(UroToday.com) The 2026 American Society of Clinical Oncology (ASCO) Annual Meeting was host to a session on new approaches to curing bladder and kidney cancer. Dr. Brian Rini delivered a discussant presentation entitled “Living Longer, Living Better: Can We Have It All?”, synthesizing the four prior presentations spanning muscle-invasive bladder cancer (MIBC) and renal cell carcinoma (RCC):
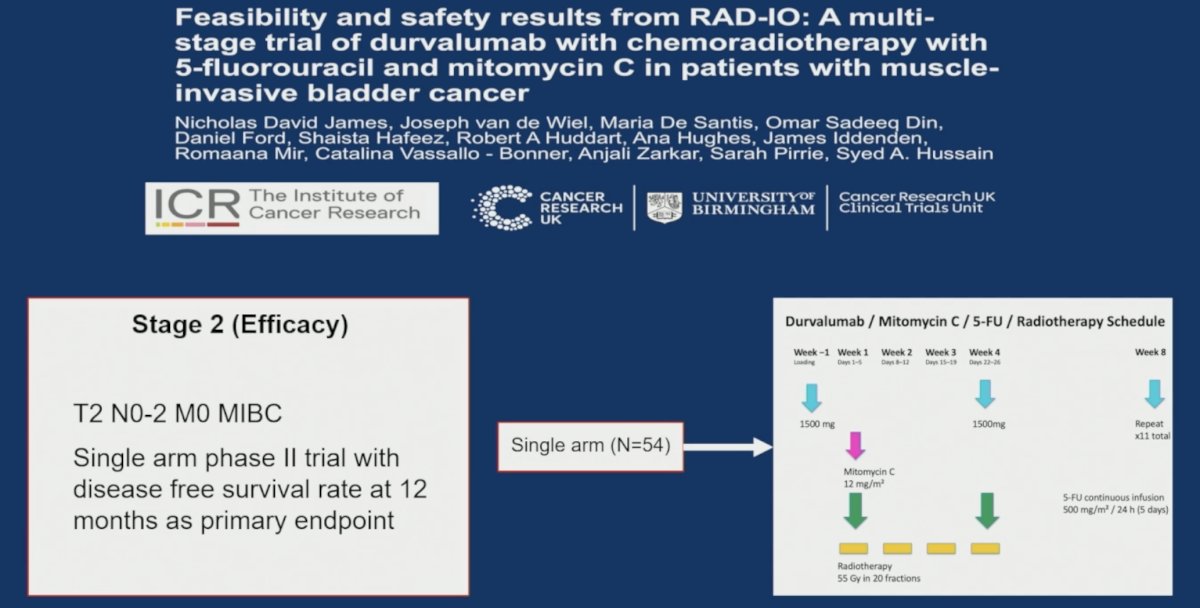
- Feasibility and safety results from RAD-IO: A multi-stage trial of durvalumab with chemoradiotherapy with 5-FU and mitomycin C in patients with MIBC
- Durvalumab monotherapy versus active monitoring for resected primary RCC in RAMPART: An international, phase 3, randomized controlled trial
- HRQoL with neoadjuvant and adjuvant EV + Pembro in patients with MIBC who are cisplatin-ineligible: Phase 3 KEYNOTE-905 Study
- Decision regret and toxicity perception following adjuvant immune checkpoint inhibitor in renal cell carcinoma
Rather than focusing on individual trial results in isolation, Dr. Rini framed the discussion around three central questions facing modern peri-operative genitourinary oncology: how best to integrate local and systemic therapies in the era of highly active immunotherapy-based regimens, whether treatment intensification strategies are truly improving outcomes, and how clinicians should measure treatment success beyond traditional efficacy endpoints.
Integrating Bladder-Directed and Systemic Therapy in MIBCDr. Rini outlined the three major components of perioperative treatment for urothelial cancer: neoadjuvant systemic therapy, bladder-directed therapy, and adjuvant systemic therapy. While each component has traditionally been viewed as essential, recent advances in systemic therapy have prompted renewed questions regarding the optimal sequencing and necessity of each element.
Key questions remain regarding neoadjuvant therapy, including the optimal number of treatment cycles, the applicability of these approaches to upper tract urothelial carcinoma, whether systemic therapy should precede chemoradiotherapy, and how quality-of-life considerations should be weighed against improvements in disease-free and overall survival.
Similarly, the role of bladder-directed therapy is evolving. Dr. Rini highlighted several unresolved issues: whether all patients require definitive bladder treatment, how clinical complete response should be defined, whether selected patients can safely avoid bladder intervention altogether, the future role of chemoradiotherapy, and whether biomarkers such as circulating tumor DNA (ctDNA), urine tumor DNA (utDNA), and advanced imaging can improve patient selection.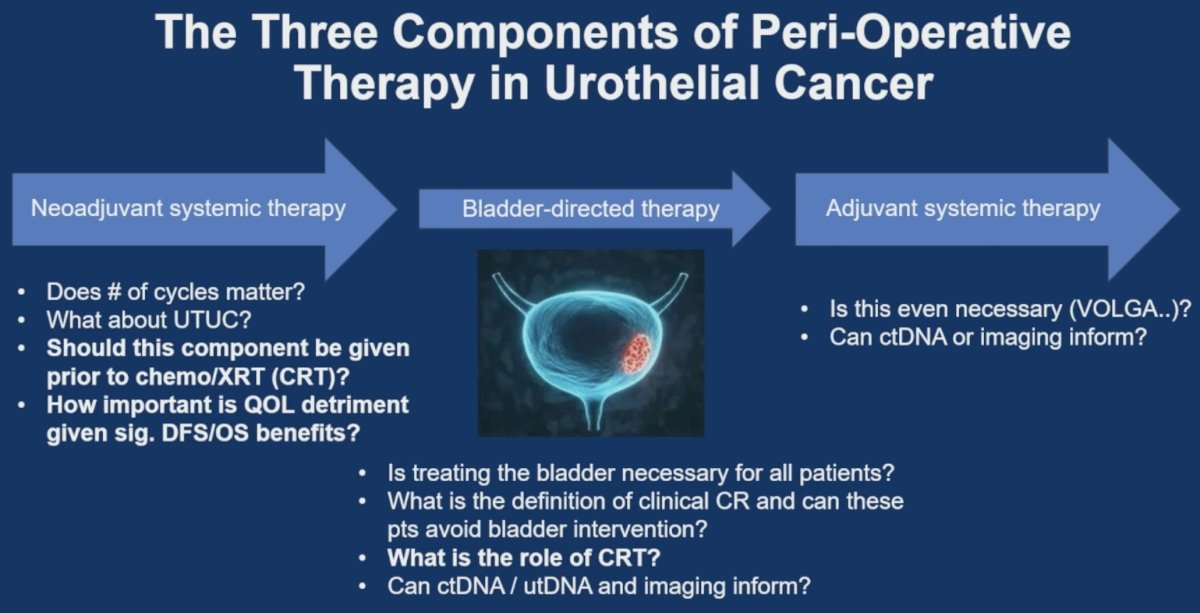
RAD-IO: Encouraging Early Results, but Longer Follow-Up Needed
Dr. Rini discussed the phase II RAD-IO study evaluating durvalumab combined with chemoradiotherapy using 5-fluorouracil and mitomycin C in patients with localized MIBC.
He noted several reassuring findings regarding treatment feasibility. All 54 patients received the planned radiotherapy dose of 55 Gy in 20 fractions, with 87% completing treatment without delay or extension. Chemotherapy delivery was largely maintained, while 61% of patients completed all planned durvalumab treatment.
Importantly, the addition of durvalumab did not appear to compromise either radiotherapy or chemotherapy delivery, suggesting that integration of immune checkpoint inhibition into bladder-preservation strategies is feasible.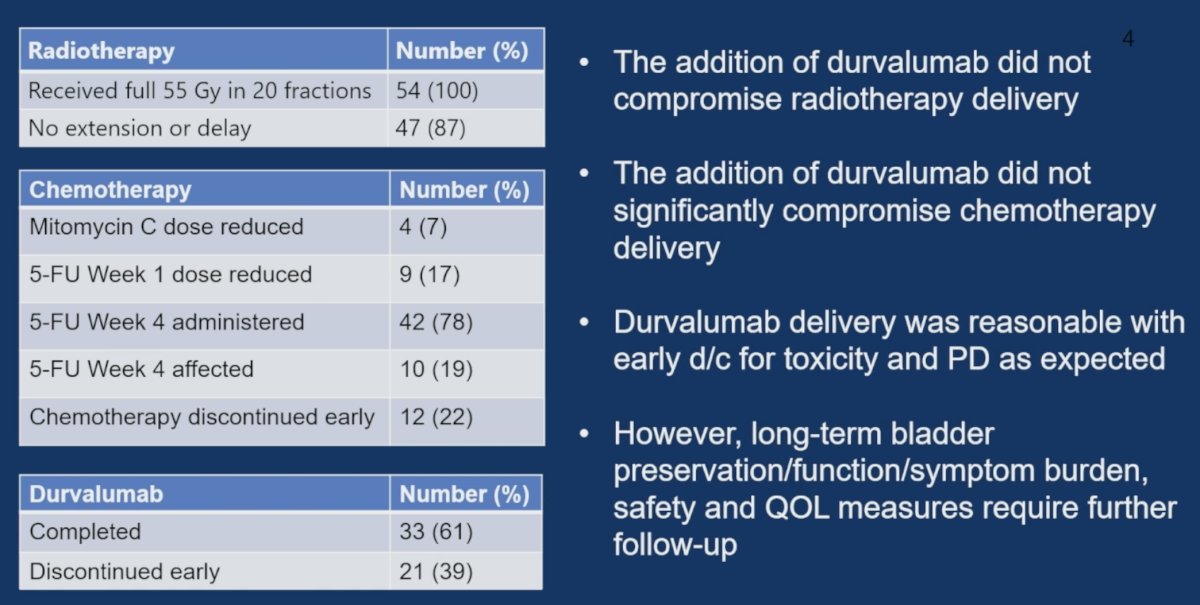
Efficacy outcomes were similarly encouraging. Twelve-month disease-free survival reached 84%, comparing favorably with the approximately 60% 12-month disease-free survival reported in the BC2001 chemoradiotherapy study. Dr. Rini also noted that these outcomes appear comparable to those achieved with contemporary peri-operative systemic therapy regimens, including KEYNOTE-905/EV-303, KEYNOTE-B15/EV-304, and NIAGARA.
Nevertheless, he emphasized that follow-up remains short, particularly given the curative-intent setting. While the early efficacy signal is promising, longer-term data evaluating bladder preservation rates, bladder function, symptom burden, toxicity, quality of life, and durability of disease control remain essential before broader conclusions can be drawn.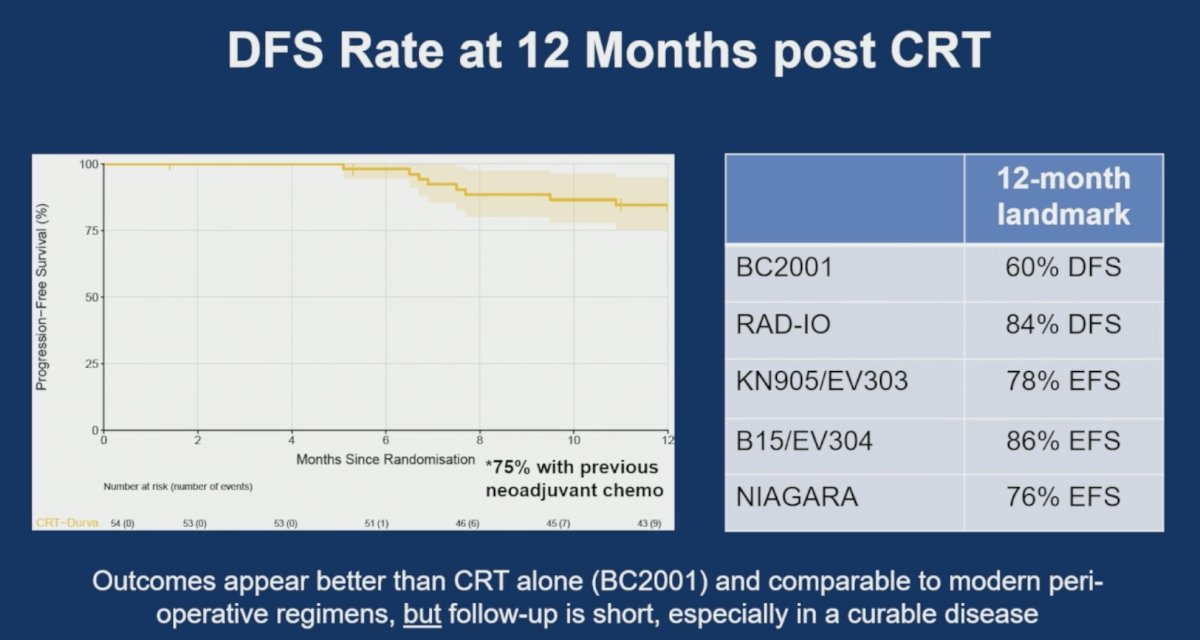
Future Directions in Bladder Preservation
Dr. Rini placed RAD-IO within a rapidly evolving landscape of bladder-preservation research.
He highlighted the ongoing phase III KEYNOTE-992 study, which is evaluating pembrolizumab combined with chemoradiotherapy versus chemoradiotherapy alone in patients pursuing bladder preservation. The trial’s primary endpoint is bladder-intact event-free survival, with overall survival as a key secondary endpoint.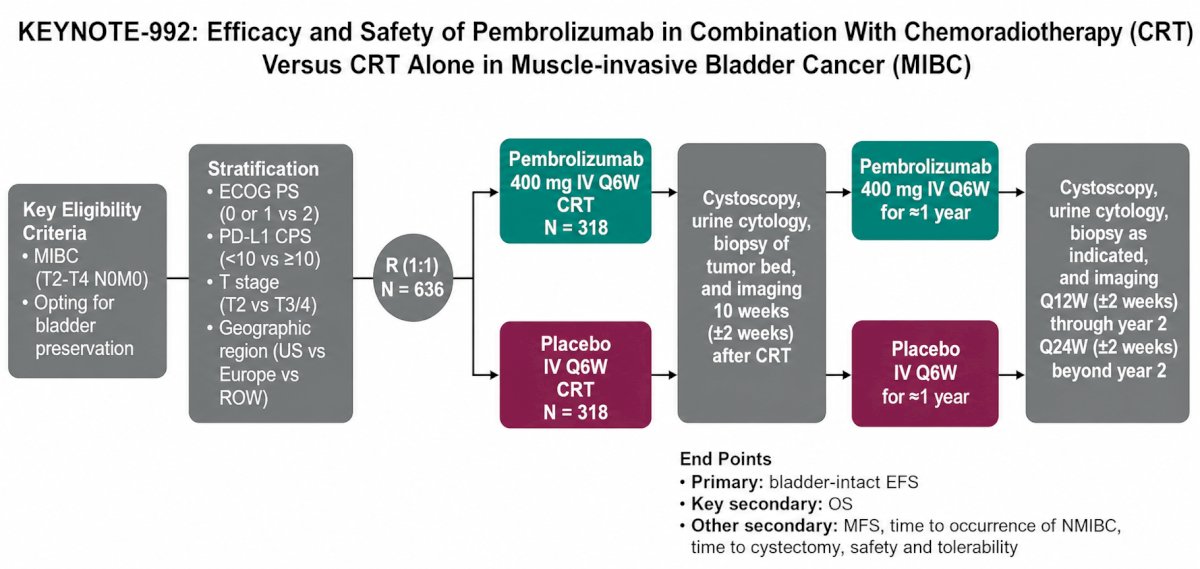
He also discussed emerging bladder-directed therapy–sparing strategies involving enfortumab vedotin plus pembrolizumab. Trials such as EV-209 and EV-309 are exploring whether patients achieving clinical complete responses following systemic therapy may safely avoid surgery or radiation altogether. These studies incorporate serial MRI, cystoscopy, cytology, and imaging assessments to determine whether treatment de-escalation can be safely pursued.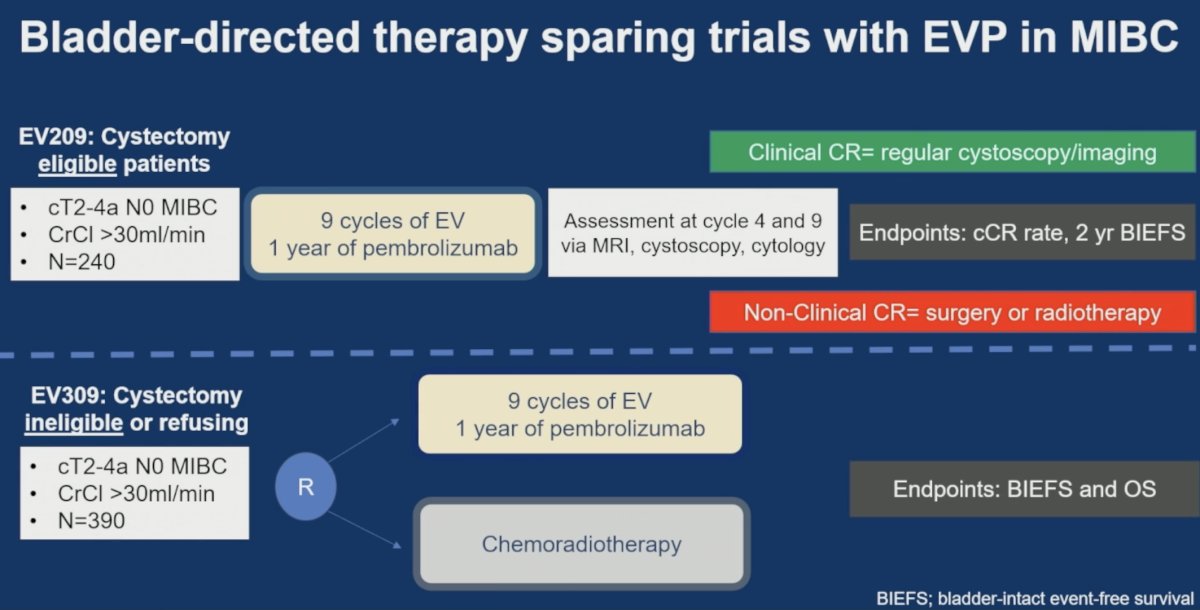
Collectively, these studies raise a fundamental question for the field: how should chemoradiotherapy be integrated into an era increasingly dominated by highly active systemic therapies?
Turning to RCC, Dr. Rini discussed results from the RAMPART trial evaluating adjuvant durvalumab alone or durvalumab plus tremelimumab following nephrectomy.
He concluded that the trial provides additional evidence supporting the activity of adjuvant immunotherapy in resected RCC. Both durvalumab-containing arms demonstrated improved disease-free survival compared with active monitoring.
Among all randomized patients, disease-free survival hazard ratios were 0.74 for durvalumab monotherapy and 0.65 for durvalumab plus tremelimumab versus active monitoring. In the high-risk/M1 NED population, the benefit appeared more pronounced, with hazard ratios of 0.77 and 0.52, respectively.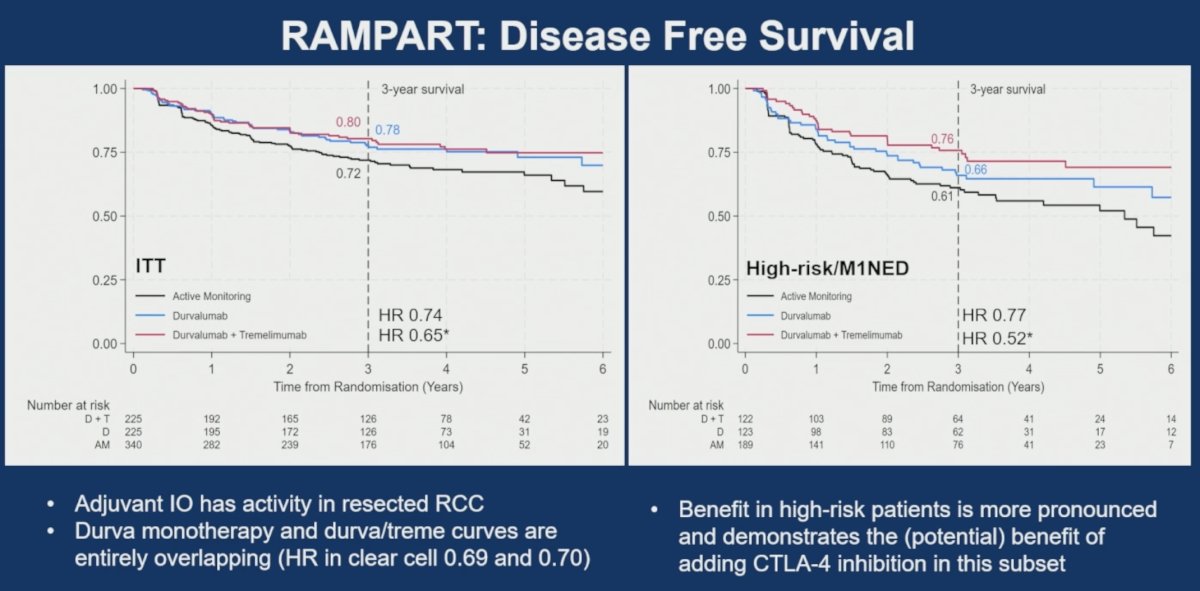
These findings suggest that patients at the highest risk of recurrence may derive the greatest benefit from adjuvant immunotherapy and raise the possibility that CTLA-4 inhibition could contribute additional efficacy in selected patients.
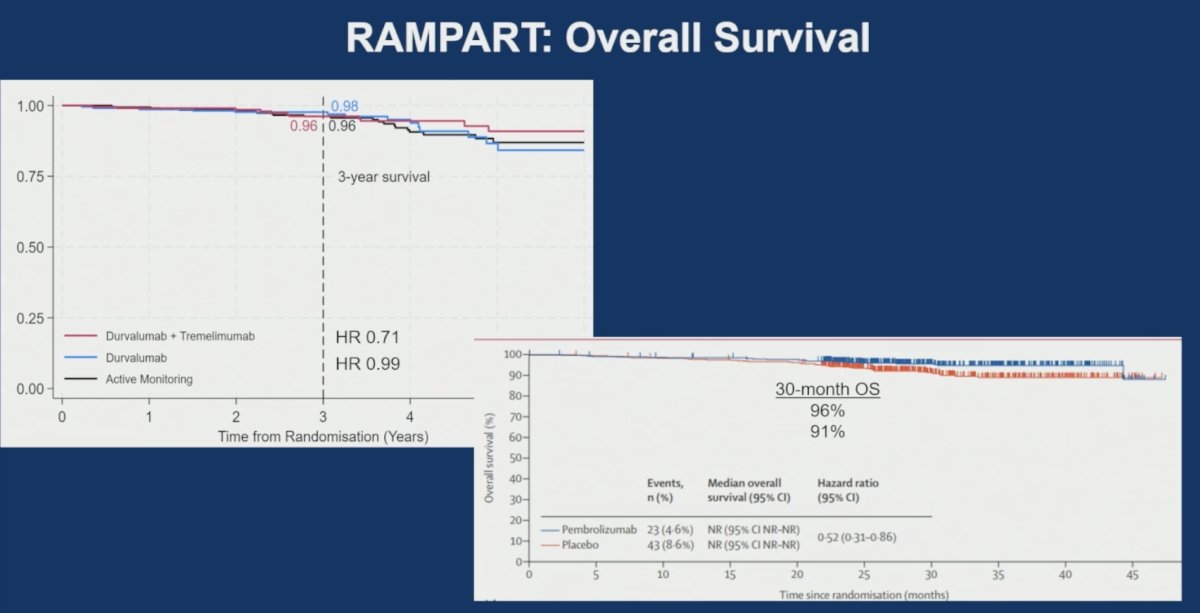
However, Dr. Rini cautioned against overinterpreting these findings. The disease-free survival curves for durvalumab monotherapy and durvalumab plus tremelimumab were largely overlapping, particularly among patients with clear-cell histology. Furthermore, overall survival data remain immature.
What Is the Added Value of CTLA-4 Inhibition?
One of the central questions posed by Dr. Rini was whether CTLA-4 inhibition meaningfully improves outcomes in the adjuvant RCC setting.
To address this issue, he compared RAMPART with other studies across both adjuvant and metastatic disease settings, including CheckMate 914, CheckMate 214, LITESPARK-012, and CheckMate 915 in melanoma.
While RAMPART demonstrated numerically improved disease-free survival with durvalumab plus tremelimumab, Dr. Rini emphasized that the additional benefit attributable to CTLA-4 blockade remains uncertain. The apparent efficacy signal must be balanced against substantially increased toxicity, with grade ≥3 adverse events increasing by approximately 32% relative to observation compared with a 21% increase observed with durvalumab monotherapy.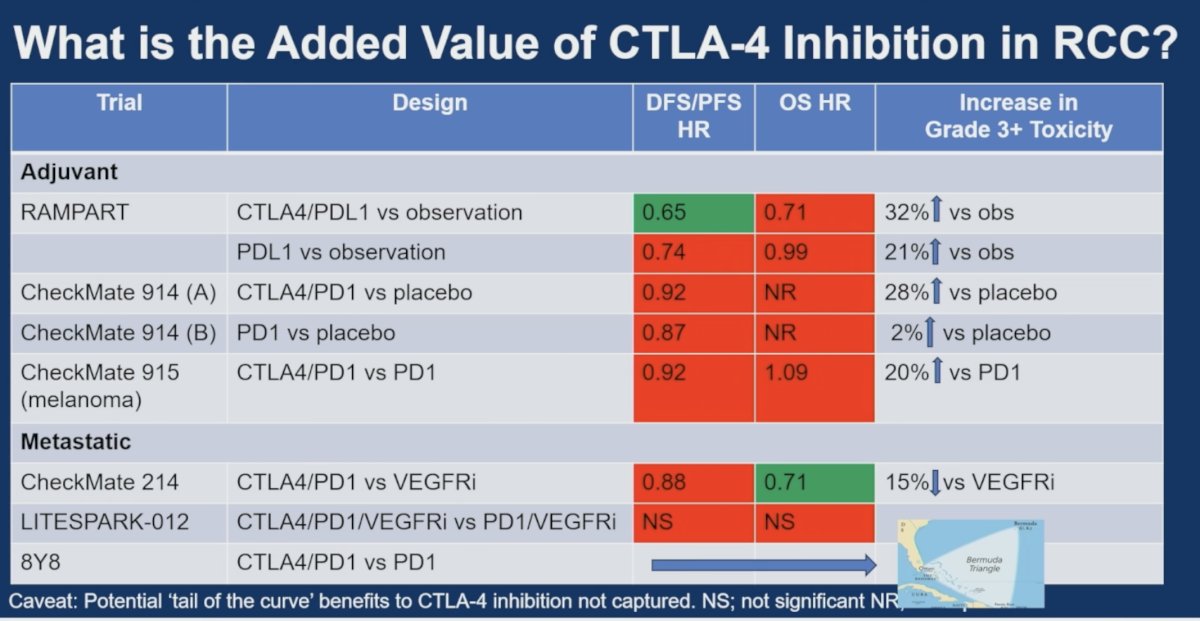
Accordingly, he concluded that additional follow-up, particularly for overall survival, will be necessary before defining the role of CTLA-4 inhibition in the adjuvant RCC setting.
Dr. Rini argued that current pathologic risk stratification methods remain relatively crude tools for treatment selection.
Using emerging data from studies evaluating ctDNA and KIM-1, he demonstrated the profound heterogeneity in recurrence risk among patients who are currently grouped together using conventional clinicopathologic criteria.
In KEYNOTE-564, ctDNA-positive patients experienced markedly inferior outcomes compared with ctDNA-negative patients, regardless of treatment assignment. Similarly, exploratory analyses of KIM-1 have suggested the potential to identify biologically distinct populations with differential benefit from adjuvant immunotherapy.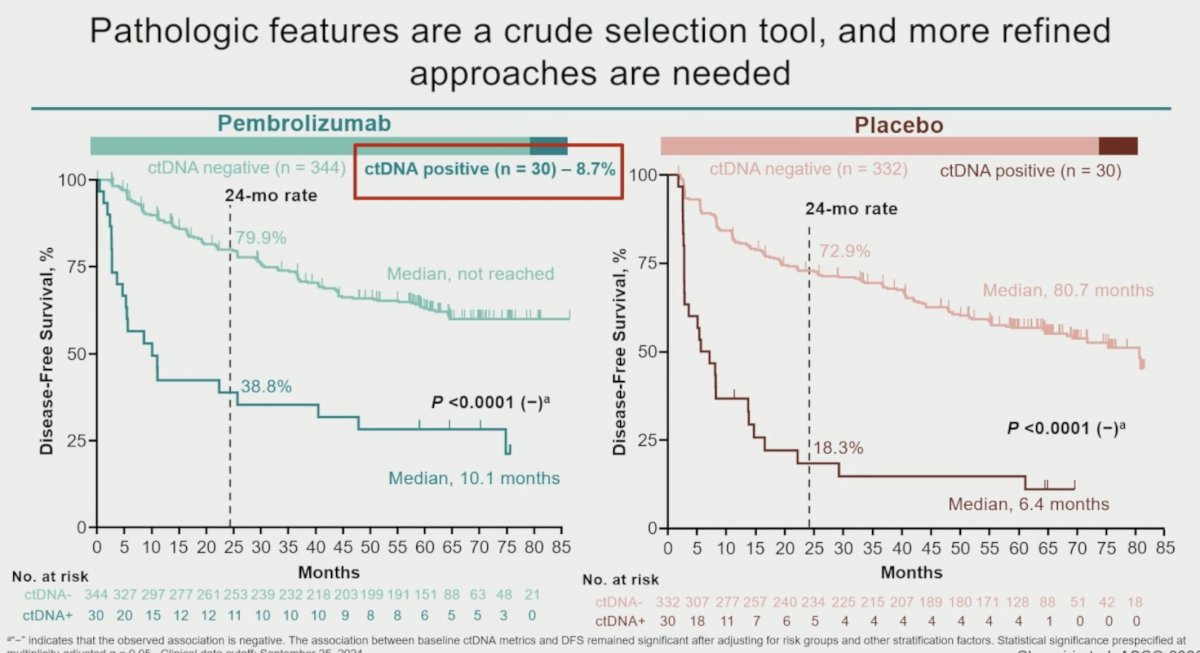
These findings reinforce the need for biomarker-driven treatment strategies capable of identifying which patients truly require adjuvant therapy and which may safely avoid overtreatment.
Importantly, Dr. Rini noted that adjuvant immunotherapy currently has no proven benefit in non-clear cell RCC. Interpretation of RAMPART subgroup analyses remains challenging because of small patient numbers, limited events, and wide confidence intervals. Central pathology review remains ongoing.
Quality of Life in the Era of Transformative TherapiesThe second major theme of Dr. Rini’s discussion centered on the limitations of contemporary quality-of-life assessment.
Reviewing patient-reported outcome data from KEYNOTE-905, he challenged the assumption that conventional quality-of-life instruments adequately capture patient experience during treatment.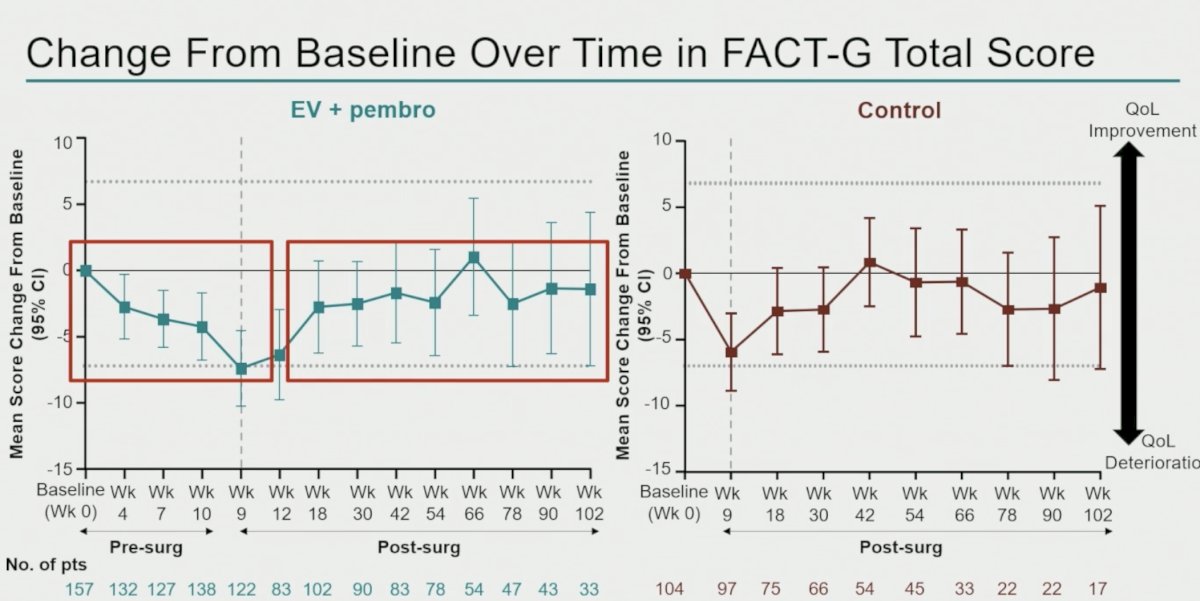
Several methodological concerns were highlighted. First, the primary week-18 assessment may fail to capture acute toxicities associated with neoadjuvant enfortumab vedotin plus pembrolizumab and the immediate perioperative period. Second, existing instruments were not designed to measure important toxicities such as peripheral neuropathy, one of the hallmark adverse events associated with enfortumab vedotin. Third, completion rates of approximately 65% may introduce substantial bias, as patients experiencing the greatest toxicity are often those least likely to complete questionnaires.
Dr. Rini further noted that averaging patient-reported outcomes across populations can obscure important individual experiences.
Despite these limitations, he emphasized that peri-operative enfortumab vedotin plus pembrolizumab is a transformative treatment strategy. In a curative setting, many patients may be willing to accept both short- and long-term toxicities if meaningful improvements in cure rates can be achieved.
Patient-Defined Toxicity and Decision RegretThe presentation by Nally and colleagues provided a complementary perspective by examining toxicity through a patient-centered lens.
Using a novel framework categorizing toxicities as life-changing, significant long-term, significant short-term, or non-significant, investigators demonstrated that traditional CTCAE grading does not adequately capture the patient experience.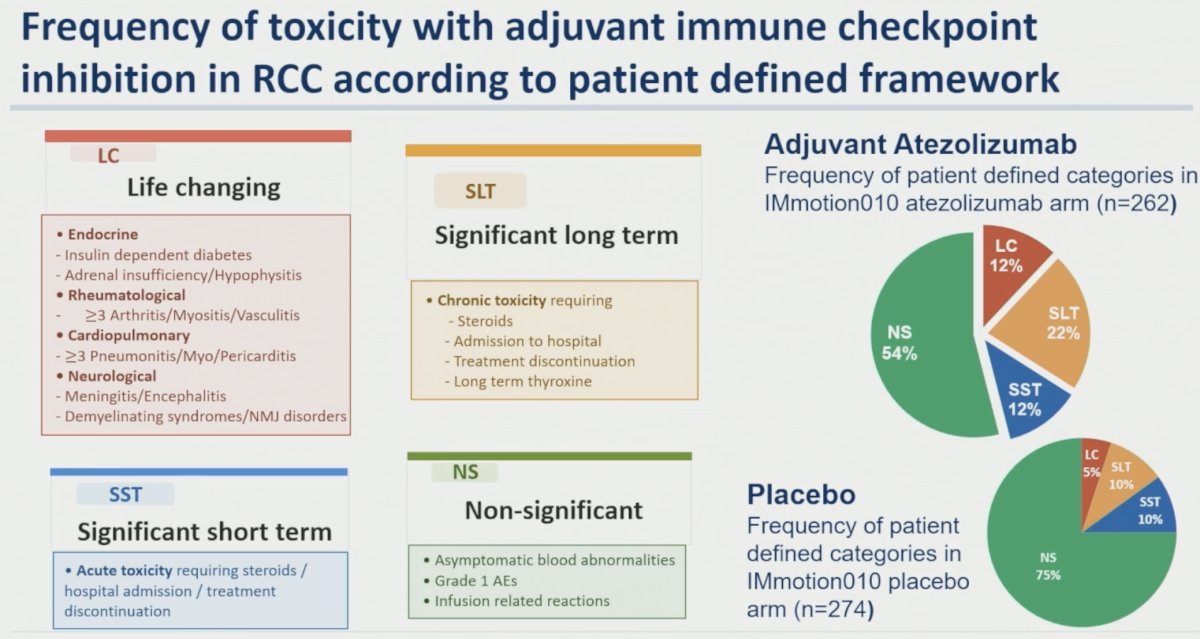
Notably, approximately one-third of patients experiencing only grade 1–2 toxicities nevertheless considered those toxicities significant or life-changing. Furthermore, conventional quality-of-life instruments showed substantial overlap between toxicity categories during treatment, with meaningful separation occurring only after therapy discontinuation, a period often not captured by standard assessments.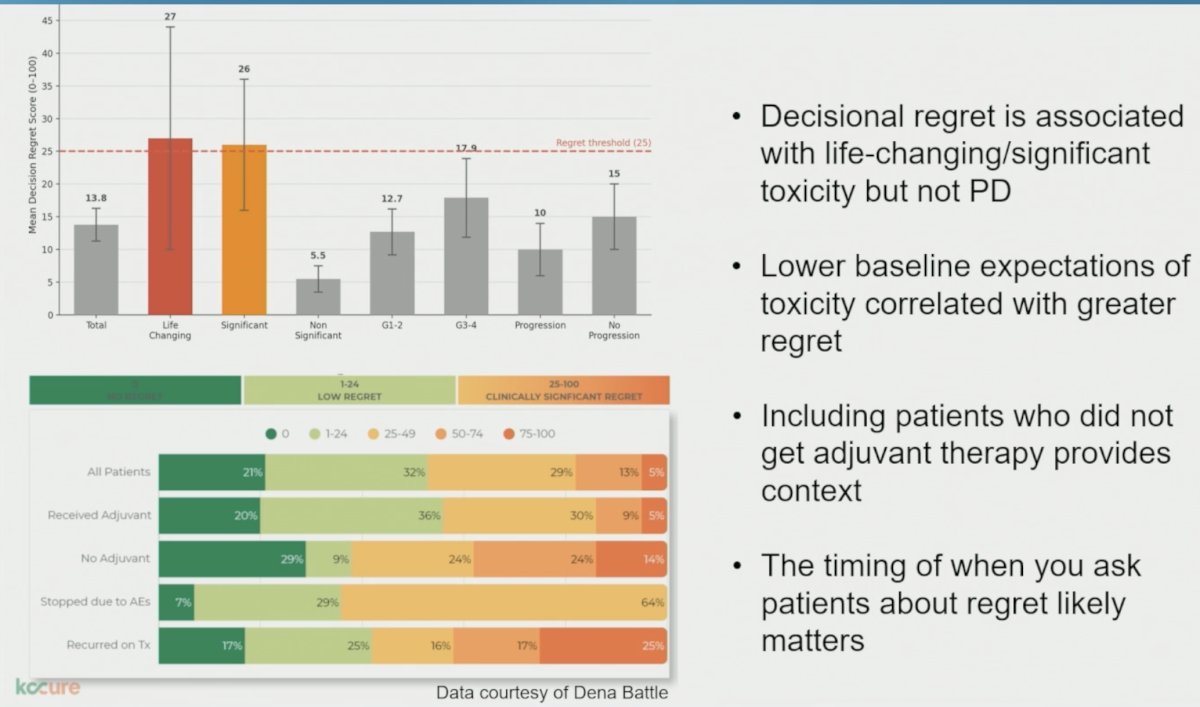
The study also demonstrated that decisional regret was associated with life-changing and significant toxicities but not with disease progression. Lower baseline expectations regarding toxicity correlated with greater regret, emphasizing the importance of patient counseling and expectation management.
Dr. Rini suggested that patient-defined toxicity frameworks and regret scores may ultimately provide a more nuanced understanding of treatment burden than conventional adverse event reporting alone.
Dr. Rini concluded by returning to the three central questions that framed his presentation:
- For MIBC, the combination of chemoradiotherapy and durvalumab appears tolerable and associated with promising short-term outcomes. However, additional data are needed to define how bladder-directed therapy should be integrated with increasingly effective systemic treatment approaches.
- For RCC, it remains unclear whether CTLA-4 inhibition provides meaningful additional benefit beyond PD-(L)1 blockade in the adjuvant setting. Longer follow-up from RAMPART, particularly for overall survival and non-clear cell disease, will be essential.
- Finally, current quality-of-life tools do not fully capture the patient experience. Emerging approaches incorporating patient-defined toxicity categories and decisional regret assessments may provide a more meaningful understanding of treatment burden and should be prospectively evaluated in future trials.
Taken together, Dr. Rini’s discussion highlighted a central challenge facing modern GU oncology: as treatments become increasingly effective, the field must simultaneously improve its ability to personalize therapy, measure patient experience, and balance cure with quality of life.
Presented by: Brian Rini, MD, Professor, Department of Medicine, Vanderbilt-Ingram Cancer Center, Nashville, TN, USA
Written by: Rashid K. Sayyid, MD, MSc, Assistant Professor, Urologic Oncologist, Department of Urology at The University of Arizona and Banner University Medical Center, Tucson, AZ – @rksayyid on X during the American Society of Clinical Oncology Genitourinary (ASCO) Annual Meeting held in Chicago, IL between May 29th and June 1st, 2026