(UroToday.com) The 2026 American Society of Clinical Oncology Genitourinary (ASCO) Annual Meeting held in Chicago, IL, between Fri, May 29 – Tues, Jun 2, 2026, was host to the New Approaches to Curing Bladder and Kidney Cancer. Dr. Srikala Sridhar discussed new approaches to curing Bladder and Kidney Cancers: Where do we stand today?
Dr. Sridhar began by highlighting the remarkable progress achieved in genitourinary oncology across both bladder and kidney cancer, emphasizing how recent advances in immunotherapy, antibody-drug conjugates, targeted therapy combinations, and biomarker-driven approaches are steadily moving the field “towards cure,” with goals of improving survival, quality of life, and long-term disease control. In bladder cancer, she reviewed perioperative immunotherapy strategies and the growing role of personalized molecular profiling. In kidney cancer, she discussed adjuvant pembrolizumab strategies. She posed a critical question to the audience: as outcomes improve, are we adequately measuring the outcomes that matter most to patients?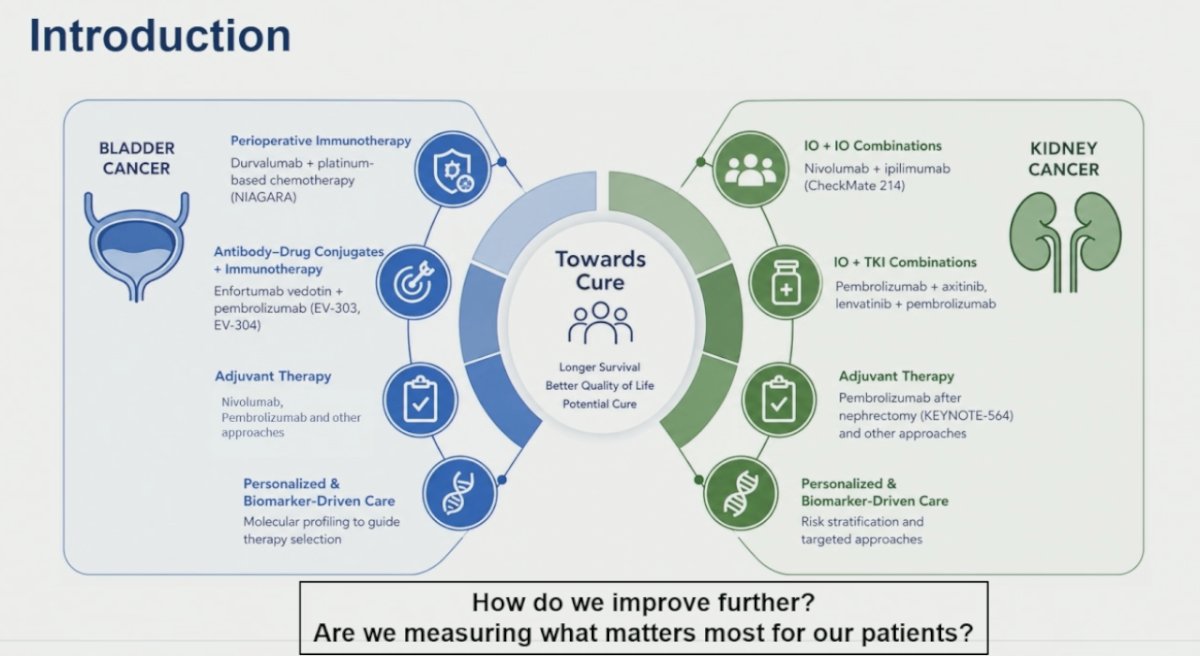
Dr. Sridhar then discussed the major paradigm shift occurring in muscle-invasive bladder cancer with perioperative enfortumab vedotin plus pembrolizumab. She highlighted the EV-304 trial, where the combination achieved markedly higher pathologic complete response rates compared with cisplatin plus gemcitabine (55.8% versus 32.5%), raising the important clinical question of whether all patients may still require cystectomy in the future.1,2 At the same time, she emphasized that these regimens are associated with clinically relevant toxicities, including rash, neuropathy, and hyperglycemia, underscoring the need to better understand the short- and long-term impact of treatment-related adverse events on patients’ quality of life. 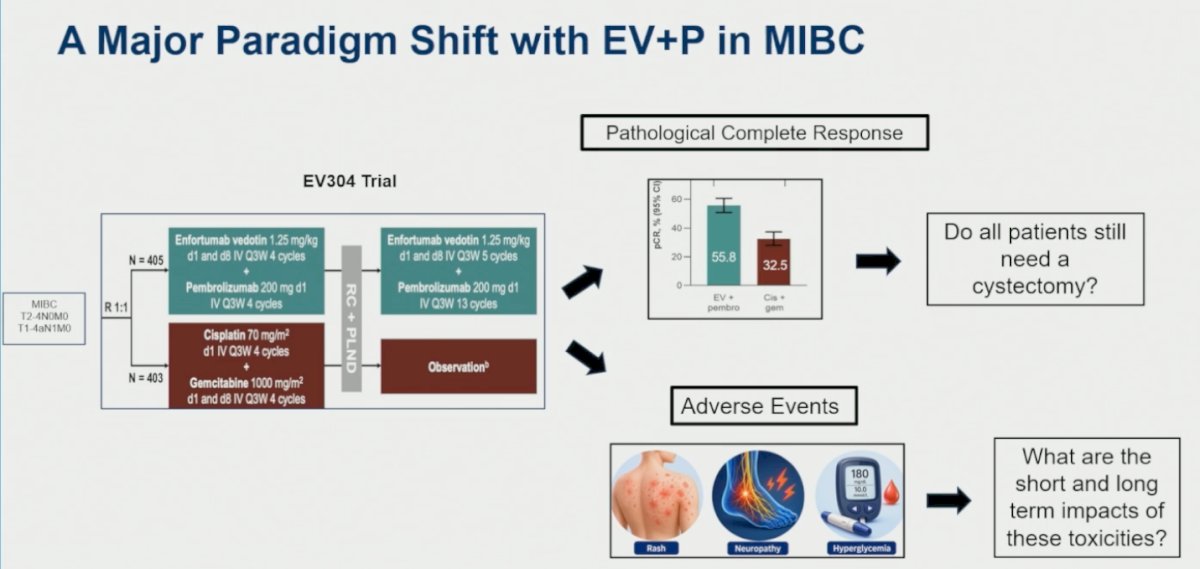
Dr. Sridhar emphasized that bladder-sparing approaches are not a new concept in MIBC. For eligible patients, trimodality therapy (TMT), consisting of TURBT followed by concurrent chemotherapy and radiation, may be a reasonable alternative to radical cystectomy. She noted that retrospective propensity analyses suggest comparable long-term outcomes between TMT and radical cystectomy in selected patients, although these remain among the limited comparative data available in this setting.3 Importantly, she highlighted that the bladder-sparing population is changing. While these approaches were historically considered mainly for patients who were not cystectomy-eligible, younger and fitter patients are increasingly interested in bladder preservation. This shift raises two important questions: how to select the ideal patient for bladder-sparing treatment, and how to integrate TMT with novel systemic therapies.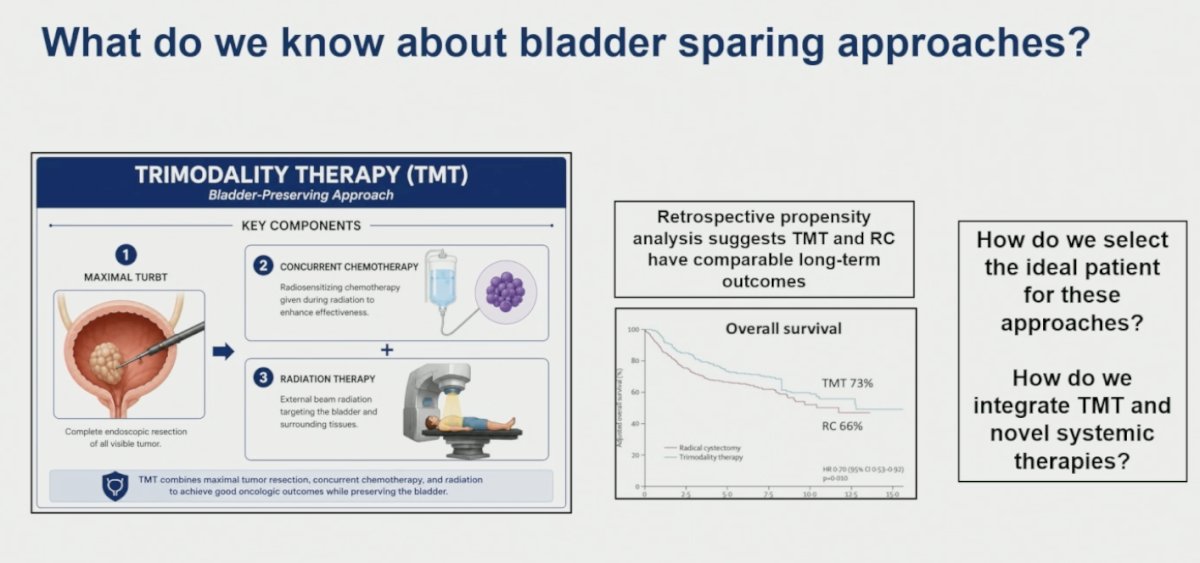
Building on the evolving interest in bladder-sparing strategies, Dr. Sridhar highlighted the phase 2 RAD-IO trial evaluating the addition of durvalumab to chemoradiation with mitomycin C and 5-FU in patients undergoing TMT. The study was designed not only to determine whether adding immunotherapy to chemoradiation is safe and improves outcomes, but also to address broader questions in the bladder preservation space, including what the most appropriate clinical endpoints should be and how best to incorporate patient-reported outcomes for patients receiving TMT.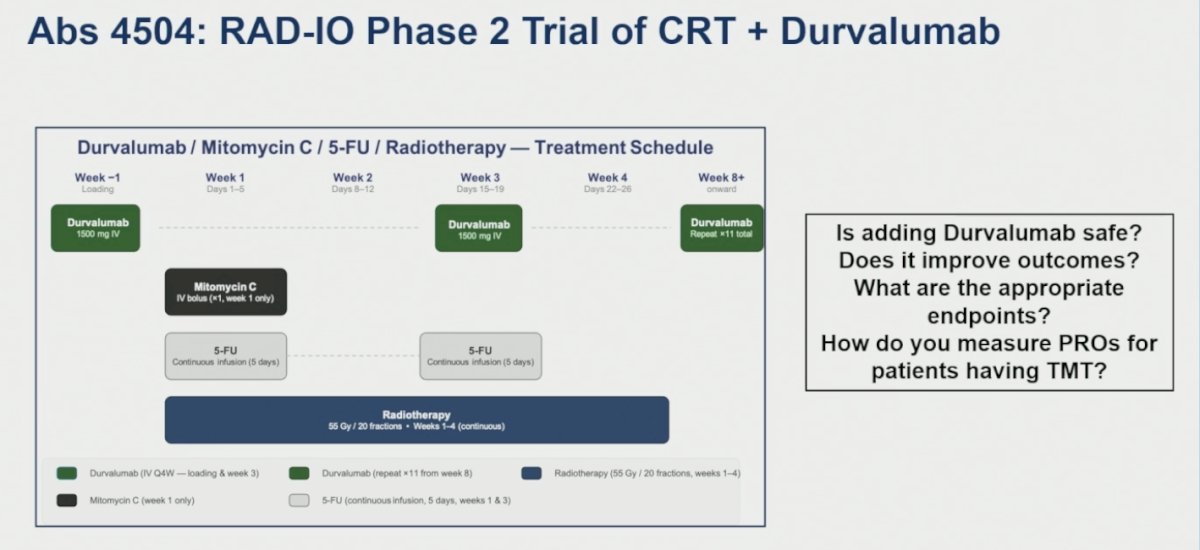
Dr. Sridhar also discussed the growing importance of patient-reported outcomes (PROs) and health-related quality of life (HRQOL) assessments in the era of novel perioperative and bladder-sparing therapies. Using EV-303 as an example, she emphasized that understanding treatment impact extends beyond traditional oncologic endpoints and should include symptoms and toxicities, physical functioning, emotional well-being, social and role functioning, quality of life, treatment burden, and patient priorities and preferences.1,2 She also raised several practical challenges regarding PRO integration in clinical trials, including whether current tools adequately capture quality of life, whether assessments are being performed at the appropriate time points, how PRO completion rates influence interpretation, and how outcomes should be evaluated in patients who discontinue therapy early or experience significant toxicity.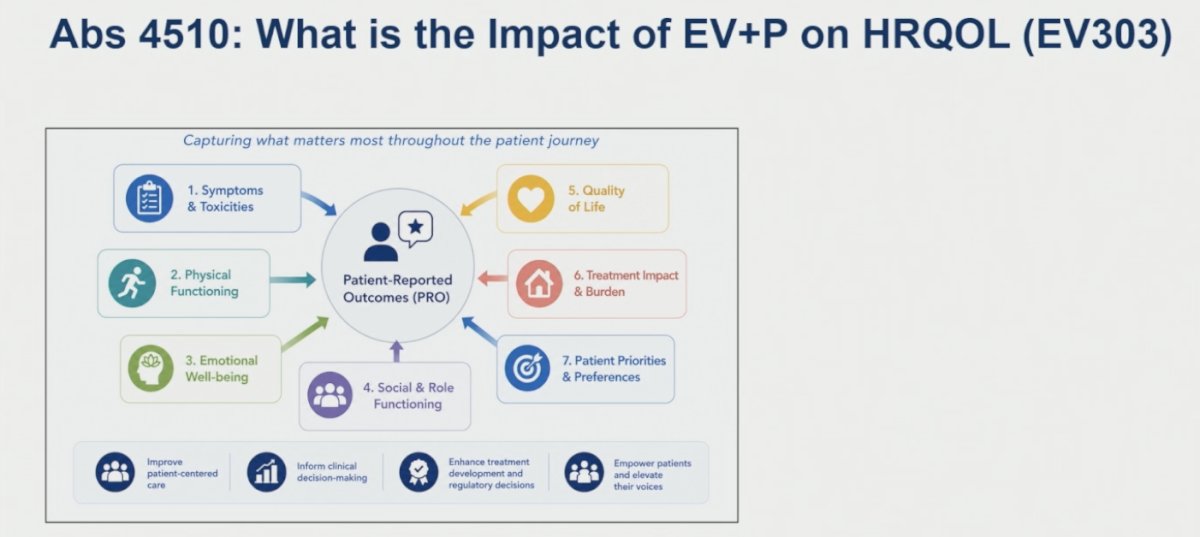
Renal cell carcinoma (RCC)
Transitioning to RCC, Dr. Sridhar highlighted that the adjuvant immunotherapy landscape has produced mixed results despite significant enthusiasm surrounding perioperative approaches. While KEYNOTE-5644 demonstrated a disease-free survival and overall survival benefit with one year of adjuvant pembrolizumab, several other studies, including IMmotion010, CheckMate 914,5 and PROSPER,6 failed to show meaningful improvements in outcomes. More recent studies, such as RAMPART7 and LITESPARK-022, have reported encouraging disease-free survival signals, although overall survival data remain pending. These divergent results raise important questions regarding whether differences are driven by patient selection, choice of therapeutic agents, study design, or other underlying biologic factors.

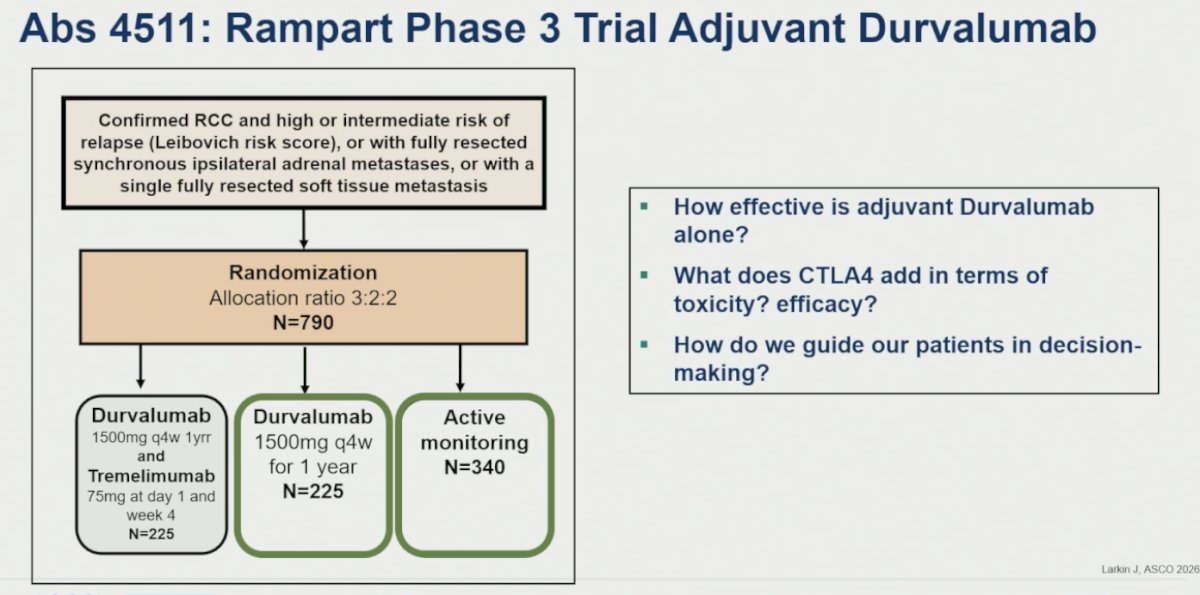
Dr. Sridhar also reviewed the phase 3 RAMPART trial evaluating adjuvant durvalumab with or without tremelimumab in patients with high- or intermediate-risk RCC following surgery. In this study, 790 patients were randomized in a 3:2:2 fashion to durvalumab plus tremelimumab, durvalumab monotherapy, or active monitoring. She emphasized that the study was designed to address several clinically relevant questions in the adjuvant RCC setting, including the efficacy of adjuvant durvalumab alone, the incremental benefit and toxicity associated with CTLA-4 inhibition, and how these data can better guide shared decision-making with patients.7
Dr. Sridhar also discussed the concept of “decision regret” in the adjuvant RCC setting, emphasizing the delicate balance between potential oncologic benefit and treatment-related toxicity when counseling patients about adjuvant therapy. She highlighted validated decision regret scales as tools to measure distress or regret following healthcare decisions, noting that significant regret is often associated with permanent toxicities. These observations underscore the importance of clear risk communication and shared decision-making, while also suggesting that improved biomarkers for both response and toxicity may help better individualize adjuvant treatment strategies in the future.
Lastly, she highlighted Abstract 4512, evaluating decision regret and toxicity perception in patients receiving adjuvant pembrolizumab for RCC. She emphasized that although adjuvant pembrolizumab improves survival outcomes, important questions remain regarding how patients perceive treatment-related toxicity and whether some patients ultimately regret their treatment decisions. The study also explored whether conventional CTCAE grading systems and current quality-of-life tools adequately capture the real-world burden of immune-related adverse events, and whether patient-defined toxicity classifications may better reflect treatment impact. Ultimately, she noted that understanding what drives decision regret, treatment toxicity, disease recurrence, or both remains critical to improving patient-centered care and shared decision-making in the adjuvant setting.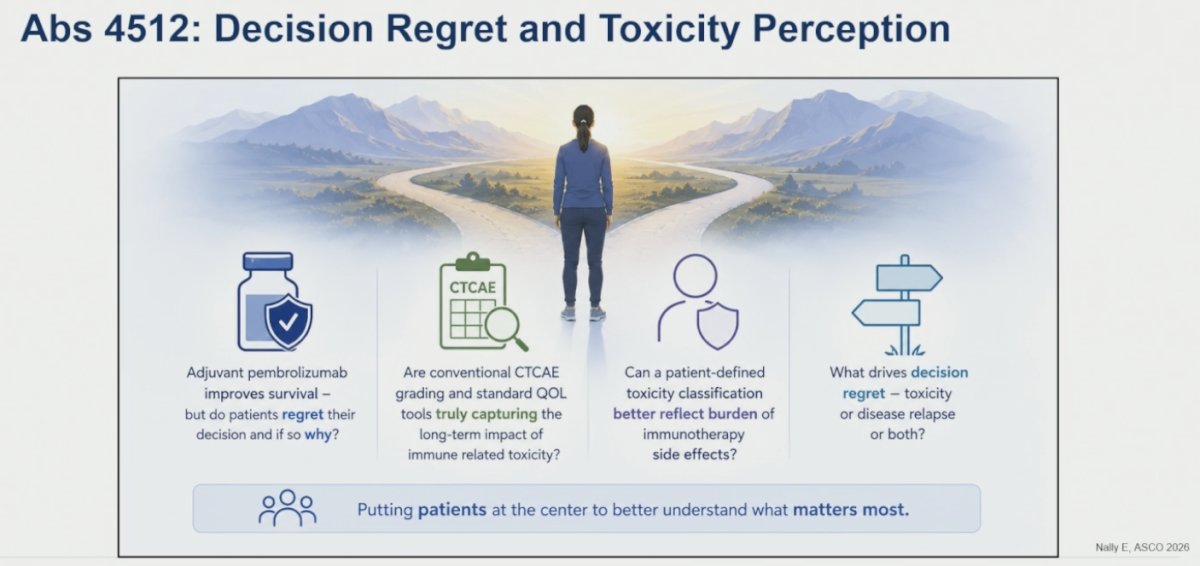
Dr Sridhar concluded her presentation with the following key points:
- Major advances in GU oncology have improved outcomes across bladder cancer and RCC, although many important clinical questions remain unanswered
- As novel therapies and treatment combinations become increasingly available, greater emphasis must be placed on understanding how to support patients before, during, and after treatment decision-making
- Improved patient selection and better integration of biomarkers and novel systemic therapies will be critical to further refining outcomes
- There is a growing need to develop and implement tools that more accurately capture patient-reported outcomes, treatment burden, and quality of life alongside traditional oncologic endpoints
Presented by: Srikala Sridhar, MD, MSc, FRCPC, Professor, Department of Medicine, University of Toronto, GU Medical Oncologist, Princess Margaret Cancer Center, Toronto, ON
Written by: Rashid K. Sayyid, MD, MSc, Assistant Professor, Urologic Oncologist, Department of Urology at The University of Arizona and Banner University Medical Center, Tucson, AZ – @rksayyid on X during the American Society of Clinical Oncology Genitourinary (ASCO) Annual Meeting held in Chicago, IL between May 29th and June 1st, 2026
References:- Vulsteke C, Adra N, Danchaivijitr P, Sabadash M, Rodriguez-Vida A, Zhang Z, Atduev V, Göger YE, Rausch S, Kang SH, Loriot Y, Bedke J, Galsky MD, O'Donnell PH, von Amsberg G, Alimohamed N, Sulimka G, Gupta S, Paramonov V, Nakane K, Mihm M, Meng C, Huang CD, Ramamurthy C, Homet Moreno B, Ullén A; KEYNOTE-905/EV-303 Investigators. Perioperative Enfortumab Vedotin and Pembrolizumab in Bladder Cancer. N Engl J Med. 2026 Apr 2;394(13):1257-1269. doi: 10.1056/NEJMoa2511674. Epub 2026 Feb 18. PMID: 41707170.
- Sternschuss M, Rosenberg JE. Enfortumab vedotin and pembrolizumab: redefining the standard of care for previously untreated advanced urothelial cancer. Future Oncol. 2025 May;21(11):1333-1348. doi: 10.1080/14796694.2025.2482363. Epub 2025 Mar 25. PMID: 40129250; PMCID: PMC12051594.
- Zlotta AR, Ballas LK, Niemierko A, Lajkosz K, Kuk C, Miranda G, Drumm M, Mari A, Thio E, Fleshner NE, Kulkarni GS, Jewett MAS, Bristow RG, Catton C, Berlin A, Sridhar SS, Schuckman A, Feldman AS, Wszolek M, Dahl DM, Lee RJ, Saylor PJ, Michaelson MD, Miyamoto DT, Zietman A, Shipley W, Chung P, Daneshmand S, Efstathiou JA. Radical cystectomy versus trimodality therapy for muscle-invasive bladder cancer: a multi-institutional propensity score matched and weighted analysis. Lancet Oncol. 2023 Jun;24(6):669-681. doi: 10.1016/S1470-2045(23)00170-5. Epub 2023 May 12. PMID: 37187202.
- Choueiri TK, Tomczak P, Park SH, Venugopal B, Ferguson T, Symeonides SN, Hajek J, Chang YH, Lee JL, Sarwar N, Haas NB, Gurney H, Sawrycki P, Mahave M, Gross-Goupil M, Zhang T, Burke JM, Doshi G, Melichar B, Kopyltsov E, Alva A, Oudard S, Topart D, Hammers H, Kitamura H, McDermott DF, Silva A, Winquist E, Cornell J, Elfiky A, Burgents JE, Perini RF, Powles T; KEYNOTE-564 Investigators. Overall Survival with Adjuvant Pembrolizumab in Renal-Cell Carcinoma. N Engl J Med. 2024 Apr 18;390(15):1359-1371. doi: 10.1056/NEJMoa2312695. PMID: 38631003
- Motzer RJ, Russo P, Grünwald V, Tomita Y, Zurawski B, Parikh O, Buti S, Barthélémy P, Goh JC, Ye D, Lingua A, Lattouf JB, Albigès L, George S, Shuch B, Sosman J, Staehler M, Vázquez Estévez S, Simsek B, Spiridigliozzi J, Chudnovsky A, Bex A. Adjuvant nivolumab plus ipilimumab versus placebo for localised renal cell carcinoma after nephrectomy (CheckMate 914): a double-blind, randomised, phase 3 trial. Lancet. 2023 Mar 11;401(10379):821-832. doi: 10.1016/S0140-6736(22)02574-0. Epub 2023 Feb 9. PMID: 36774933; PMCID: PMC10259621.
- Allaf ME, Kim SE, Master V, McDermott DF, Harshman LC, Cole SM, Drake CG, Signoretti S, Akgul M, Baniak N, Li-Ning E, Palmer MB, Emamekhoo H, Adra N, Kaimakliotis H, Ged Y, Pierorazio PM, Abel EJ, Bilen MA, Ogan K, Moon HH, Ramaswamy KA, Singer EA, Mayer TM, Lohrey J, Margulis V, Gills J, Delacroix SE, Waples MJ, James AC, Wang P, Choueiri T, Michaelson MD, Kapoor A, Heng DY, Shuch B, Leibovich BC, Lara PN, Manola J, Maskens D, Battle D, Uzzo R, Bratslavsky G, Haas NB, Carducci MA. Perioperative nivolumab versus observation in patients with renal cell carcinoma undergoing nephrectomy (PROSPER ECOG-ACRIN EA8143): an open-label, randomised, phase 3 study. Lancet Oncol. 2024 Aug;25(8):1038-1052. doi: 10.1016/S1470-2045(24)00211-0. Epub 2024 Jun 25. Erratum in: Lancet Oncol. 2025 Dec;26(12):e625. doi: 10.1016/S1470-2045(25)00522-4. PMID: 38942046; PMCID: PMC11323681.
- Oza B, Frangou E, Smith B, Bryant H, Kaplan R, Choodari-Oskooei B, Powles T, Stewart GD, Albiges L, Bex A, Choueiri TK, Davis ID, Eisen T, Fielding A, Harrison D, McWhirter A, Mulhere S, Nathan P, Rini B, Ritchie A, Scovell S, Shakeshaft C, Stockler MR, Thorogood N, Parmar MKB, Larkin J, Meade A. RAMPART: A phase III multi-arm multi-stage trial of adjuvant checkpoint inhibitors in patients with resected primary renal cell carcinoma (RCC) at high or intermediate risk of relapse. Contemp Clin Trials. 2021 Sep;108:106482. doi: 10.1016/j.cct.2021.106482. Epub 2021 Sep 16. PMID: 34538402; PMCID: PMC8520913.