtansine and disitamab vedotin, continue to expand the therapeutic landscape.
HER2 testing is most commonly performed by immunohistochemistry. Current clinical trial approaches have utilized gastroesophageal cancer scoring criteria in DESTINY-PanTumor and breast cancer scoring criteria in other studies.
Among patients with advanced or metastatic urothelial carcinoma:
- HER2 IHC 3+ expression is present in approximately 13.2%
- HER2 gene amplification by in situ hybridization is observed in 56.2% of HER2 IHC 3+ tumors
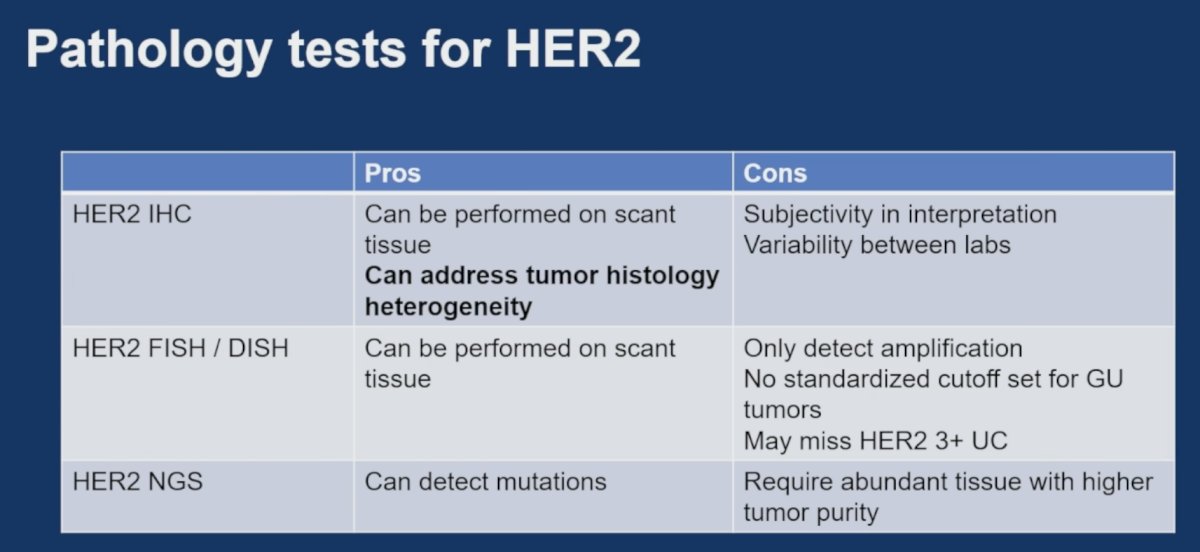
Dr. Ding reviewed the strengths and weaknesses of available HER2 testing platforms.
- HER2 IHC offers the advantages of requiring minimal tissue and capturing tumor histologic heterogeneity. Limitations include subjective interpretation and inter-laboratory variability
- HER2 FISH/DISH similarly performs well on limited tissue samples but detects amplification only, lacks standardized GU-specific cutoffs, and may miss HER2-positive urothelial cancers identified by IHC
- HER2 NGS can identify HER2 mutations, but requires more abundant tissue and higher tumor purity
Importantly, Dr. Ding highlighted the issue of intratumoral heterogeneity. She presented a urothelial carcinoma specimen containing both small-cell carcinoma and high-grade papillary urothelial carcinoma components that demonstrated markedly different HER2 expression patterns despite shared underlying genomic alterations. These findings emphasize the importance of morphology-aware biomarker assessment and careful pathologic review.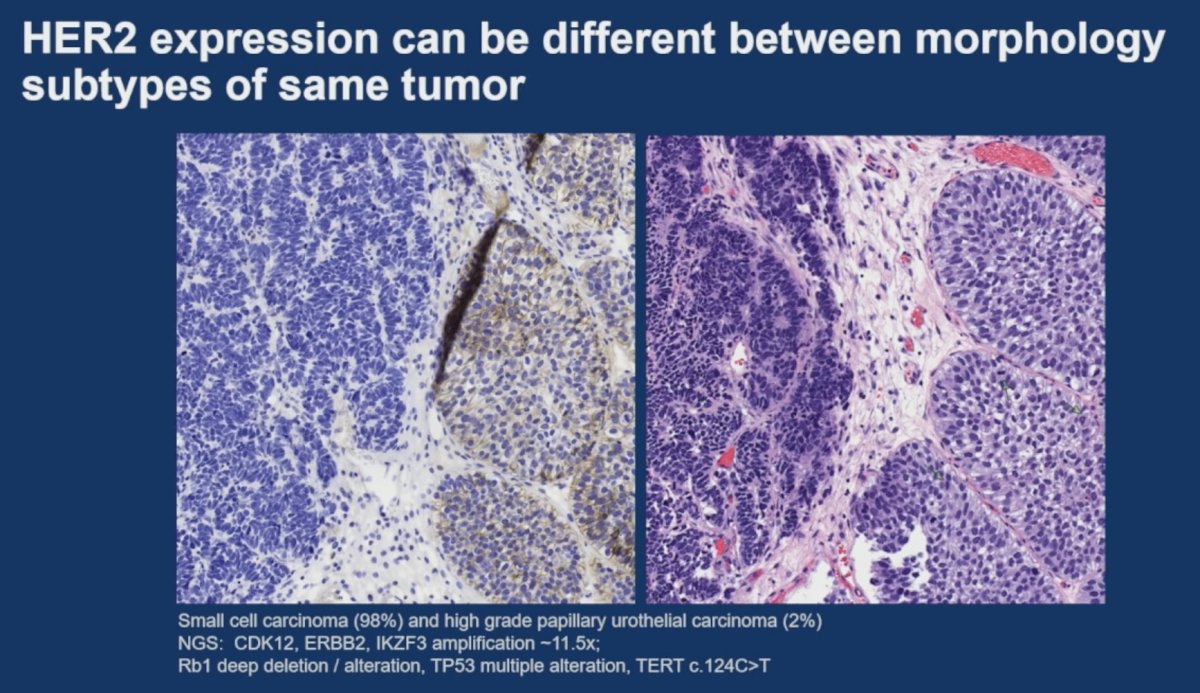
Emerging Biomarkers
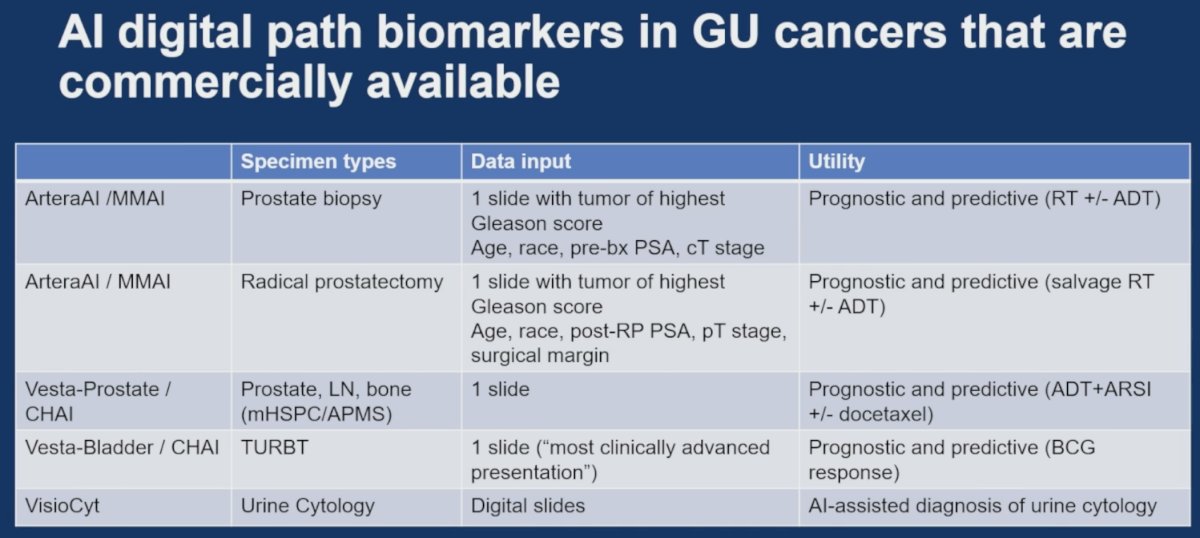
Dr. Ding then turned to AI-enabled digital pathology biomarkers that are now commercially available in GU oncology.
Examples include:
- ArteraAI/MMAI
- Uses prostate biopsy specimens
- Uses a single slide containing the highest Gleason score tumor, together with clinical variables
- Provides prognostic and predictive information for radiotherapy ± ADT
- ArteraAI/MMAI (post-prostatectomy)
- Utilizes a slide containing the highest Gleason score tumor, together with postoperative clinical variables
- Provides prognostic and predictive information regarding salvage radiotherapy ± ADT
- Vesta-Prostate/CHAI
- Applied to prostate, lymph node, and bone specimens in mHSPC/APMSC
- Generates prognostic and predictive information regarding ADT, ARSI, and docetaxel therapy
- Vesta-Bladder/CHAI
- Applied to TURBT specimens
- Provides prognostic and predictive information regarding BCG response
- VisioCyt
- Uses digital urine cytology slides
- Provides AI-assisted urine cytology interpretation
Dr. Ding noted several advantages of AI pathology biomarkers:
- No additional tissue consumption
- Ability to leverage routinely acquired pathology slides
However, several limitations remain:
- Variable strength of supporting evidence across platforms
- Limited explainability for many AI algorithms
- Dependence on the pathologist's expertise and appropriate slide selection
She emphasized that identifying the “best slides” still depends heavily on pathologist grading, diagnostic expertise, and communication between clinicians and pathologists.
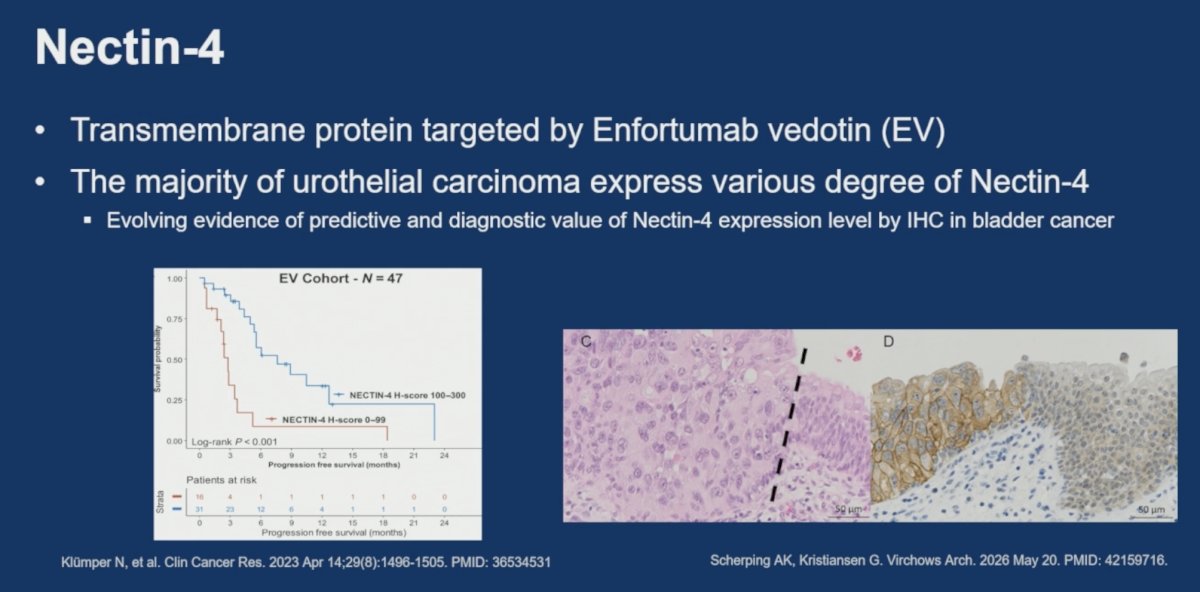
Nectin-4Dr. Ding next reviewed Nectin-4, a transmembrane protein targeted by enfortumab vedotin. The majority of urothelial carcinomas express Nectin-4 to varying degrees, and emerging evidence suggests that Nectin-4 expression may possess both predictive and diagnostic value.
She highlighted data demonstrating improved progression-free survival among patients receiving enfortumab vedotin whose tumors exhibited high Nectin-4 H-scores (100–300) compared to lower expression levels (0–99), supporting a potential predictive role for Nectin-4 assessment. Additional studies have also demonstrated substantial heterogeneity of Nectin-4 expression within tumors.
Clear Cell RCC Pathology Biomarkers
Dr. Ding then discussed pathology biomarkers for clear cell RCC. Histologic growth patterns have emerged as important prognostic biomarkers, with morphology-based risk groups demonstrating distinct overall survival outcomes.
She additionally reviewed loss of BAP1 expression by immunohistochemistry, which has consistently been associated with adverse prognosis and inferior overall survival compared to tumors retaining BAP1 expression.
These findings reinforce the ongoing importance of traditional pathology assessment alongside molecular biomarker development.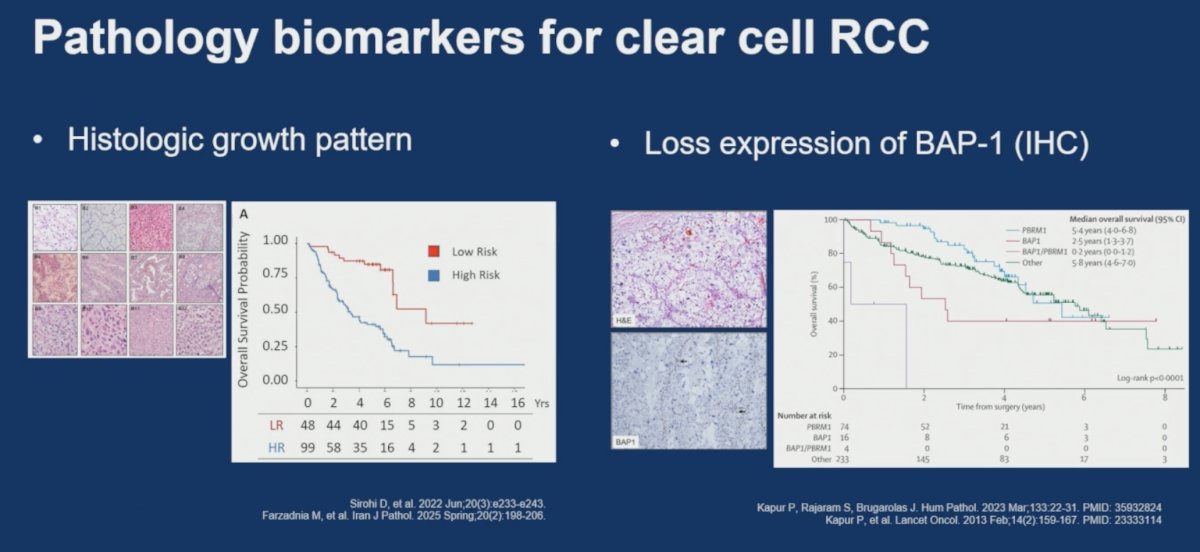
Circulating KIM-1
Finally, Dr. Ding discussed circulating kidney injury molecule-1 (KIM-1) as an emerging blood-based biomarker in RCC.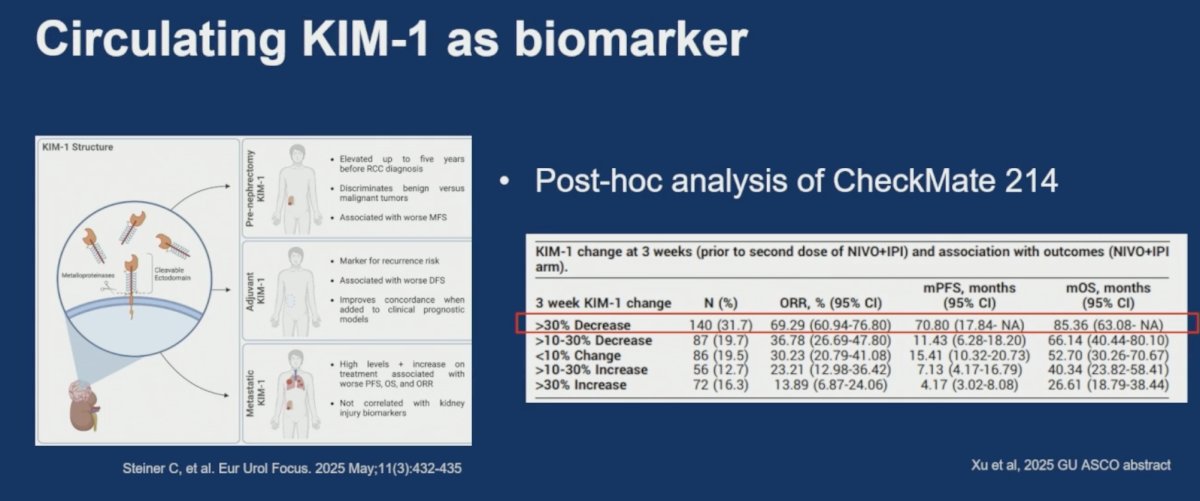
KIM-1 levels may be elevated years before RCC diagnosis, discriminate malignant from benign renal tumors, and are associated with recurrence risk. KIM-1 has also demonstrated promise as a dynamic treatment-response biomarker.
She highlighted a post-hoc analysis of CheckMate 214 evaluating early changes in KIM-1 among patients receiving nivolumab plus ipilimumab. Patients with >30% decreases in circulating KIM-1 at three weeks experienced the most favorable outcomes:
- ORR: 69.29% (95% CI: 60.94–76.80)
- Median PFS: 70.80 months (95% CI: 17.84–NA)
- Median OS: 85.36 months (95% CI: 63.08–NA)
Conversely, increasing KIM-1 levels were associated with progressively worse clinical outcomes.
Dr. Ding concluded by reiterating three key messages:
- There is no one perfect assay for commonly used pathology biomarkers.
- Many biomarker assays remain insufficiently standardized across laboratories, necessitating an understanding of assay-specific strengths and limitations.
- Clinicians should work closely with pathologists to optimize tissue utilization, ensure adequate specimen quality, and prioritize biomarkers that directly inform clinical management.
Emerging biomarkers—including AI-driven digital pathology platforms, Nectin-4 expression, morphology-based RCC biomarkers, and circulating KIM-1—have the potential to further expand the role of pathology in precision GU oncology.
Presented by: Chien-Kuang Cornelia Ding, MD, PhD, Assistant Professor, Department of Pathology, University of California, San Francisco, CA, USA
Written by: Rashid K. Sayyid, MD, MSc, Assistant Professor, Urologic Oncologist, Department of Urology at The University of Arizona and Banner University Medical Center, Tucson, AZ – @rksayyid on X during the American Society of Clinical Oncology Genitourinary (ASCO) Annual Meeting held in Chicago, IL between May 29th and June 1st, 2026