(UroToday.com) The 2026 American Society of Clinical Oncology (ASCO) Annual Meeting was host to a session on new approaches to curing bladder and kidney cancer. Dr. Nicholas James presented the feasibility and safety results from RAD-IO, a multi-stage trial of durvalumab plus chemoradiotherapy with 5-FU and mitomycin C in patients with muscle invasive bladder cancer (MIBC).
Bladder preservation with radical radiotherapy represents an established alternative to radical cystectomy for selected patients with MIBC. Building upon prior experience from BC2001 and other bladder-preservation studies, RAD-IO investigated whether the addition of neoadjuvant, synchronous, and adjuvant durvalumab to chemoradiotherapy could be safely delivered while improving oncologic outcomes. The study utilized a predefined go/no-go framework benchmarked against historical outcomes from BC2001, with a disease-free survival (DFS) rate ≥75% at 12 months considered sufficient to support further evaluation and a DFS rate <60% considered a no-go signal.
The study was conducted as a multi-stage platform trial. Stage 1 evaluated feasibility and safety, while Stage 2 assessed efficacy. Eligible patients had cT2–T4a urothelial carcinoma. Initial enrollment focused on patients with N0M0 disease, with subsequent expansion to include node-positive patients.
Stage 1 utilized a 2:1 randomization design comparing chemoradiotherapy plus durvalumab versus chemoradiotherapy alone. Randomization was stratified according to receipt of neoadjuvant chemotherapy. Due to the COVID-19 pandemic, patient enrolment was suspended, and upon re-activation, only re-enrolment to the investigational arm was possible, rendering RAD-IO effectively a single arm trial.
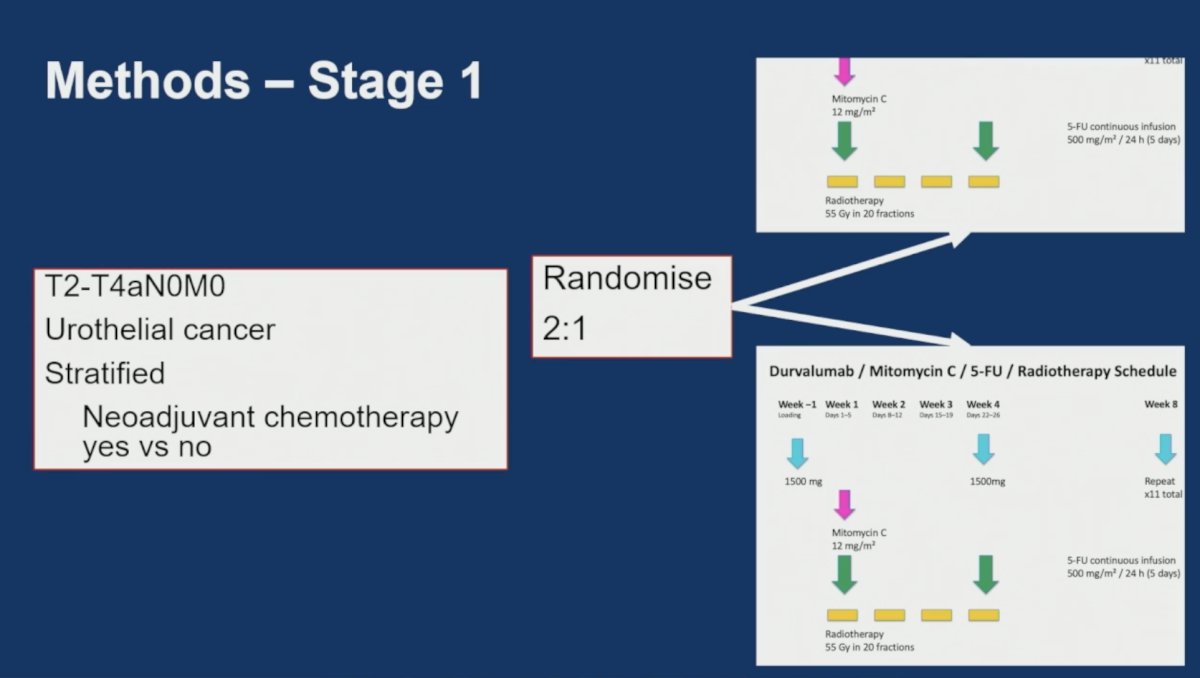
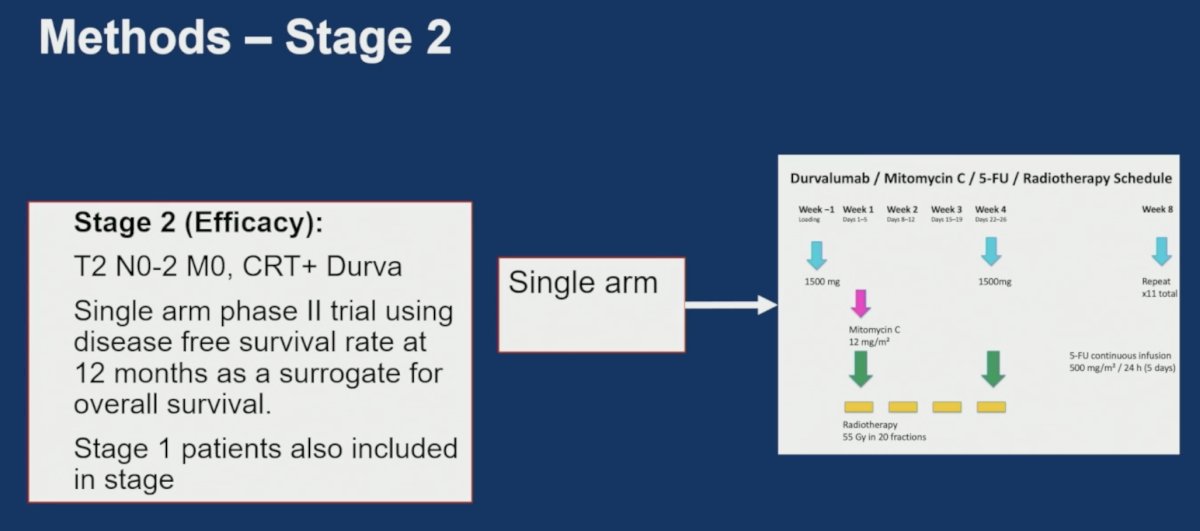
The chemoradiotherapy backbone was based on the BC2001 regimen. Patients received mitomycin C 12 mg/m² together with continuous-infusion 5-fluorouracil at 500 mg/m² per 24 hours for 5 days, administered concurrently with radiotherapy delivered to 55 Gy in 20 fractions.
In the investigational arm, durvalumab was administered at a loading dose of 1,500 mg prior to initiation of chemoradiotherapy, followed by additional 1,500 mg doses during treatment and continued every four weeks thereafter for a planned total of 11 maintenance doses. The treatment schema incorporated concurrent administration of durvalumab with mitomycin C, 5-fluorouracil, and radiotherapy.
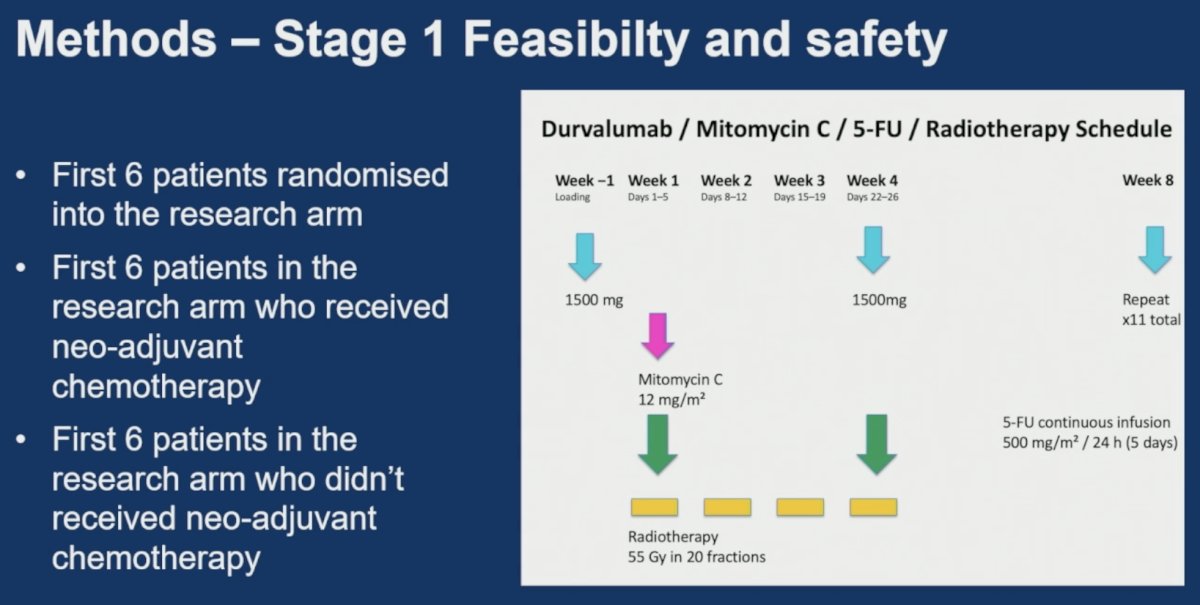
The Stage 1 feasibility component was deliberately conducted in sequential cohorts. Safety evaluation initially included:
- The first six patients randomized to the research arm
- The first six patients in the research arm who had received neoadjuvant chemotherapy
- The first six patients in the research arm who had not received neoadjuvant chemotherapy
Radiotherapy planning differed according to nodal status. For node-negative patients, treatment consisted of 55 Gy in 20 fractions directed to the bladder only. Representative planning images demonstrated bladder-targeted treatment volumes used in this cohort.
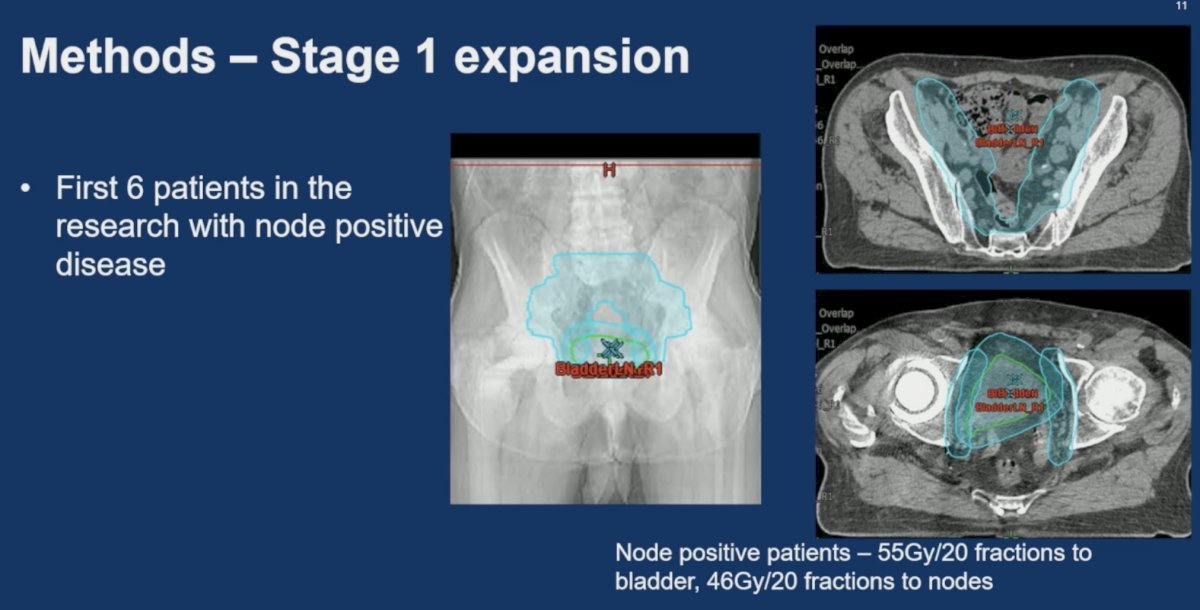
Following successful completion of the initial safety evaluation, Stage 1 expanded to include patients with node-positive disease. For these patients, radiotherapy consisted of 55 Gy in 20 fractions to the bladder with concurrent treatment of pelvic nodal regions to 46 Gy in 20 fractions. The presentation included radiotherapy planning images illustrating both bladder and pelvic nodal target volumes incorporated into the protocol.
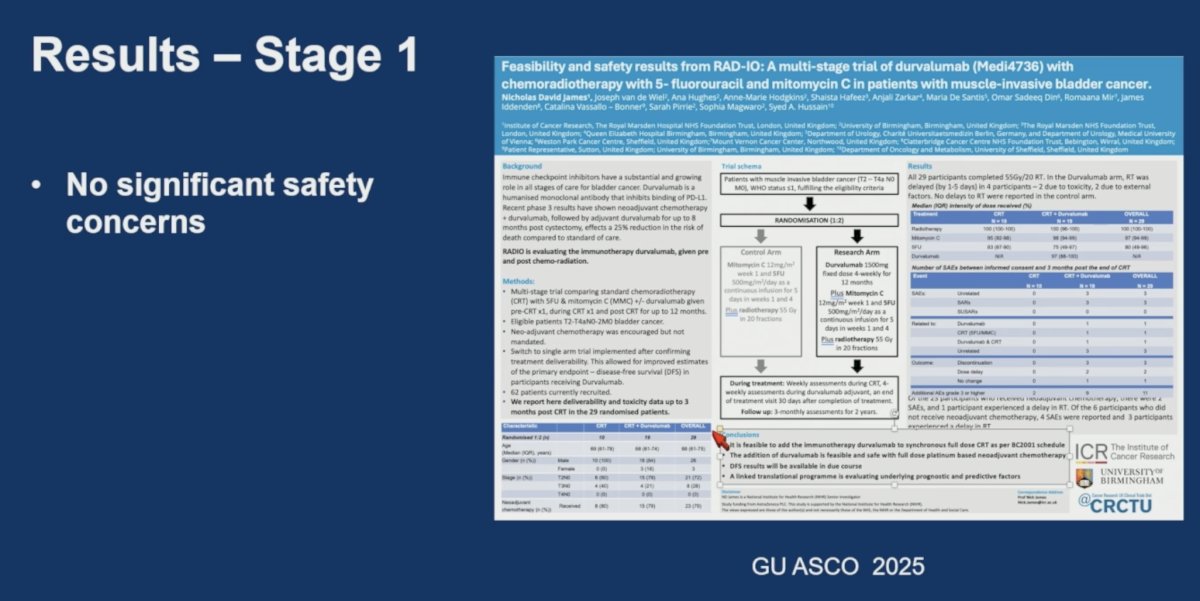
Early Stage 1 feasibility and safety results were previously presented at the 2025 ASCO Genitourinary Cancers Symposium. Dr. James highlighted that no significant safety concerns were identified during the safety run-in phase, supporting progression to the efficacy component of the study.
Following successful completion of Stage 1, the trial transitioned into Stage 2, which was designed as a single-arm phase II efficacy study evaluating chemoradiotherapy plus durvalumab. Patients with T2 N0–2 M0 disease were eligible, and patients enrolled during Stage 1 were incorporated into the Stage 2 efficacy analysis.
The primary endpoint for Stage 2 was disease-free survival (DFS) rate at 12 months following completion of chemoradiotherapy. The trial selected 12-month DFS as a surrogate endpoint for overall survival based on historical data from BC2001.
Disease-free survival was rigorously defined. Patients were considered disease-free only in the absence of:
- Distant metastases
- Locoregional nodal recurrence
- New muscle-invasive bladder tumors
- New non-muscle-invasive bladder tumors
- Upper tract urothelial carcinoma
- Death from bladder cancer
To guide interpretation of the efficacy results, investigators prospectively established a GO/NO-GO framework using 12-month DFS rates. A DFS rate ≥75% was considered a positive signal warranting further development of the regimen. A DFS rate <60% was considered insufficient activity and designated a NO-GO result. DFS rates between 60% and 75% were considered contextual and would require additional interpretation.
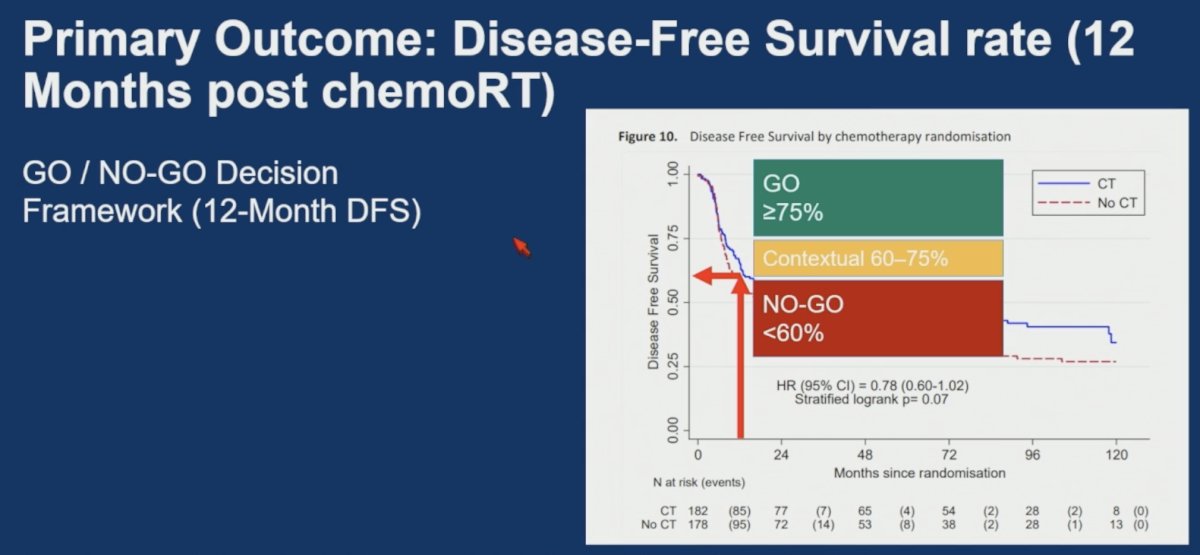
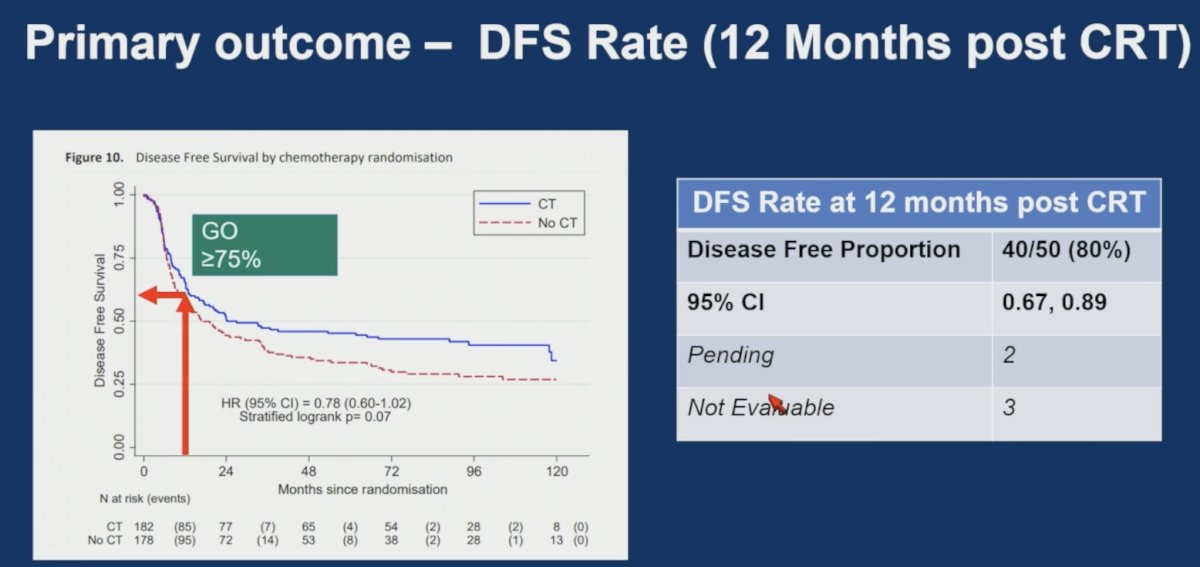
Historical BC2001 data served as the benchmark comparator throughout trial development. Dr. James reviewed the long-term BC2001 disease-free survival curve, which demonstrated a favorable effect of chemoradiotherapy compared with radiotherapy alone (HR 0.78, 95% CI 0.60–1.02; stratified log-rank p=0.07), providing the foundation upon which the RAD-IO study was built.
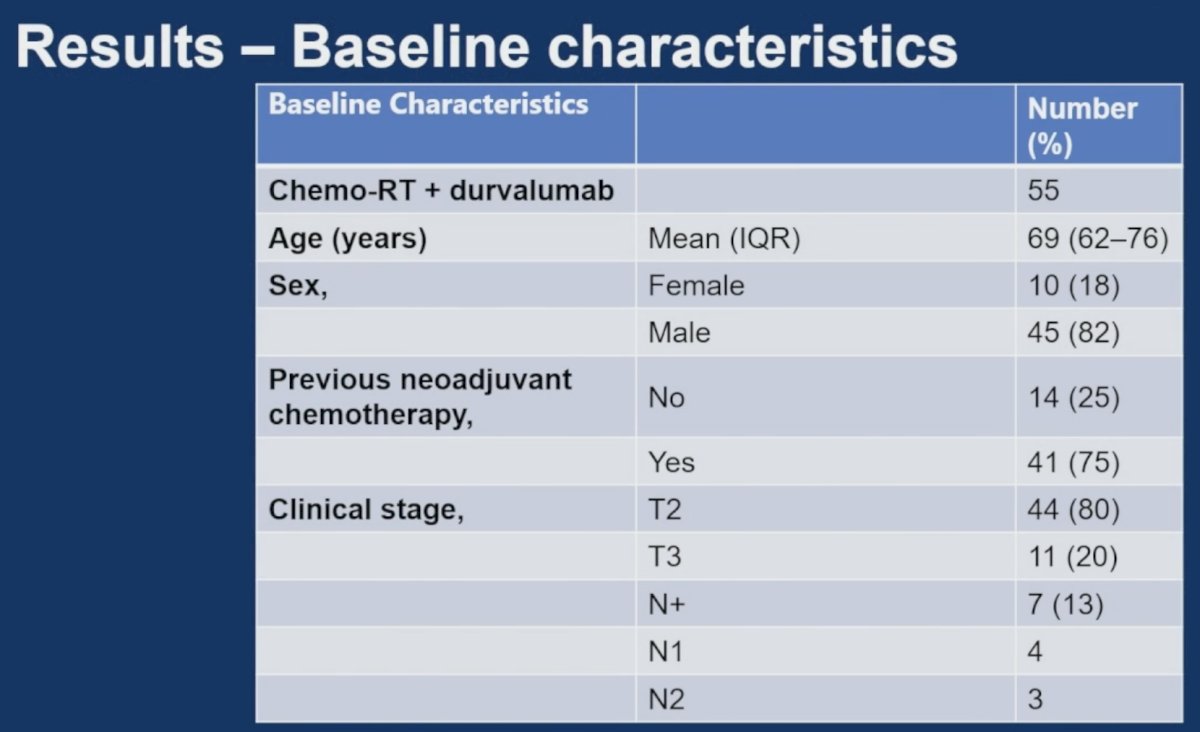
A total of 100 patients were included in the efficacy analysis. Baseline characteristics were balanced and reflected a typical bladder preservation population. The median age was approximately 75 years, most patients were male, and the majority had T2 disease. Approximately one-third of patients had received prior neoadjuvant chemotherapy. The efficacy cohort also included patients with node-positive disease enrolled during the Stage 1 expansion phase.
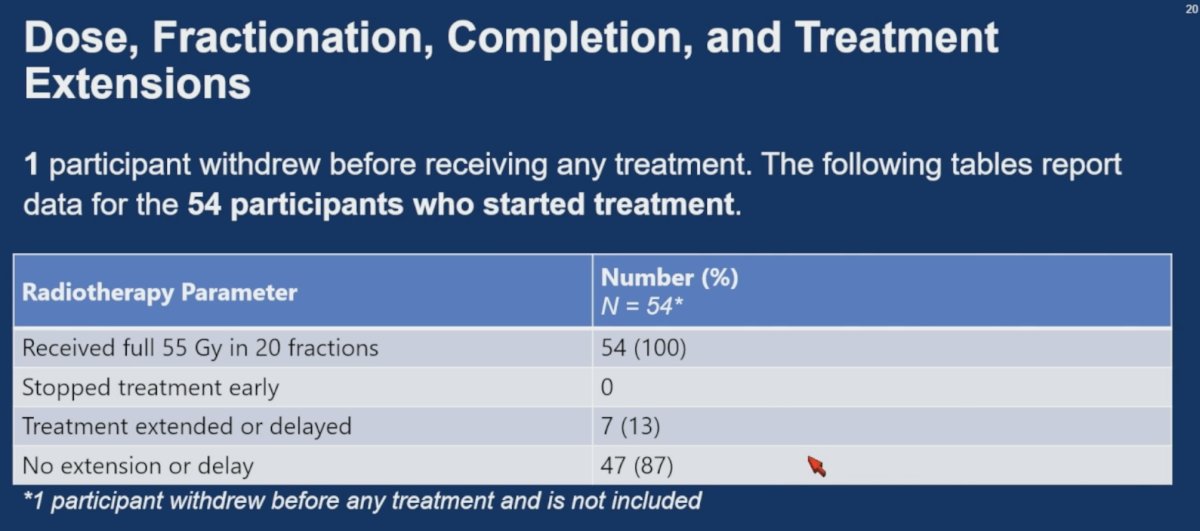
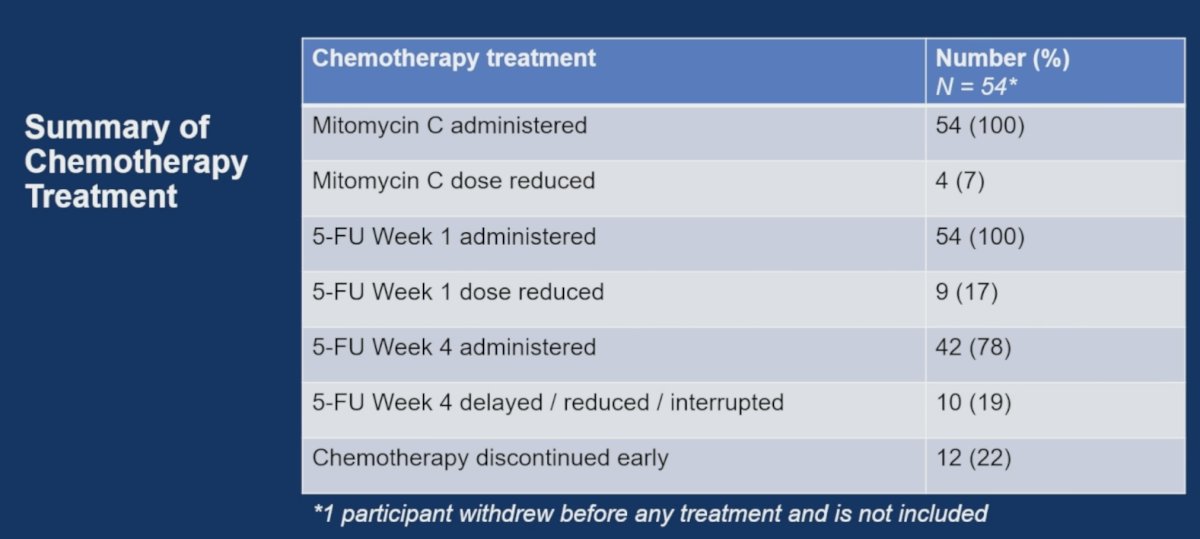
Treatment delivery was excellent across all modalities. Among the 55 enrolled patients, one withdrew prior to treatment initiation; therefore, treatment compliance analyses were based on 54 treated patients. All 54 treated patients (100%) successfully received the planned 55 Gy in 20 fractions, and no patients discontinued radiotherapy prematurely. Only 7 patients (13%) experienced a treatment extension or delay, while 47 patients (87%) completed radiotherapy without interruption.
Chemotherapy delivery was similarly favorable. All treated patients received mitomycin C, with dose reductions required in only 4 patients (7%). Week 1 5-fluorouracil was administered to all patients, although dose reductions were required in 9 patients (17%). Forty-two patients (78%) received the planned week 4 5-fluorouracil administration, while 10 patients (19%) required dose reduction, delay, or interruption. Overall, chemotherapy was discontinued early in 12 patients (22%).
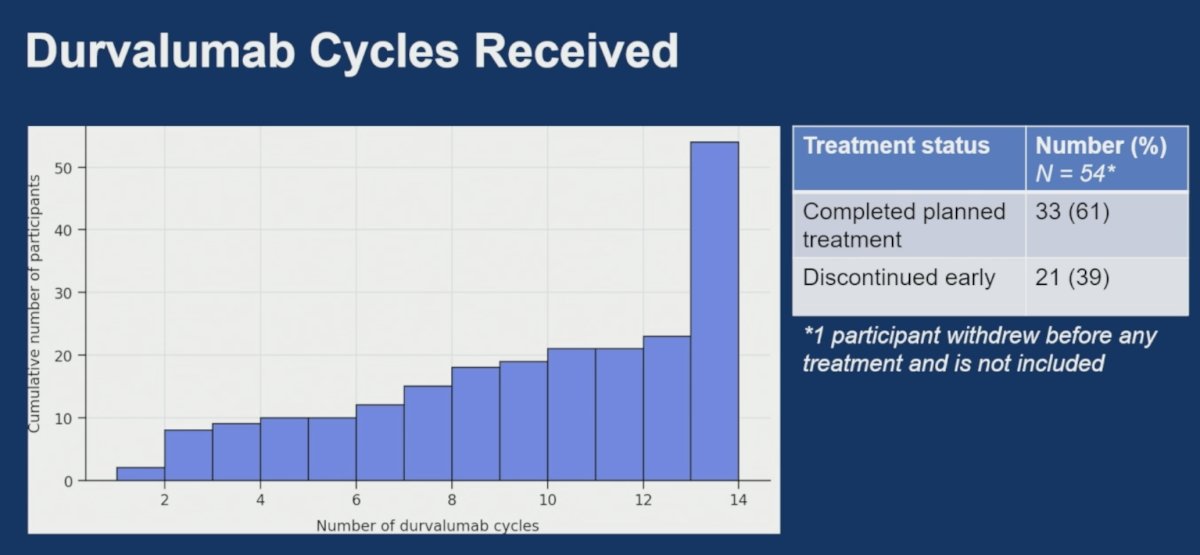
Durvalumab treatment exposure was also encouraging. Thirty-three of 54 treated patients (61%) completed the full planned course of durvalumab, while 21 patients (39%) discontinued treatment early.
The primary endpoint was successfully achieved. The observed 12-month disease-free survival rate (80% [40/50]; 95% CI 0.67–0.89) exceeded the prespecified efficacy threshold and met the GO criterion established by the protocol. The lower confidence interval remained above the NO-GO boundary, supporting further clinical development of the regimen.
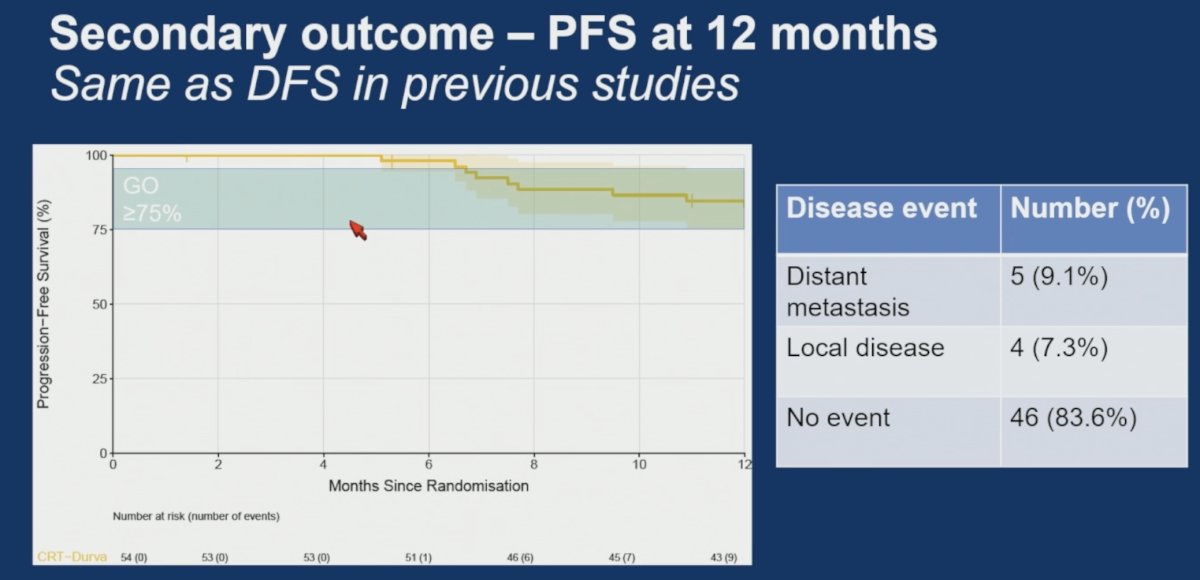
Overall, five patients (9.1%) developed distant metastases, and four (7.3%) had local disease recurrence.
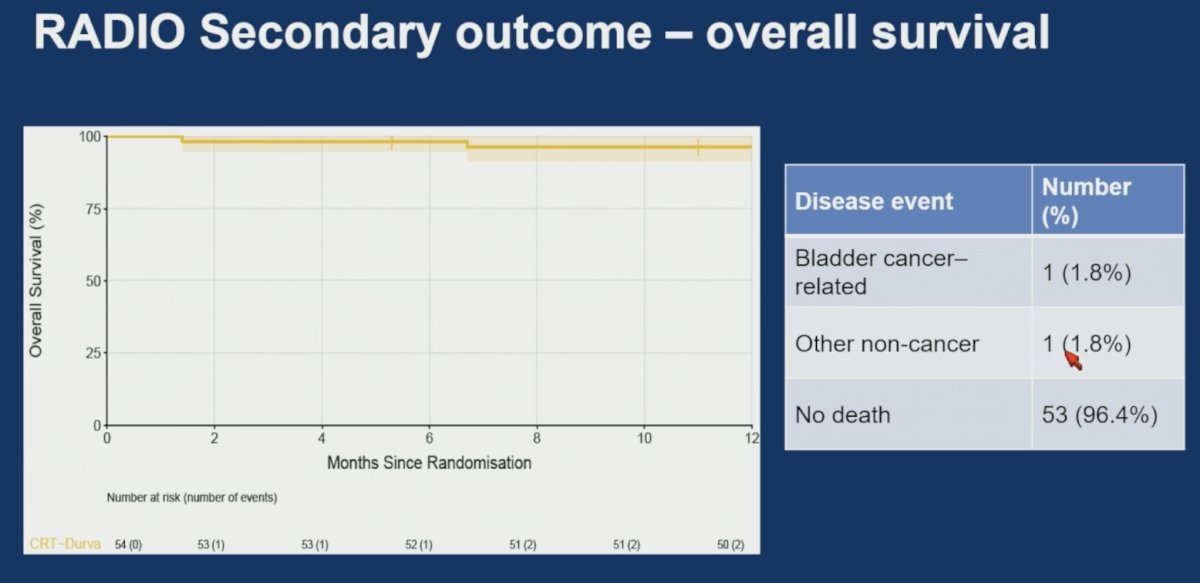
At the time of analysis, 96.4% of patients were alive, with 1 bladder cancer-related death (1 additional non-cancer related).
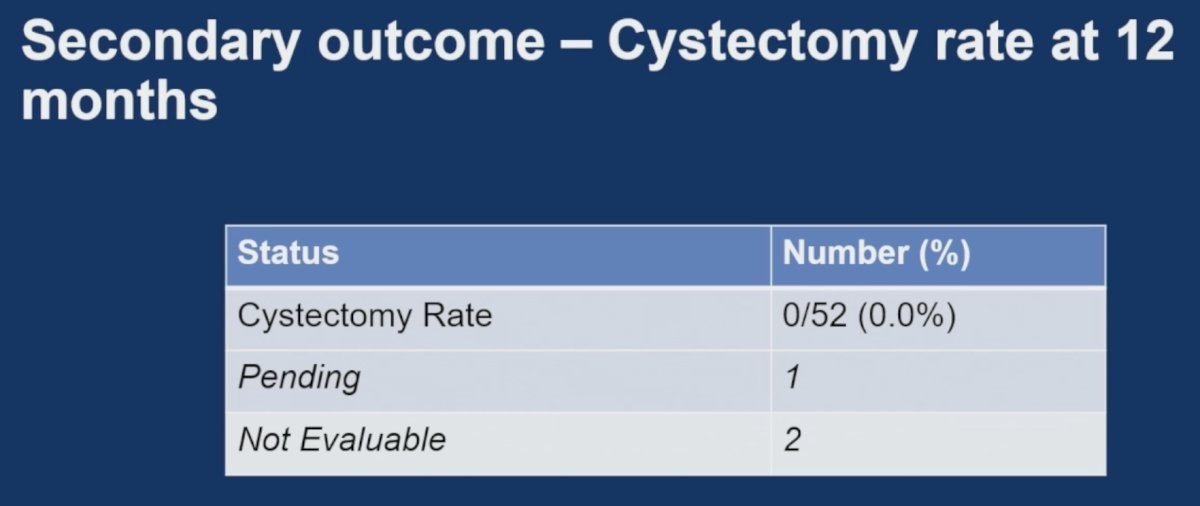
Notably, none of the patients required a cystectomy during the study follow up.
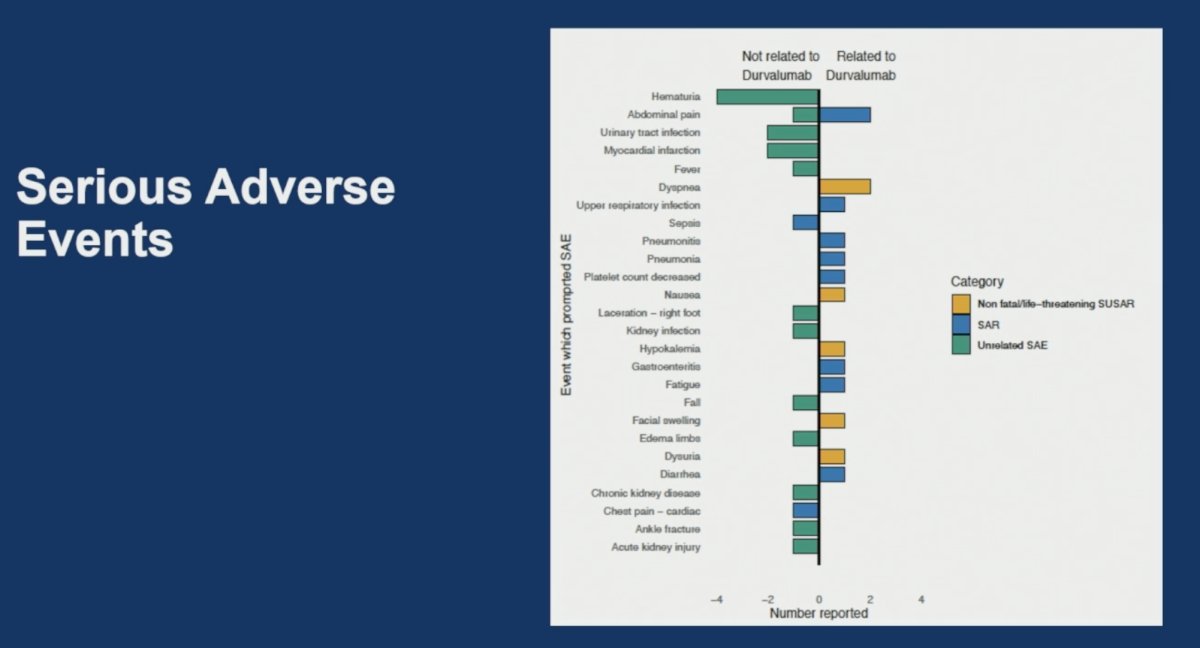
Dr. James noted that serious adverse events were relatively uncommon. Approximately half of reported serious adverse events (SAEs) were considered unrelated to durvalumab, with hematuria, urinary tract infection, myocardial infarction, falls, kidney infection, chronic kidney disease, and acute kidney injury among the most frequently reported unrelated events.
Treatment-related SAEs were infrequent and included abdominal pain, dyspnea, pneumonitis, pneumonia, upper respiratory infection, thrombocytopenia, gastroenteritis, fatigue, and diarrhea. A small number of non-fatal/non-life-threatening SUSARs were reported, including dyspnea, nausea, hypokalemia, facial swelling, dysuria, and diarrhea. Overall, no dominant toxicity signal emerged, and the observed serious adverse events were consistent with the established safety profile of durvalumab.
Dr. James acknowledged the following limitations:
- Non-randomized data but benchmarked against previous trial outcomes (BC-2001)
- Still to come
- Partially randomized comparison data from the feasibility phase
- 2-year outcomes
- Patient reported outcomes
Dr. James concluded his presentation of the RAD-IO trial as follows:
- Adding neoadjuvant, synchronous and adjuvant durvalumab is feasible and tolerable
- Adverse events in line with component parts of therapy – chemo-radiation and durvalumab
- Efficacy data met pre-set criteria for further evaluation benchmarked against our previous studies
- Very high bladder preservation rates
- Very high overall and disease-free survival versus previous trial data
Presented by: Nicholas James, MBBS, PhD, Professor of Prostate and Bladder Cancer Research at The Institute of Cancer Research and The Royal Marsden NHS Foundation Trust, London, UK
Written by: Rashid K. Sayyid, MD, MSc, Assistant Professor, Urologic Oncologist, Department of Urology at The University of Arizona and Banner University Medical Center, Tucson, AZ – @rksayyid on X during the American Society of Clinical Oncology Genitourinary (ASCO) Annual Meeting held in Chicago, IL between May 29th and June 1st, 2026
References:
- James ND, Hussain SA, Hall E, et al. Radiotherapy With or Without Chemotherapy in Muscle-Invasive Bladder Cancer. N Engl J Med. 2012;366(16):1477-1488.