(UroToday.com) The 2026 American Society of Clinical Oncology (ASCO) Annual Meeting was host to a kidney and bladder cancer oral abstract session. Dr. Gopa Iyer presented the initial results from NEXUS-01, a phase 1 study of LY4052031, an antibody-drug conjugate (ADC) targeting Nectin-4, in participants with advanced or metastatic urothelial carcinoma.
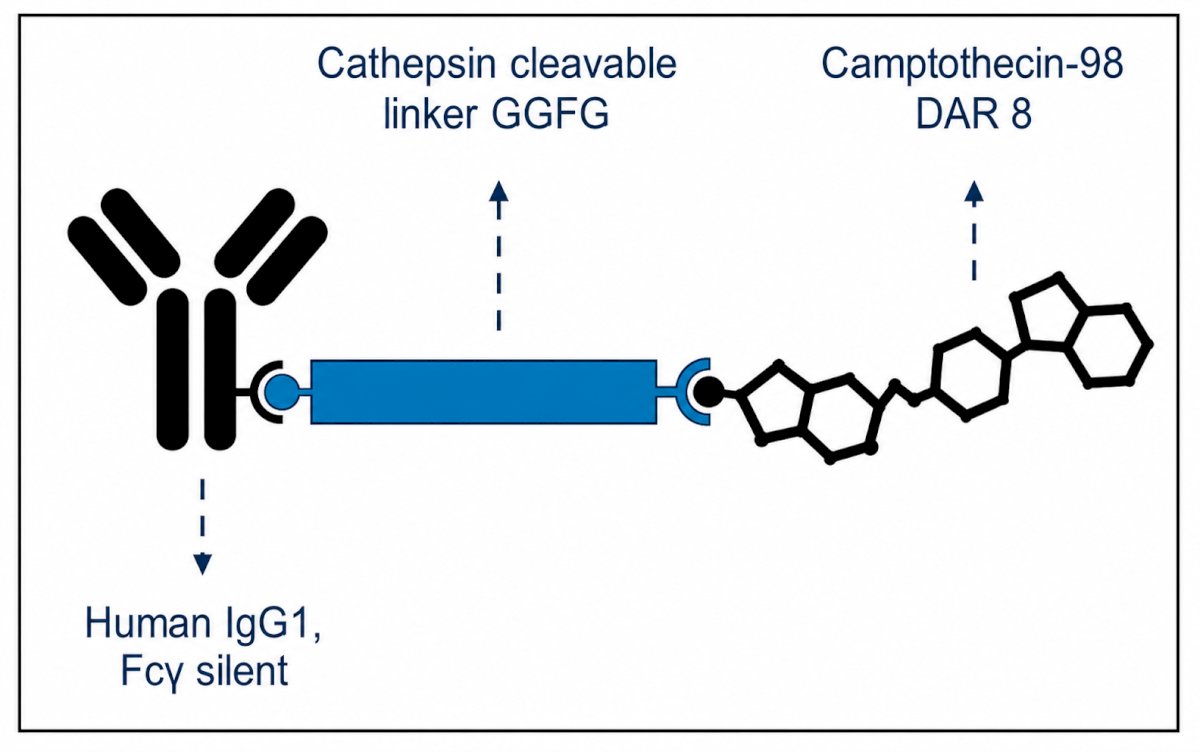
Enfortumab vedotin plus pembrolizumab (EV+P) has become the standard first-line therapy for locally advanced and metastatic urothelial carcinoma, firmly establishing Nectin-4 as a clinically relevant therapeutic target. However, treatment options following progression on EV+P are limited, and outcomes remain poor. Pre-clinical data suggest that resistance to enfortumab vedotin may be mediated by P-glycoprotein–driven payload efflux, supporting continued Nectin-4 targeting through ADCs employing alternative cytotoxic payloads. LY4052031 was therefore developed as a next-generation anti–Nectin-4 ADC consisting of a humanized IgG1 antibody linked via a cleavable peptide linker to a novel camptothecin-derived topoisomerase-I inhibitor payload (camp98), with a homogeneous drug-to-antibody ratio of 8. Importantly, clearance of camp98 is predominantly mediated through hepatic CYP2D6 metabolism, providing a rationale for pharmacogenomic-guided dose optimization.
NEXUS-01 was designed as a phase 1a dose-escalation and dose-optimization study utilizing every-3-week dosing. The trial included two principal cohorts. Cohort A1 enrolled patients with metastatic urothelial carcinoma and selected Nectin-4–expressing solid tumors into a Bayesian Optimal Interval Design (BOIN)-based dose-escalation strategy ranging from 0.6 mg/kg to 5.4 mg/kg. Cohort A2 subsequently randomized patients with mUC to four dose levels: 2.4 mg/kg, 3.6 mg/kg, 4.2 mg/kg, and 4.8 mg/kg. Key eligibility criteria included ECOG performance status 0–1, advanced or metastatic Nectin-4–expressing tumors, and allowance for prior enfortumab vedotin exposure. Primary objectives included determination of the optimal dose, safety and tolerability, pharmacokinetics, and preliminary efficacy by RECIST v1.1.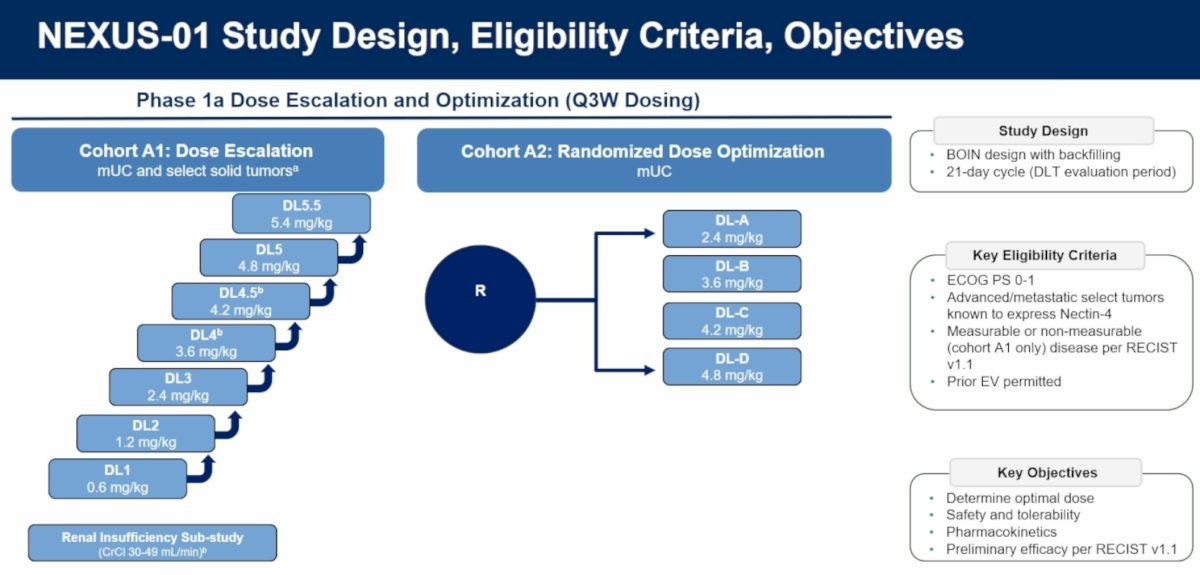
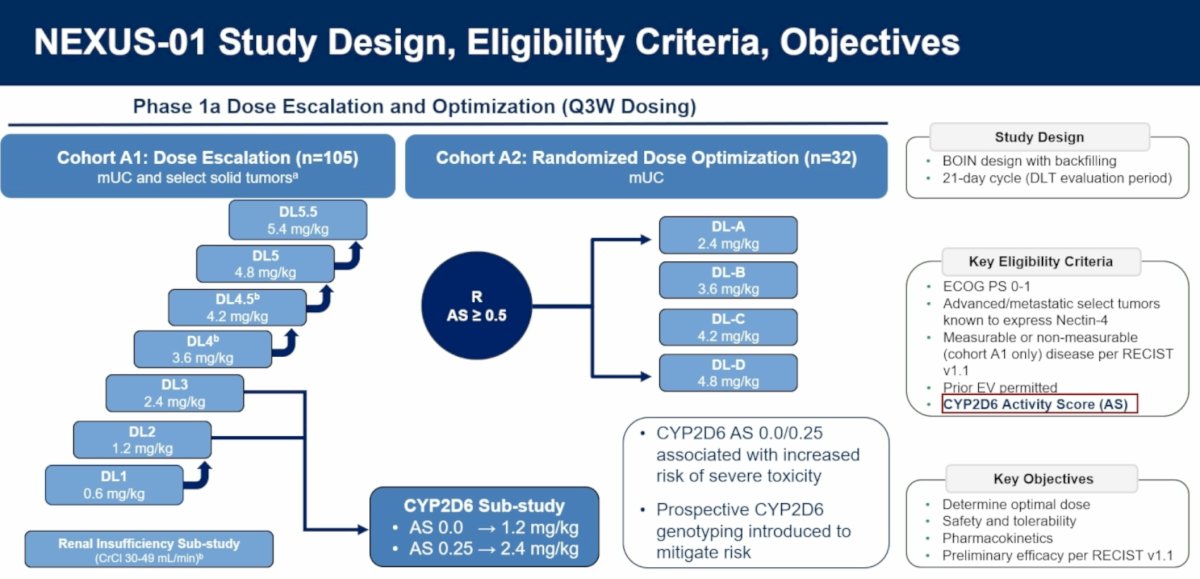
As clinical experience accumulated, the investigators observed that severe toxicities clustered among patients with reduced CYP2D6 activity. Consequently, prospective CYP2D6 genotyping was incorporated into the study. Patients with an activity score (AS) of 0.0 received 1.2 mg/kg, whereas those with an AS of 0.25 received 2.4 mg/kg as part of a dedicated pharmacogenomic substudy. Participants with AS 0.0 or 0.25 had demonstrated an increased risk of severe toxicity due to reduced payload clearance.
At the April 29, 2026, data cutoff, 137 participants had been treated, including 107 patients with metastatic urothelial carcinoma. The median age was 67 years (range 31–86 years), and 60% had ECOG performance status 1. Among all participants, CYP2D6 activity scores were 0.0 in 3%, 0.25 in 4%, and ≥0.5 in 89%. Within the mUC cohort, the disease burden was substantial: 59% had visceral metastases, including liver metastases in 31%, and patients had received a median of three prior systemic therapies (range 1–9). Prior treatments included platinum chemotherapy in 88%, enfortumab vedotin with or without pembrolizumab in 67%, EV+P specifically in 39%, immune checkpoint inhibitors in 94%, and prior topoisomerase-I ADCs in 23%.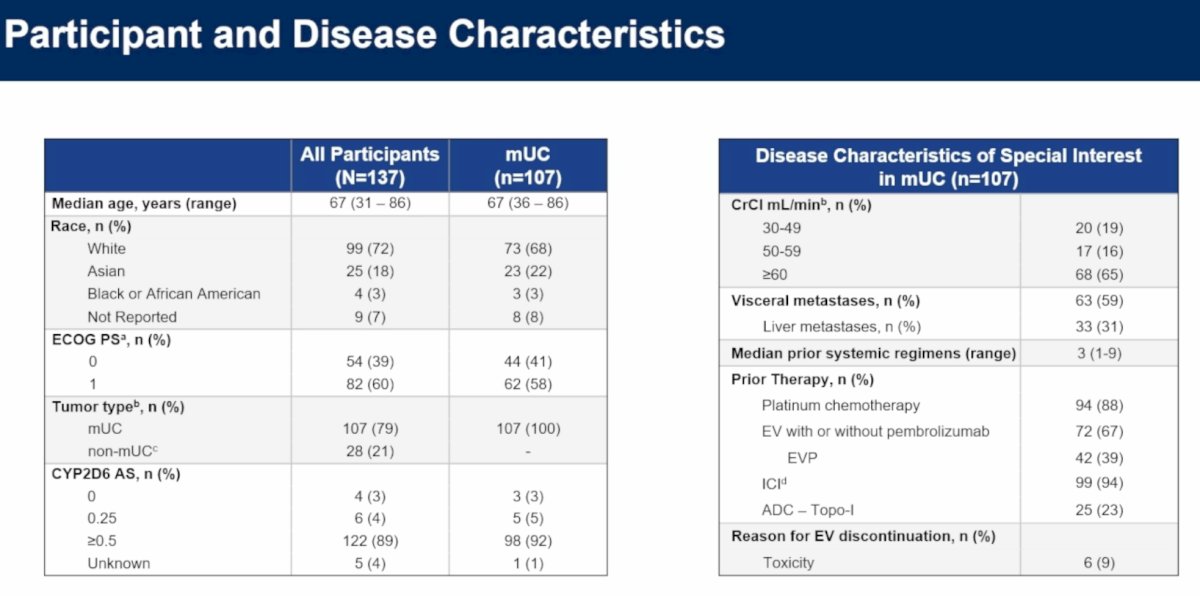
Safety analyses demonstrated a generally favorable toxicity profile. Across all treated patients, 47% remained on therapy at data cutoff. The most common treatment-emergent adverse events (TEAEs) were alopecia (38%), nausea (38%), dysgeusia (35%), fatigue (31%), and anemia. Most events were grade 1–2 in severity. Notably, adverse events commonly associated with enfortumab vedotin—including skin toxicity, peripheral neuropathy, ocular toxicity, and hyperglycemia—were uncommon. Diarrhea was infrequent and predominantly low grade.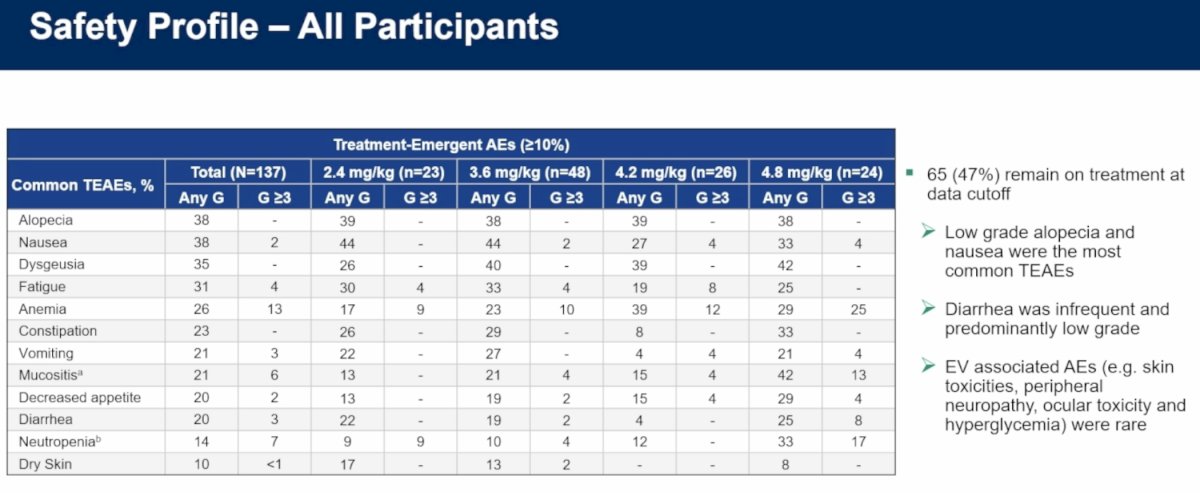
Among patients with CYP2D6 activity scores ≥0.5 (n=122), tolerability was particularly encouraging. Fifty percent remained on treatment at data cutoff. Grade 4 adverse events were uncommon, occurring in only 3 patients (2.5%), including neutropenia and white blood cell count decrease. Dose reductions due to adverse events occurred in 13% of patients, and treatment discontinuations in only 3%. Even at higher dose levels, neutropenia remained relatively uncommon and was predominantly low grade.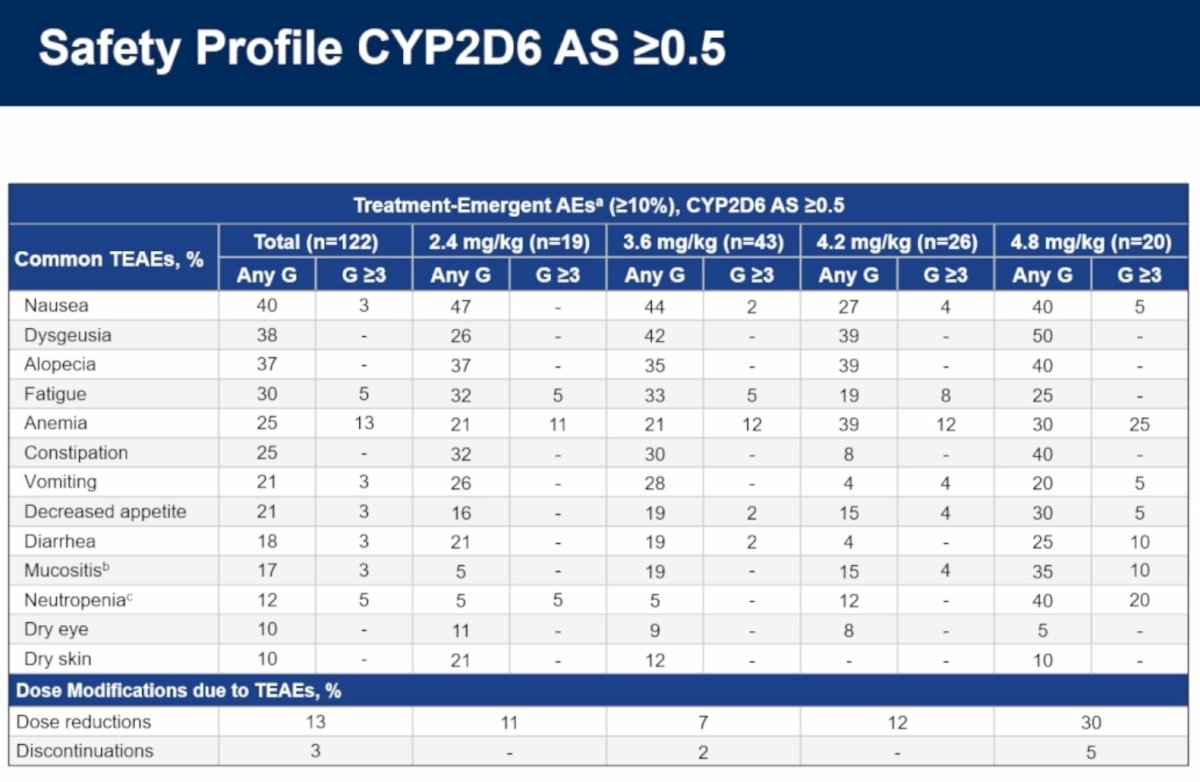
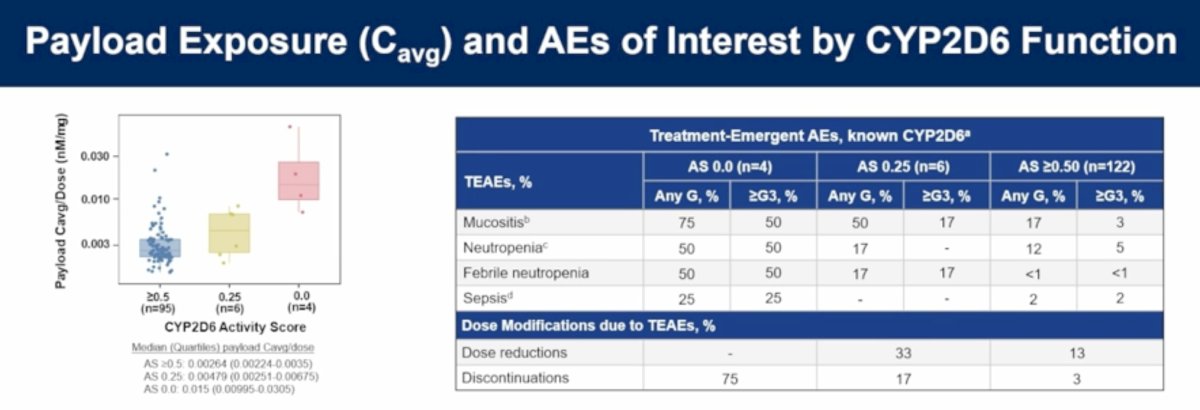
Pharmacokinetic analyses highlighted the importance of CYP2D6 metabolism. Patients with poor or minimal CYP2D6 function (AS 0.0 or 0.25) demonstrated substantially higher payload exposure and correspondingly increased risks of severe toxicity. Rates of mucositis, neutropenia, febrile neutropenia, and sepsis were markedly higher among these patients compared to individuals with activity scores ≥0.5. Dose reductions occurred in 33% of patients with AS 0.25, and treatment discontinuations occurred in 75% and 17% of patients with AS 0.0 and AS 0.25, respectively, compared with only 3% among those with AS ≥0.5. Three treatment-related deaths were reported, including aspiration pneumonia in a patient with AS 0.25, sepsis in a patient with AS 0.0, and another participant with unknown CYP2D6 status. These findings prompted the implementation of prospective germline genotyping and activity score–based dose optimization.
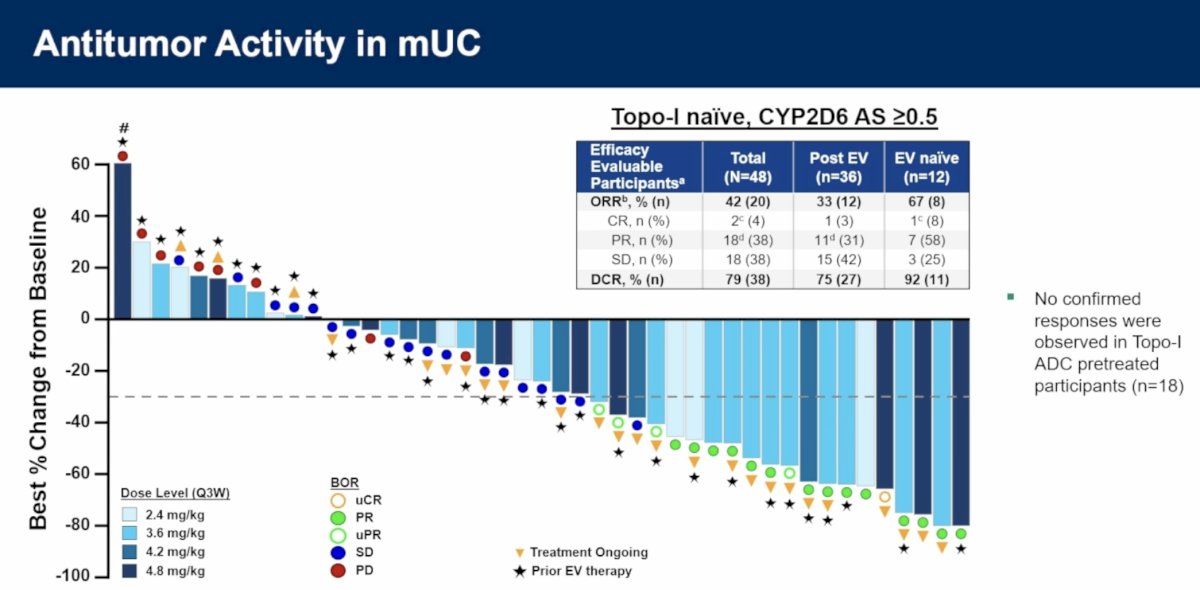
Preliminary antitumor activity was particularly notable among patients with metastatic urothelial carcinoma who were topoisomerase-I ADC naïve and had CYP2D6 activity scores ≥0.5. Among 48 efficacy-evaluable patients, the overall response rate (ORR) was 42% (20/48), including confirmed complete responses in 4% and partial responses in 38%. The disease control rate (DCR) was 79% (38/48). Responses were observed regardless of prior enfortumab vedotin exposure. Among patients previously treated with EV (n=36), ORR was 33% (12/36), and DCR was 75% (27/36). In EV-naïve patients (n=12), ORR reached 67% (8/12) with a DCR of 92% (11/12). Importantly, no confirmed responses were observed among the 18 patients previously exposed to a topoisomerase-I ADC, suggesting potential payload-class cross-resistance.
Durability analyses further supported clinical activity. Among EV-pretreated, topoisomerase-I ADC–naïve patients with CYP2D6 activity scores ≥0.5, the median duration of response was 7.4 months (95% CI: 2.7–not estimable) among nine confirmed responders. Notably, 67% of responding patients remained on treatment at the time of analysis, indicating ongoing disease control in many responders.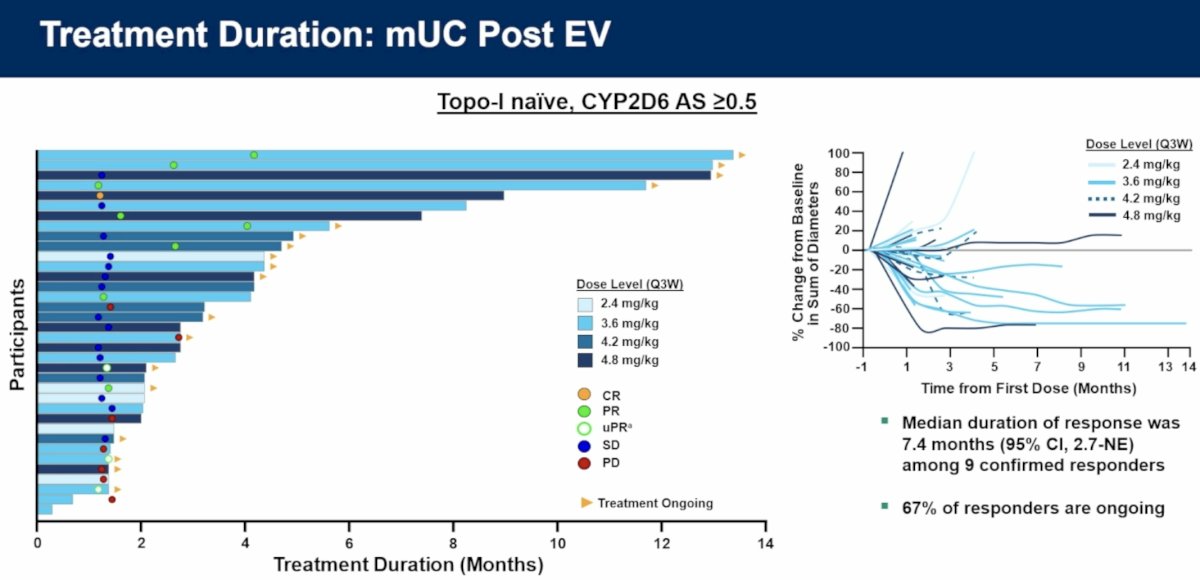
Dr. Iyer concluded as follows:
- LY4052031 demonstrated promising clinical activity across multiple dose levels, suggesting Nectin-4 remains an important therapeutic target following progression on EV-based therapy
- 42% (20/48) ORR and 79% DCR in EV-naïve and pretreated mUC
- 33% (12/36) ORR, 75% (27/36) DCR, and a median DoR of 7.4 months in EV-pretreated mUC
- LY4052031 was generally well-tolerated, and the most common TEAEs were grades 1–2
- Among participants with CYP2D6 AS ≥0.5, LY4052031 showed a favorable tolerability profile with low rates of myelosuppression and diarrhea. Dose reductions (13%) and discontinuations (3%) due to AEs were uncommon
- No or minimal CYP2D6 function (AS 0.0–0.25) was associated with increased risk of severe toxicity, most notably neutropenia. Risk mitigation with prospective germline genotyping has been implemented
- CYP2D6 AS-specific dose optimization is ongoing
The key takeaway points from this study were:
- LY4052031, a next-generation Nectin-4 ADC incorporating a novel topoisomerase-I payload, demonstrated meaningful antitumor activity in metastatic urothelial carcinoma, including patients previously treated with enfortumab vedotin.
- Among topoisomerase-I ADC–naïve patients with CYP2D6 activity scores ≥0.5, ORR was 42% overall, including 33% in EV-pretreated patients and 67% in EV-naïve patients, with a DCR of 79%.
- LY4052031 exhibited a favorable safety profile, with predominantly grade 1–2 toxicities and low rates of dose reductions (13%) and treatment discontinuations (3%).
- Reduced CYP2D6 activity was associated with increased payload exposure and substantially higher risks of severe toxicity, supporting prospective CYP2D6 genotyping and pharmacogenomic-guided dose optimization as an integral component of future development.
Presented by: Gopa Iyer, MD, Medical Oncology, Memorial Sloan Kettering Cancer Center, New York, NY, USA
Written by: Rashid K. Sayyid, MD, MSc, Assistant Professor, Urologic Oncologist, Department of Urology at The University of Arizona and Banner University Medical Center, Tucson, AZ – @rksayyid on X during the American Society of Clinical Oncology Genitourinary (ASCO) Annual Meeting held in Chicago, IL between May 29th and June 1st, 2026