(UroToday.com) The 2026 American Society of Clinical Oncology (ASCO) Annual Meeting was host to a kidney and bladder cancers oral abstract session. Dr. Thomas Powles presented 3.5-year follow-up data and response analyses from the phase 3 EV-302 study evaluating enfortumab vedotin + pembrolizumab (EV+P) for previously untreated locally advanced or metastatic urothelial carcinoma.
EV-302/KEYNOTE-A39 previously established EV+P as the preferred first-line standard of care for patients with advanced urothelial carcinoma after demonstrating significant improvements in progression-free survival (PFS) and overall survival (OS) compared to platinum-based chemotherapy.1 While earlier analyses established the superiority of EV+P, longer-term follow-up remains important to determine whether survival benefits are maintained, whether deep responses continue to mature over time, and whether the safety profile remains manageable with prolonged treatment exposure.
The current analysis evaluated efficacy and safety outcomes in the intention-to-treat (ITT) population after a median follow-up of 42.8 months. In addition, exploratory analyses focused on patients who achieved complete responses, including those whose responses deepened from a partial response (PR) to a complete response (CR), as well as patients who remained on treatment for more than one or two years.
EV-302 enrolled 886 patients with previously untreated locally advanced or metastatic urothelial carcinoma. Eligible patients were PD-(L)1 inhibitor naïve, had an ECOG performance status ≤2, and were eligible for both EV and pembrolizumab. Patients were randomized 1:1 to:
- Enfortumab vedotin plus pembrolizumab is administered until progression
- Platinum-based chemotherapy (gemcitabine plus cisplatin or carboplatin) for a maximum of six cycles
- Randomization was stratified according to cisplatin eligibility, PD-L1 expression, and presence of liver metastases
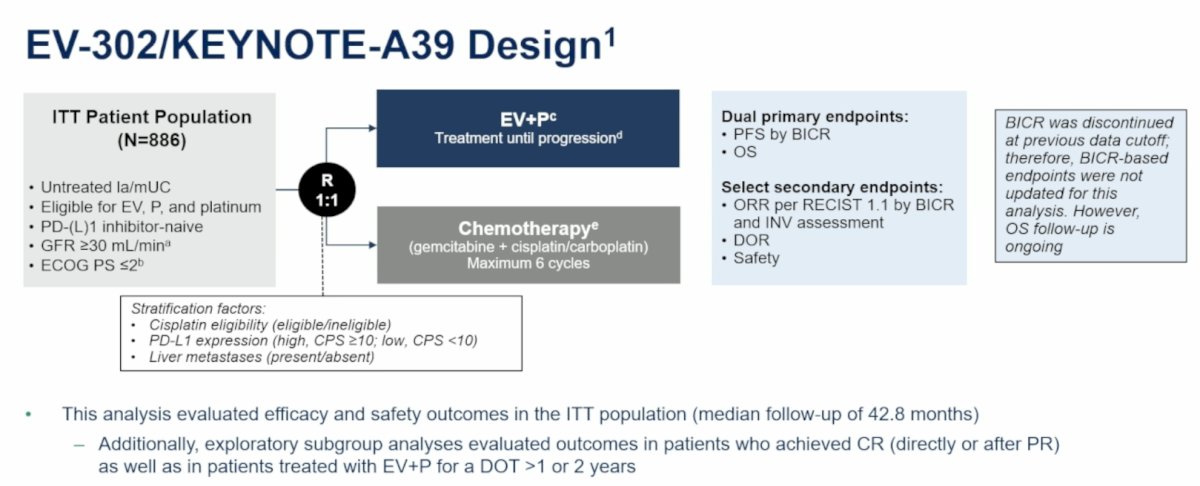
The dual primary endpoints were PFS by blinded independent central review (BICR) and OS. Secondary endpoints included objective response rate (ORR), duration of response (DOR), and safety.
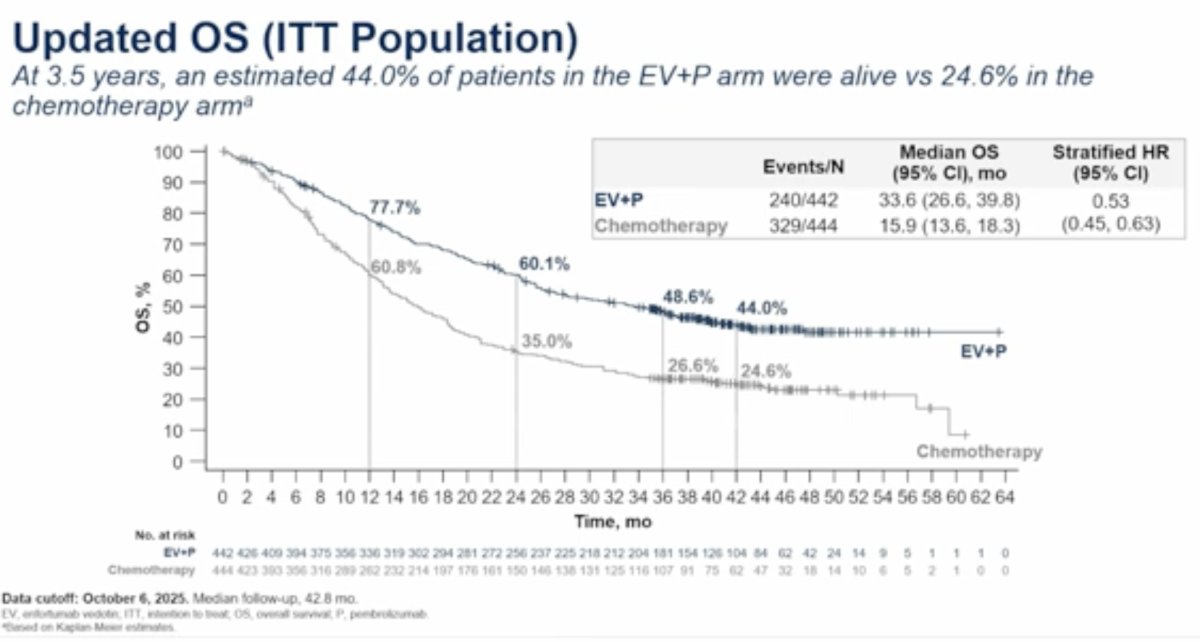
At the October 2025 data cutoff, EV+P continued to demonstrate a substantial and durable OS benefit. The median OS was 33.6 months (95% CI: 26.6–39.8) with EV+P, compared to 15.9 months (95% CI: 13.6–18.3) with chemotherapy, corresponding to a 47% reduction in the risk of death (HR: 0.53, 95% CI: 0.45–0.63). At approximately 3.5 years, nearly 50% of patients treated with EV+P remained alive compared to only one-quarter of those treated with chemotherapy.
Dr. Powles and colleagues also examined subsequent therapies following protocol treatment. In the EV+P arm, 43.4% of patients subsequently received additional anticancer therapy, and 39.1% received systemic therapy. The most common first subsequent treatment was platinum-containing chemotherapy, administered to 135 patients (30.5%), including carboplatin-based therapy in 16.5% and cisplatin-based therapy in 13.8%.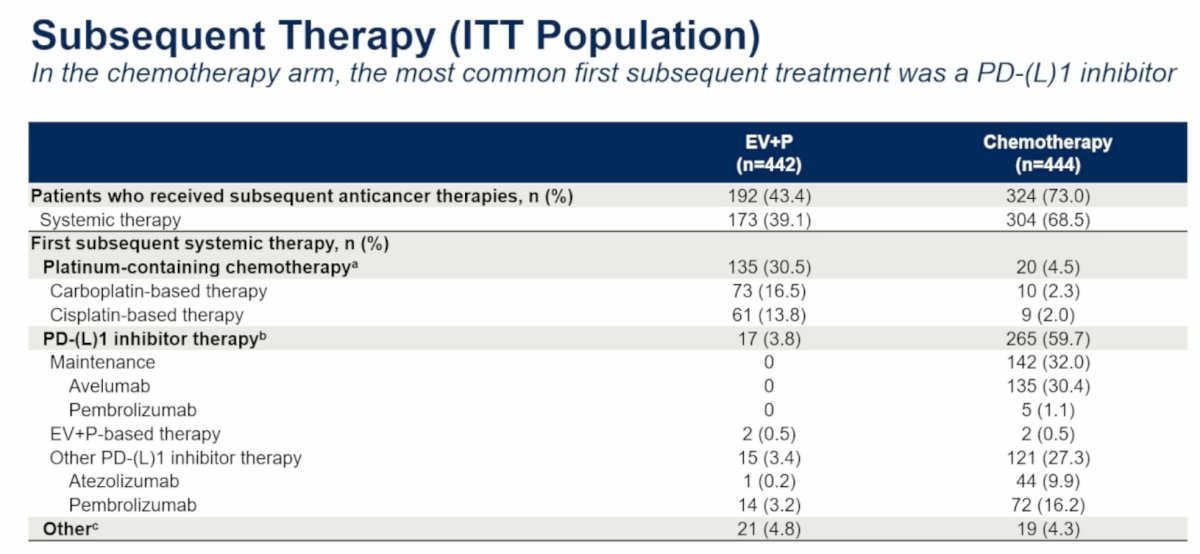
Importantly, subsequent platinum-based chemotherapy remained clinically active after frontline EV+P. Among evaluable patients receiving platinum-based chemotherapy:
- ORR was 20.7% (28/135) overall
- ORR was 19.7% with cisplatin-based therapy
- ORR was 21.9% with carboplatin-based therapy
The median OS from initiation of subsequent platinum chemotherapy was 10.9 months (95% CI: 8.3–12.8).
In contrast, among patients initially treated with chemotherapy, 73% received subsequent anticancer therapy, and 68.5% received systemic therapy. The most common first subsequent treatment was PD-(L)1 inhibitor therapy, administered to 59.7% of patients, including maintenance avelumab in 32%.
Updated response analyses continued to favor EV+P. Among response-evaluable patients, ORR was 67.5% (295/437) with EV+P compared to 44.2% (195/441) with chemotherapy. The corresponding CR proportions were 30.4% and 14.5%, respectively.
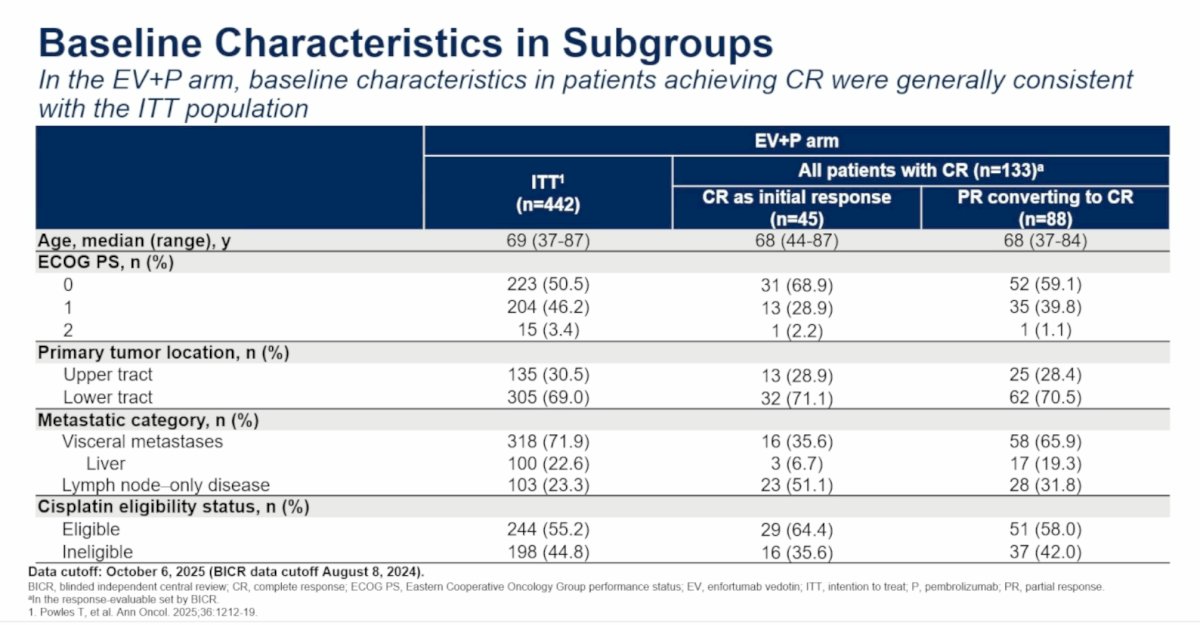
Importantly, among the 133 patients (30.4%) achieving a CR with EV+P, 45 (10.3% overall) achieved a CR as their initial response, with an additional 88 patients (20.1%) initially achieving a PR and subsequently converting into a CR.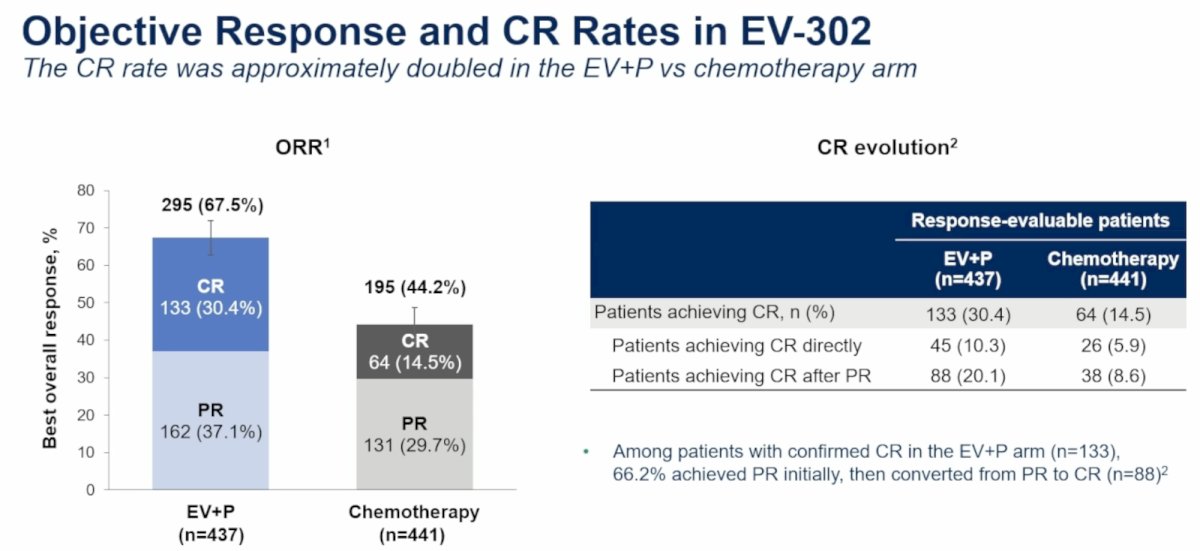
The baseline characteristics among patients who achieved a CR were generally similar to those of the overall EV+P population. However, patients achieving a CR tended to have fewer visceral metastases and more lymph node-only disease. Among patients who achieved CR directly, only 35.6% had visceral metastases, compared with 71.9% in the overall ITT population.
With regards to the median time to CR in the EV+P arm, among all patients who achieved a CR, the median time to CR was 4.3 months (IQR: 2.2–8.4). For patients converting from PR to CR, the median time to initial PR was only 2.1 months (IQR: 1.9–2.2), while the median time to eventual CR was 6.6 months (IQR: 4.3–12.1). These findings suggest that many patients continue to deepen their responses well beyond the first radiographic assessment.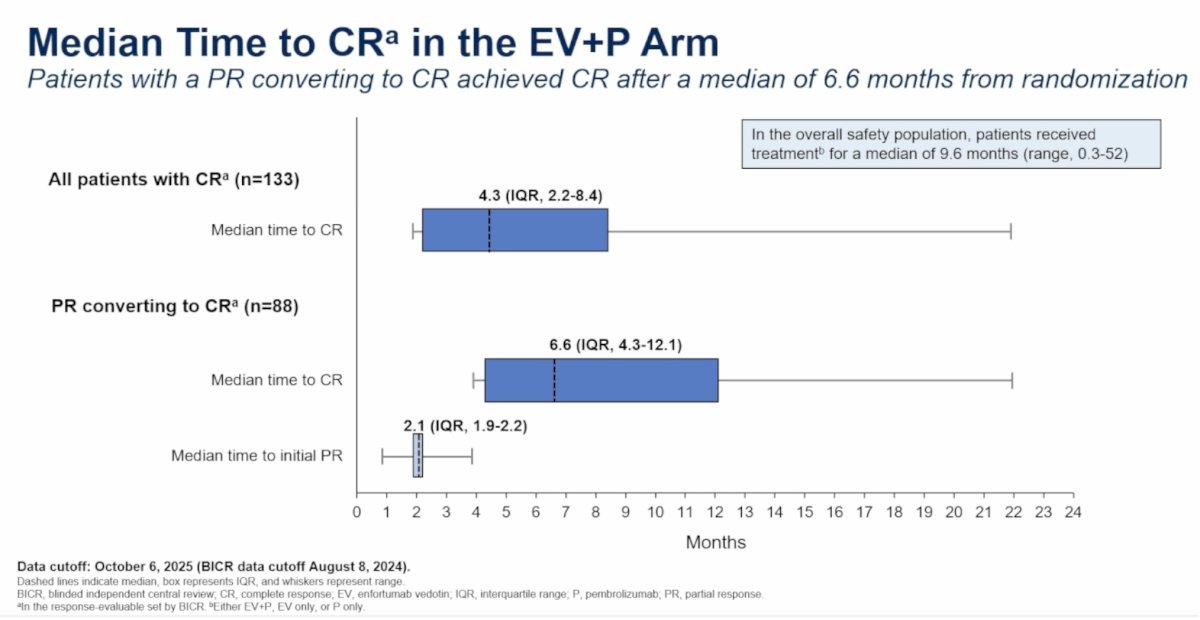
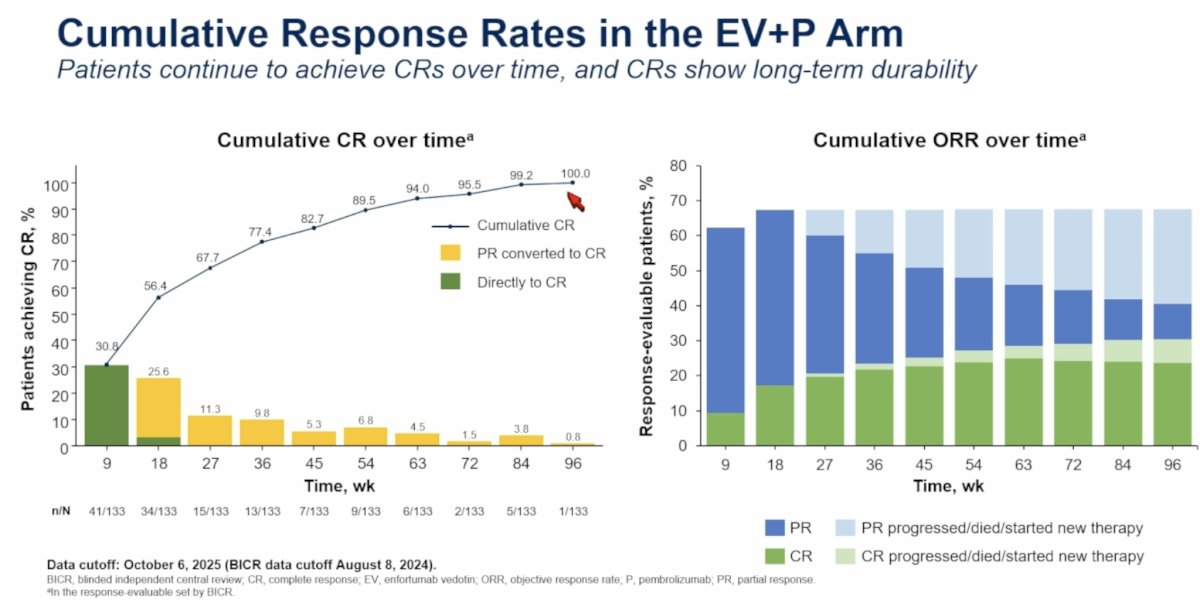
The cumulative response rates in the EV+P arm are summarized below:
Dr. Powles highlighted the excellent survival outcomes among complete responders. Among all patients achieving a CR, the median OS was not reached with EV+P versus 56.7 months with chemotherapy (HR: 0.36, 95% CI: 0.20–0.68).
At 3.5 years, the OS outcomes among CR patients were as follows:
- EV+P: 83.6%
- Chemotherapy: 68%
Importantly, patients whose responses deepened from PR to CR achieved outcomes comparable to the overall CR population. In patients converting from PR to CR, the 3.5 years OS rates were as follows:
- EV+P: 82.4%
- Chemotherapy: 67.1%
Dr. Powles noted that these findings suggest that patients who initially achieve PR should not necessarily be viewed differently from those who achieve immediate CR, as eventual conversion to CR confers similarly excellent long-term outcomes.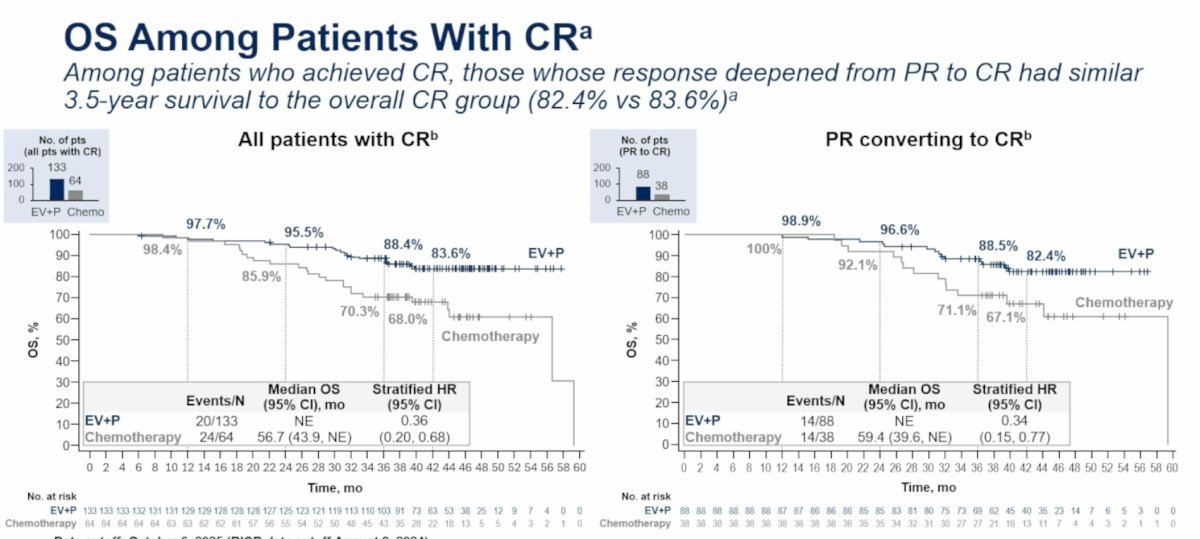
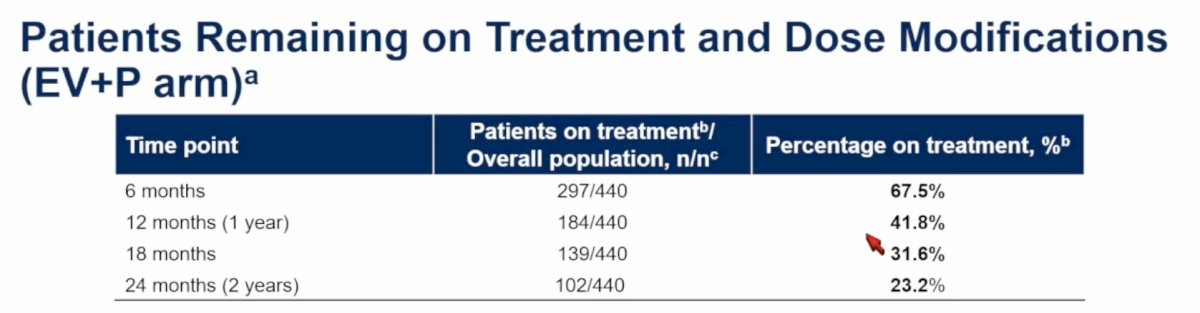
The study investigators next examined long-term treatment exposure. Among EV+P-treated patients:
- 67.5% remained on treatment at 6 months
- 41.8% remained on treatment at 12 months
- 31.6% remained on treatment at 18 months
- 23.2% remained on treatment at 24 months
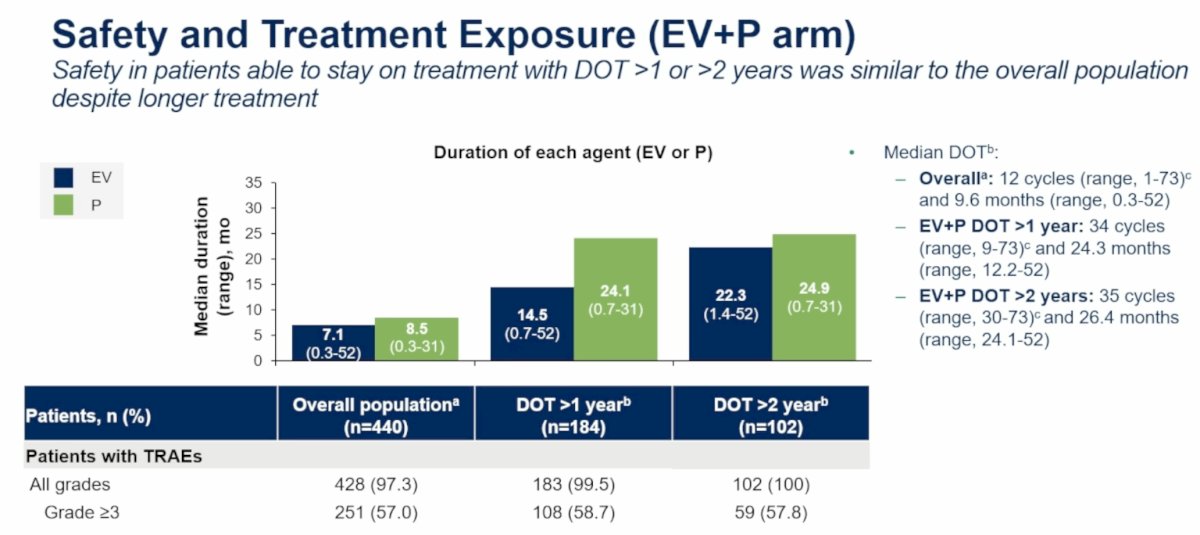
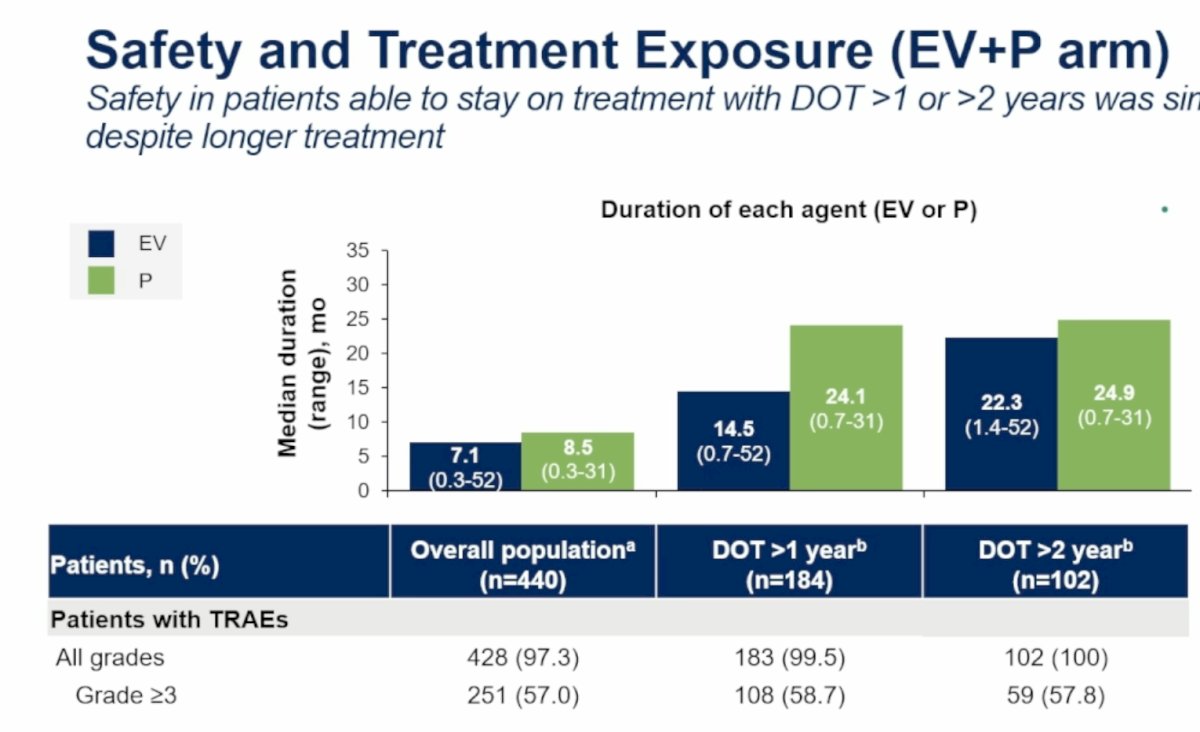
The median duration of treatment in the overall population was:
- EV: 7.1 months
- Pembrolizumab: 8.5 months
Among patients treated for >1 year, the median treatment duration increased substantially:
- EV: 14.5 months
- Pembrolizumab: 24.1 months
For patients treated beyond two years:
- EV: 22.3 months
- Pembrolizumab: 24.9 months
The median treatment duration exceeded two years among patients remaining on therapy long term, reflecting the durability of disease control achieved with EV+P.
Long-term safety remained manageable despite prolonged exposure. Across the overall population, 97.3% experienced any-grade treatment-related adverse events (TRAEs), while 57% experienced grade ≥3 TRAEs. Similar rates were observed among patients remaining on treatment beyond one and two years, suggesting no major cumulative toxicity signal.
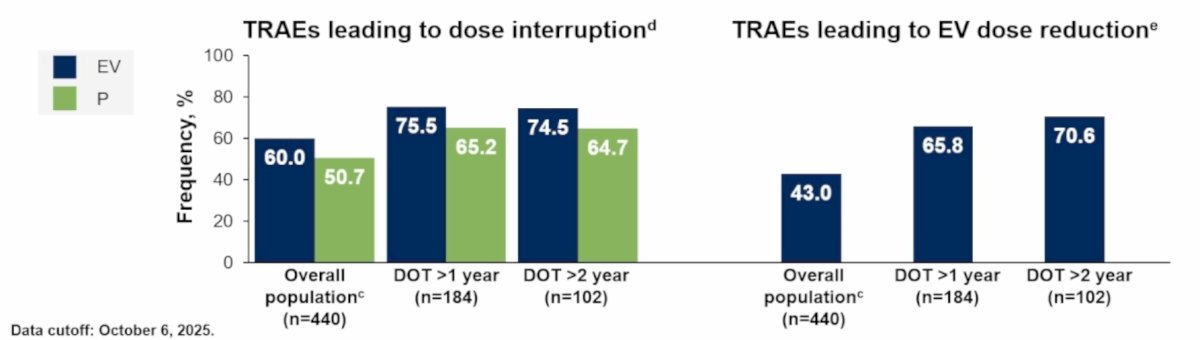
Dose modifications appeared to play an important role in maintaining long-term treatment exposure. In the overall EV+P population:
- 60% experienced EV dose interruptions
- 43% required EV dose reductions
Among patients treated beyond two years:
- 74.5% experienced EV dose interruptions
- 70.6% required EV dose reductions
These findings support the importance of proactive dose management to maintain patients on therapy long term.
No new safety signals emerged with prolonged treatment exposure. Among EV-related adverse events of special interest, modest increases were observed with longer treatment duration, largely driven by low-grade toxicities. Peripheral sensory neuropathy showed the greatest cumulative increase, approaching 90% among patients treated beyond two years, although grade ≥3 neuropathy remained uncommon. Skin reactions, hyperglycemia, dry eye, blurred vision, corneal disorders, and infusion reactions demonstrated similar patterns without evidence of unexpected late toxicity.
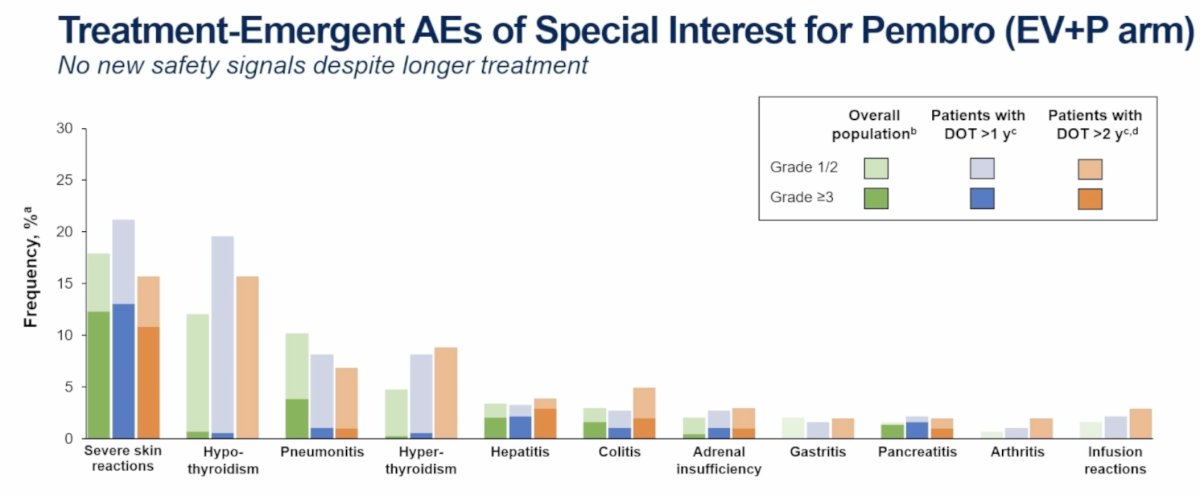
Likewise, pembrolizumab-related adverse events of special interest remained consistent with the known immune-related toxicity profile. The most common events included severe skin reactions, hypothyroidism, pneumonitis, hyperthyroidism, hepatitis, colitis, adrenal insufficiency, gastritis, pancreatitis, arthritis, and infusion reactions. Importantly, no new immune-mediated safety signals emerged despite prolonged exposure.
Dr. Powles concluded his presentation of the EV-302 3.5-year extended follow-up data as follows:
- With ~3.5 years of median follow-up, EV+P continues to demonstrate superior OS benefit, reinforcing EV+P as the preferred SOC for first-line treatment of locally advanced/metastatic urothelial carcinoma
- After EV+P, platinum-based chemotherapy was the most common subsequent treatment. Clinically meaningful response rates to platinum chemotherapy were observed.
- EV+P demonstrated ORRs exceeding those with chemotherapy, with approximately twice as many patients achieving a CR
- Cumulative responses deepened over time, with around two-thirds of patients with CR converting from PR to CR. This group achieved similar survival rates as patients with CR overall
- EV+P continues to demonstrate a consistent and manageable safety profile. Dose interruptions and reductions are important to manage AEs and may allow patients to remain on EV+P therapy
- Enfortumab vedotin plus pembrolizumab is associated with durable and clinically meaningful outcomes in metastatic urothelial carcinoma.
Presented by: Thomas Powles, MBBS, MRCP, MD, Professor of Genitourinary Oncology, Director, Barts Cancer Institute, Cancer Research UK Experimental Cancer Medicine Centre, Queen Mary University of London, London, United Kingdom
Written by: Rashid K. Sayyid, MD, MSc, Assistant Professor, Urologic Oncologist, Department of Urology at The University of Arizona and Banner University Medical Center, Tucson, AZ – @rksayyid on X during the American Society of Clinical Oncology Genitourinary (ASCO) Annual Meeting held in Chicago, IL between May 29th and June 1st, 2026