(UroToday.com) The 2026 American Society of Clinical Oncology (ASCO) Annual Meeting was host to a session on new approaches to curing bladder and kidney cancer. Dr. Peter O'Donnell presented patient-reported outcomes (PROs) from the phase III KEYNOTE-905/EV-303 trial evaluating perioperative enfortumab vedotin (EV) plus pembrolizumab in cisplatin-ineligible patients with muscle-invasive bladder cancer (MIBC). These exploratory analyses assessed the impact of treatment on health-related quality of life (HRQoL), cystectomy-specific outcomes, and overall health status.
As previously reported, the randomized, open-label phase III KEYNOTE-905 study demonstrated significant improvements in efficacy outcomes with perioperative EV plus pembrolizumab and radical cystectomy with pelvic lymph node dissection (RC + PLND) compared to RC + PLND alone in patients with MIBC who were ineligible for or declined cisplatin-based chemotherapy. Efficacy outcomes included:
- Event-free survival (primary endpoint): HR 0.40 (95% CI: 0.28–0.57); one-sided P < 0.0001
- Overall survival (key secondary endpoint): HR 0.50 (95% CI: 0.33–0.74); one-sided P = 0.0002
- Pathologic complete response (key secondary endpoint): 57.1% versus 8.6%; one-sided P < 0.000001
Based on these results, EV plus pembrolizumab received FDA approval as neoadjuvant and adjuvant treatment for adult patients with MIBC who are ineligible for cisplatin-containing chemotherapy.
KEYNOTE-905/EV-303 (NCT03924895) randomized 344 patients in a 1:1 fashion. Eligible patients had MIBC, clinical stage T2-T4aN0M0 or T1-T4aN1M0 disease by central assessment, ≥50% urothelial histology, ECOG performance status 0–2, and were cisplatin-ineligible or declined cisplatin.
Patients were randomized to:
- EV 1.25 mg/kg IV on days 1 and 8 plus pembrolizumab 200 mg IV every 3 weeks for 3 neoadjuvant cycles followed by RC + PLND and adjuvant EV every 3 weeks for 6 cycles plus pembrolizumab every 3 weeks for 14 cycles (n=170)
- RC + PLND alone followed by observation (n=174)
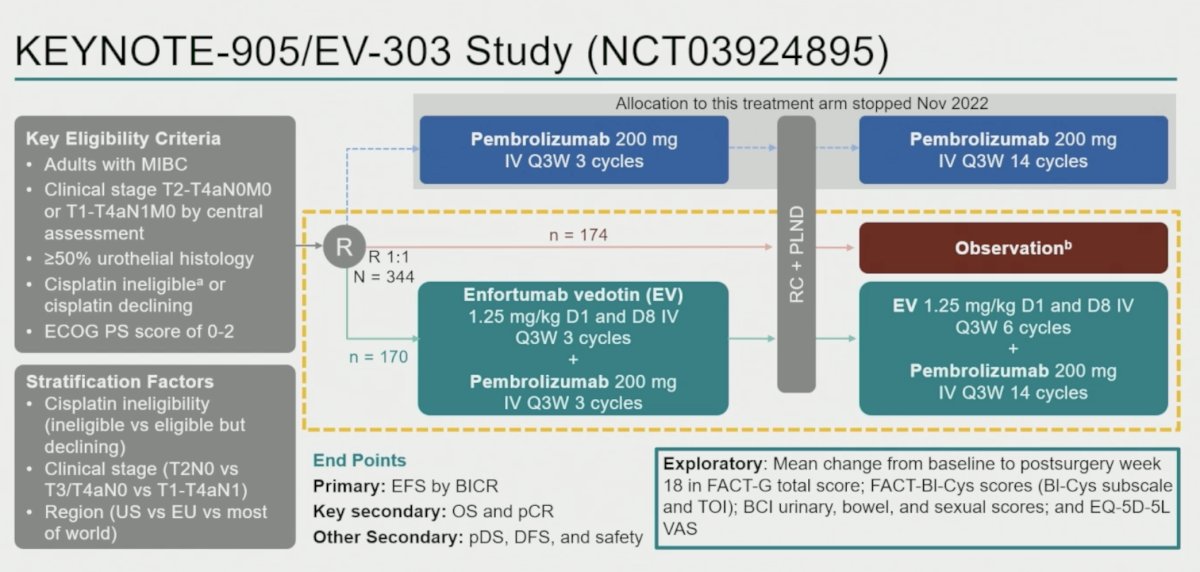
The exploratory PRO endpoints included mean change from baseline to post-surgery week 18 in:
- FACT-G total score
- FACT-Bl-Cys total score
- FACT-Bl-Cys Trial Outcome Index (TOI)
- Bladder Cancer Index (BCI) urinary, bowel, and sexual domains
- EQ-5D-5L visual analogue scale (VAS)
PRO analyses included all randomized participants with baseline and at least one postbaseline PRO assessment. Mean changes over time were evaluated within each treatment arm separately; no between-group statistical comparisons were performed. Post-surgery week 18 was selected in a blinded manner because completion and compliance rates were approximately 60% and 80%, respectively.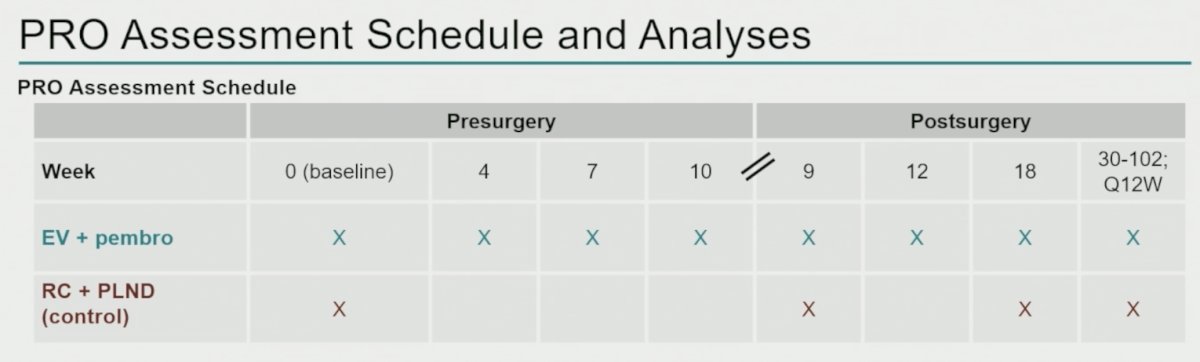
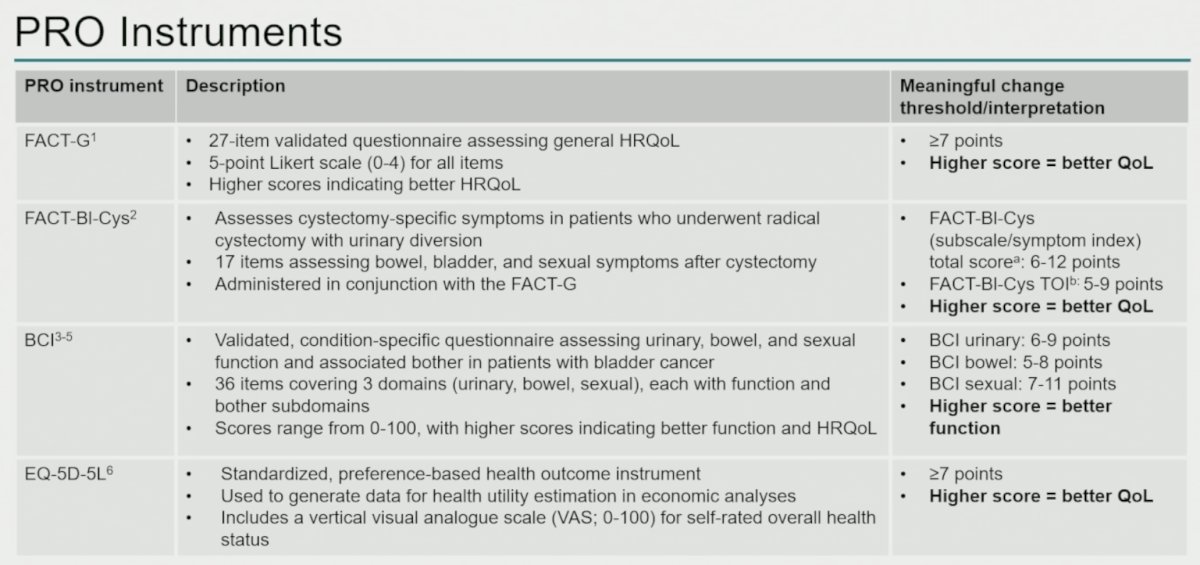
The PRO instruments utilized included:
- FACT-G, a 27-item validated questionnaire assessing general HRQoL, with clinically meaningful deterioration defined as ≥7 points
- FACT-Bl-Cys, a cystectomy-specific instrument evaluating bowel, bladder, and sexual symptoms, with clinically meaningful change thresholds of 6–12 points for the total score and 5–9 points for the TOI
- Bladder Cancer Index (BCI), assessing urinary, bowel, and sexual function domains, with clinically meaningful deterioration thresholds of 6–9, 5–8, and 7–11 points, respectively
- EQ-5D-5L VAS, with a clinically meaningful threshold of ≥7 points
Completion and compliance rates at post-surgery week 18 were high in both treatment groups. For FACT-Bl-Cys, completion rates were approximately 65% in the EV plus pembrolizumab arm and 72% in the control arm, with compliance rates of 86% and 97%, respectively. Similar findings were observed for BCI and EQ-5D-5L assessments, with compliance rates ranging from 87% to 97%.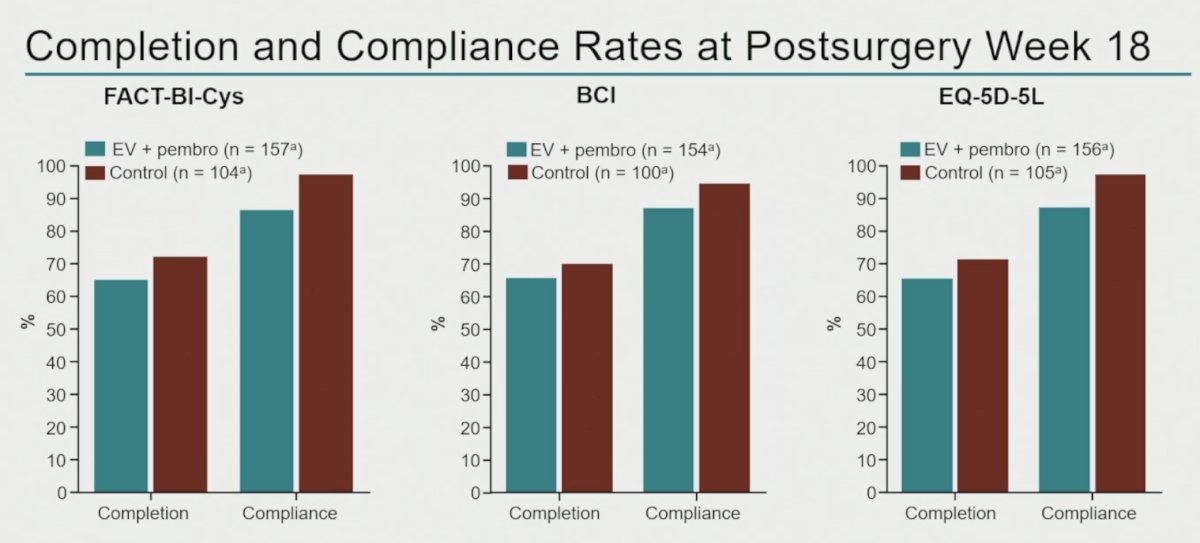
Mean change from baseline to post-surgery week 18 demonstrated preservation of HRQoL across multiple instruments.
For FACT-G total score:
- EV plus pembrolizumab: −2.73 (95% CI: −6.22 to 0.75)
- Control: −2.84 (95% CI: −6.11 to 0.43)
For FACT-Bl-Cys total score:
- EV plus pembrolizumab: 1.31 (95% CI: −0.70 to 3.32)
- Control: 1.85 (95% CI: −0.59 to 4.29)
For FACT-Bl-Cys TOI:
- EV plus pembrolizumab: −1.89 (95% CI: −5.61 to 1.84)
- Control: −0.58 (95% CI: −4.35 to 3.20)
For EQ-5D-5L VAS:
- EV plus pembrolizumab: −2.52 (95% CI: −7.23 to 2.19)
- Control: −0.39 (95% CI: −5.14 to 4.36)
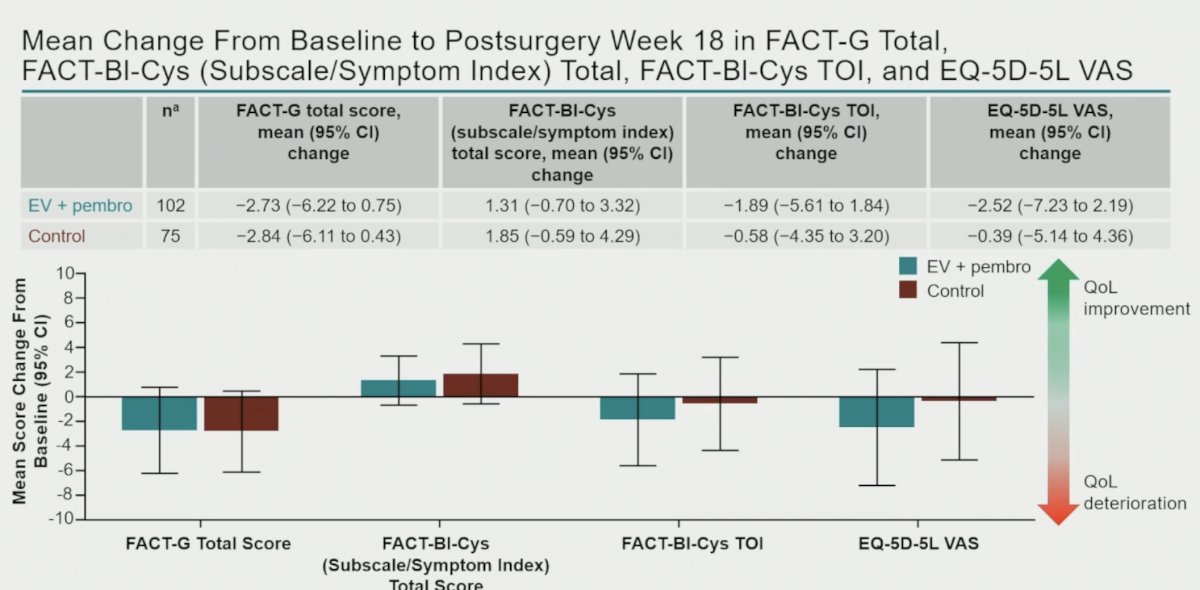
Importantly, mean changes in general HRQoL, cystectomy-specific HRQoL, and overall health status did not exceed established thresholds for clinically meaningful deterioration.
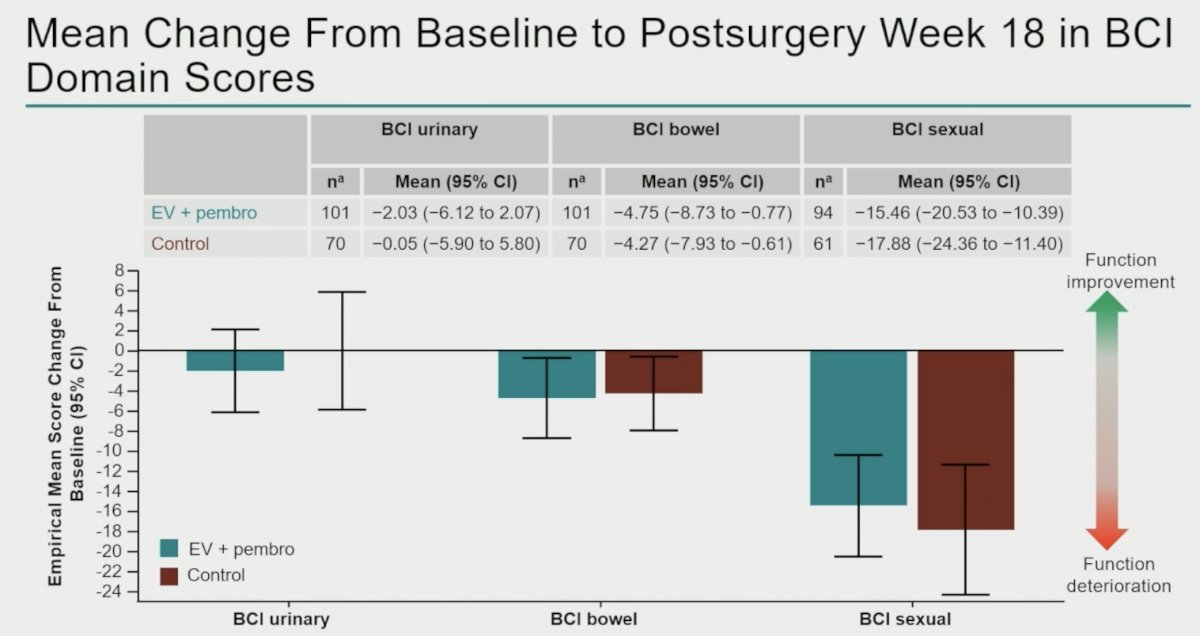
BCI domain analyses similarly demonstrated preservation of function following treatment.
For urinary function:
- EV plus pembrolizumab: −2.03 (95% CI: −6.12 to 2.07)
- Control: −0.05 (95% CI: −5.90 to 5.80)
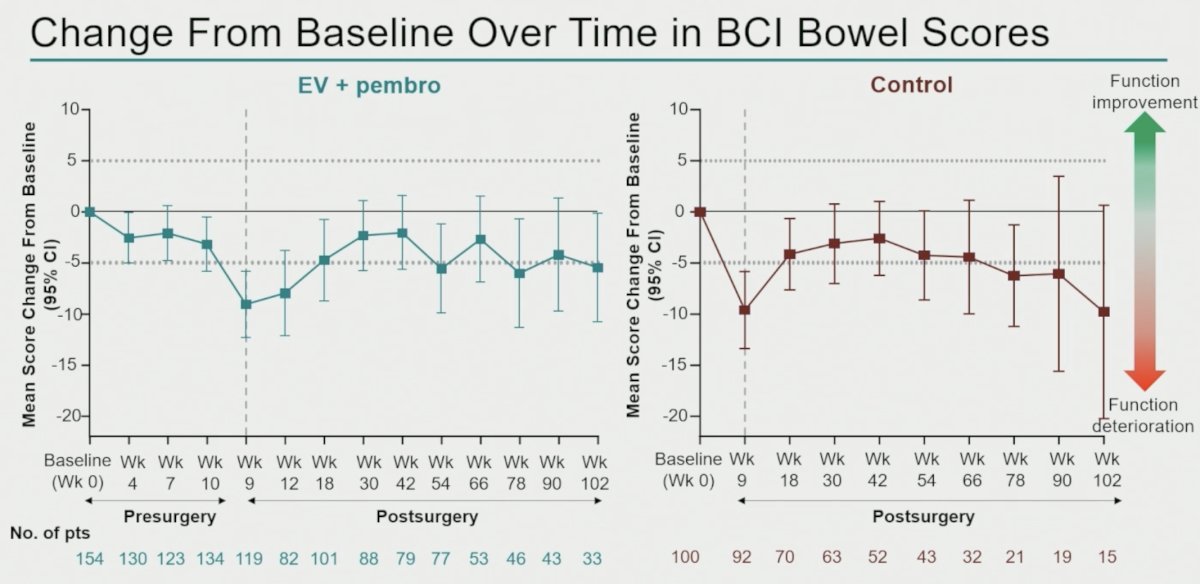
For bowel function:
- EV plus pembrolizumab: −4.75 (95% CI: −8.73 to −0.77)
- Control: −4.27 (95% CI: −7.93 to −0.61)
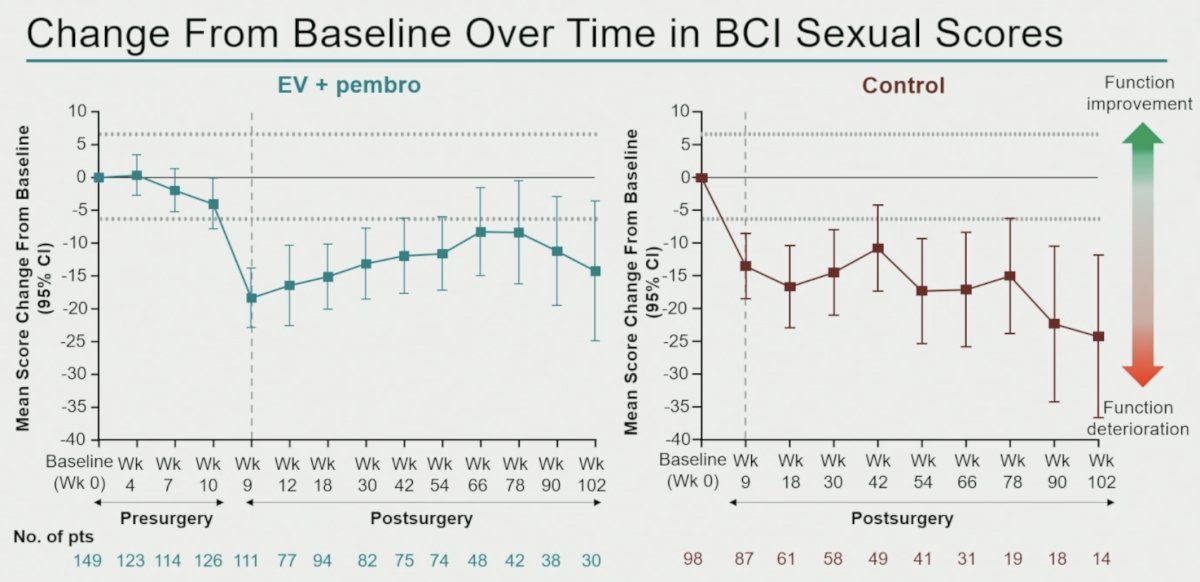
For sexual function:
- EV plus pembrolizumab: −15.46 (95% CI: −20.53 to −10.39)
- Control: −17.88 (95% CI: −24.36 to −11.40)
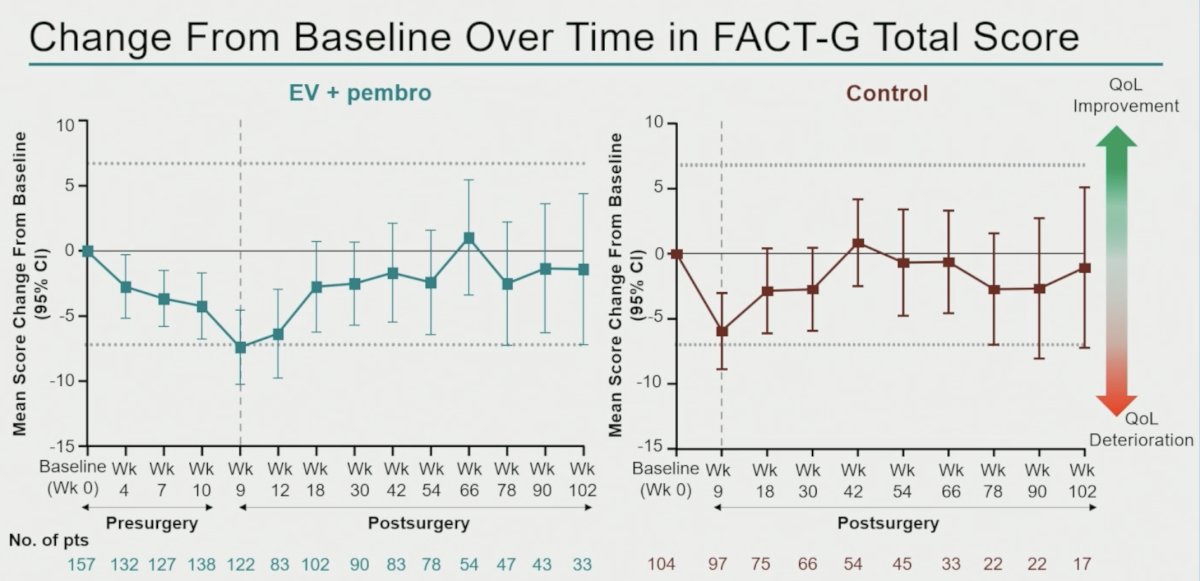
Longitudinal analyses demonstrated expected declines around the time of cystectomy, followed by recovery over time. For FACT-G, both treatment groups experienced the greatest deterioration around post-surgery week 9, after which scores improved toward baseline. Mean changes generally remained above the predefined threshold for clinically meaningful deterioration.
BCI urinary scores demonstrated an early postsurgical decline followed by recovery toward baseline in both groups. BCI bowel scores showed moderate deterioration after surgery with gradual recovery over follow-up. BCI sexual function demonstrated the greatest decline among BCI domains and remained persistently reduced over time in both arms, consistent with the known functional impact of radical cystectomy.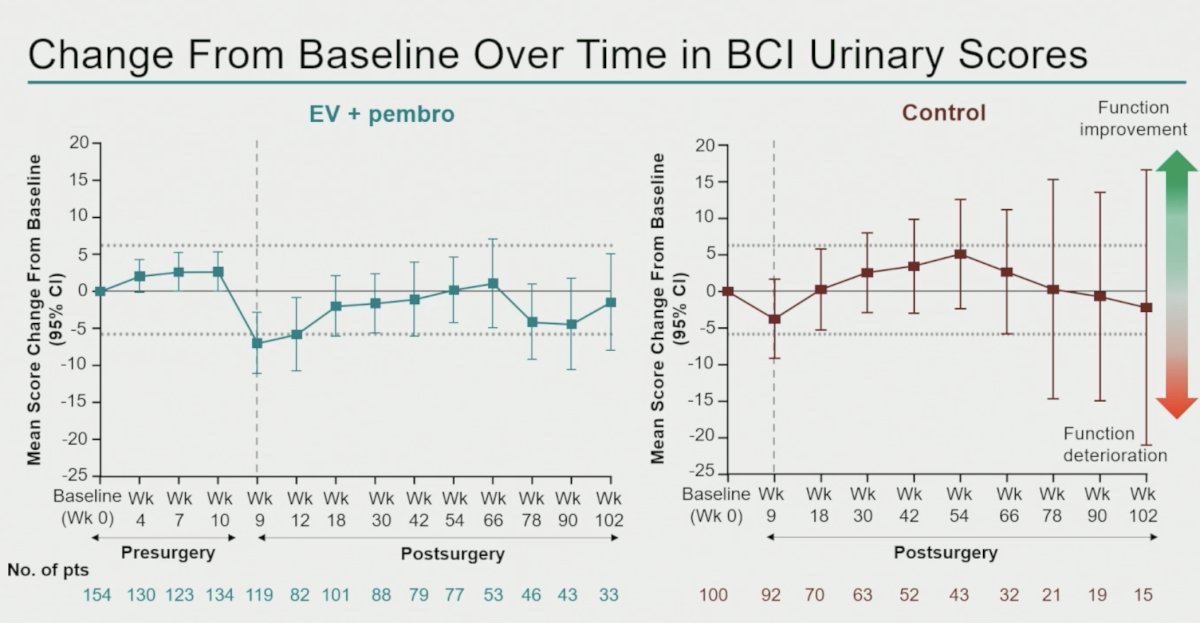
Dr. O'Donnell concluded with the following key takeaways:
- The addition of perioperative enfortumab vedotin plus pembrolizumab to radical cystectomy with standard pelvic lymph node dissection was associated with preservation of HRQoL over time relative to RC + PLND alone.
- Mean changes in general HRQoL, cystectomy-specific HRQoL, and overall health status did not exceed established thresholds for clinically meaningful deterioration.
- In this exploratory PRO analysis, perioperative EV plus pembrolizumab was not associated with a clinically meaningful detriment in general HRQoL, cystectomy-specific HRQoL, or overall health status.
- BCI bowel and sexual domains declined in both arms, consistent with the known functional impact of radical cystectomy.
- Together with the efficacy and safety results, these PRO findings support the overall benefit-risk profile of perioperative EV plus pembrolizumab for patients with MIBC who are cisplatin-ineligible.
Presented by: Peter H. O'Donnell, MD, Associate Professor, Medical Oncology, University of Chicago, Chicago, IL
Written by: Rashid K. Sayyid, MD, MSc, Assistant Professor, Urologic Oncologist, Department of Urology at The University of Arizona and Banner University Medical Center, Tucson, AZ – @rksayyid on X during the American Society of Clinical Oncology Genitourinary (ASCO) Annual Meeting held in Chicago, IL between May 29th and June 1st, 2026
Reference: