(UroToday.com) The 2026 American Society of Clinical Oncology (ASCO) Annual Meeting was host to a kidney and bladder cancers oral abstract session, where Dr. Melissa Reimer delivered the discussant presentation titled “Curing Early Bladder Cancer with Multidisciplinary Approaches,” contextualizing the key findings and future directions arising from SAKK 06/19 and the AMBASSADOR health-related quality of life (HRQoL) analysis.
Dr. Reimer framed both studies around a central question: how can multidisciplinary treatment strategies improve cure rates for patients with localized muscle-invasive bladder cancer (MIBC) while simultaneously preserving quality of life and minimizing treatment-related toxicity?
Dr. Reimer emphasized that treatment decisions in localized bladder cancer should be grounded in patient priorities. She highlighted data from an online discrete choice survey of 202 patients with MIBC demonstrating that increasing overall survival at 5 years was the most important treatment attribute, while 71% of respondents preferred bladder preservation. A separate discrete choice study of 60 patients similarly demonstrated strong preferences for treatments that increased life expectancy while reducing adverse effects on body image and lowering the risk of long-term complications (all p<0.001). These findings underscore the central challenge facing the field: maximizing cure rates while preserving bladder function and minimizing treatment burden.
Turning to SAKK 06/19, Dr. Reimer noted that the study represents an innovative attempt to combine local and systemic immunologic approaches through the addition of intravesical recombinant BCG (rBCG) to perioperative gemcitabine/cisplatin plus atezolizumab. As presented by Dr. Cathomas, this approach yielded a centrally reviewed pathological complete response (pCR) rate of 68% (27/40), a pathological response rate (≤ypT1N0) of 83%, and encouraging 12-month event-free and overall survival rates of 90% and 96%, respectively.
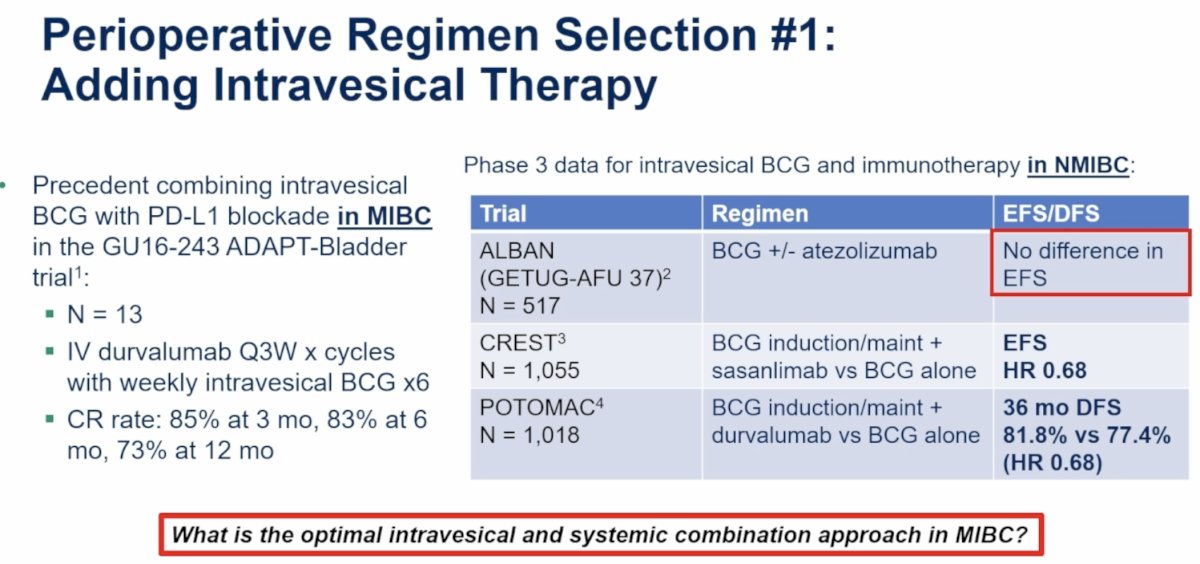
Dr. Reimer first addressed the biological rationale for incorporating intravesical therapy into perioperative treatment. She reviewed prior studies evaluating BCG combined with checkpoint inhibition, highlighting the phase I GU16-243 ADAPT-Bladder study in which 13 patients with MIBC received durvalumab every three weeks for four cycles together with weekly intravesical BCG. Clinical complete response rates were notable at 85% at 3 months, 83% at 6 months, and 73% at 12 months. Although exploratory, these data suggested potential synergy between local and systemic immune activation.
She then reviewed phase III experience evaluating intravesical BCG plus immunotherapy in NMIBC. The ALBAN trial (BCG plus atezolizumab) failed to demonstrate an event-free survival benefit compared to BCG alone.1 In contrast, CREST demonstrated improved recurrence-free survival with BCG induction and maintenance plus sasanlimab versus BCG alone in more than 1,000 patients.2 Similarly, POTOMAC reported a median disease-free survival of 36 months with BCG plus durvalumab compared to 18 months with BCG alone (HR 0.68).3 Collectively, these studies support the biological plausibility of combining intravesical and systemic immunotherapy, while simultaneously illustrating that the optimal combination strategy remains uncertain. Dr. Reimer summarized this section by posing the question: “What is the optimal intravesical and systemic combination approach in MIBC?”
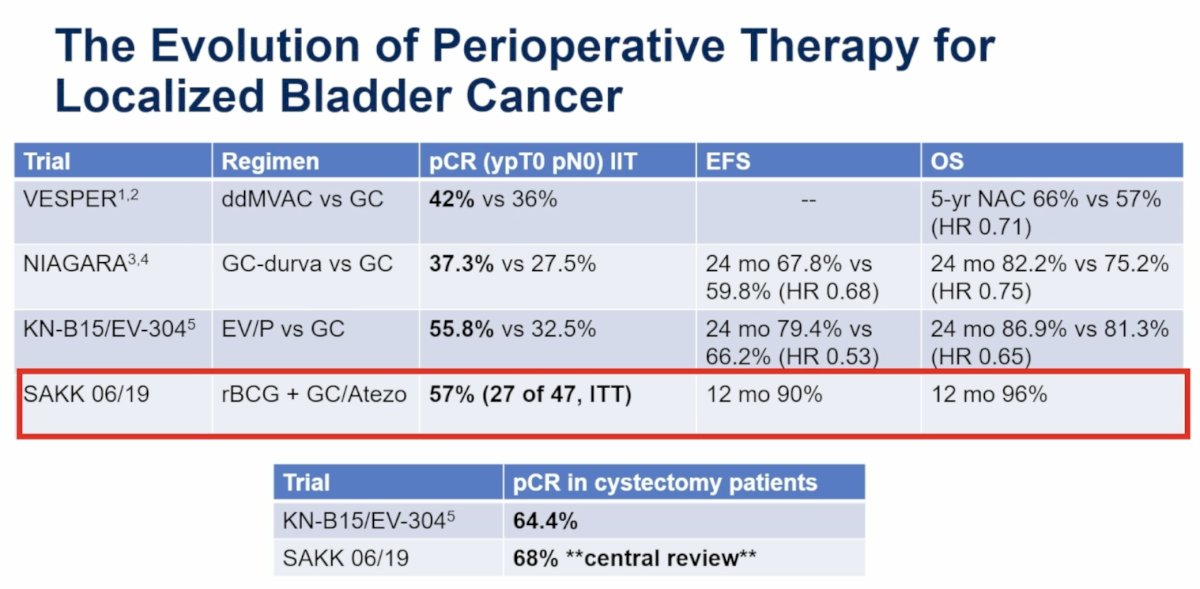
To place SAKK 06/19 into context, Dr. Reimer reviewed the evolution of perioperative therapy for localized bladder cancer. She compared outcomes across several landmark studies that have progressively improved pathological response and survival outcomes.
- In VESPER, dose-dense MVAC achieved a pCR rate of 42% compared to 36% with gemcitabine-cisplatin, translating into a 5-year overall survival of 66% versus 57% (HR 0.71).4
- NIAGARA subsequently demonstrated a pCR rate of 37.3% with durvalumab plus gemcitabine-cisplatin compared to 27.5% with chemotherapy alone, with corresponding improvements in 24-month event-free survival (67.8% versus 59.8%; HR 0.68) and overall survival (82.2% versus 75.2%; HR 0.75).5
- More recently, KEYNOTE-B15/EV-304 reported a pCR rate of 55.8% with enfortumab vedotin plus pembrolizumab versus 32.5% with chemotherapy, accompanied by improvements in 24-month EFS (74.5% versus 66.2%; HR 0.53) and OS (85.4% versus 81.3%; HR 0.65).6
- Against this backdrop, SAKK 06/19 achieved a pCR rate of 57% in the intention-to-treat population and 68% among cystectomy patients undergoing central pathology review, with 12-month EFS and OS rates of 90% and 96%, respectively.
- Dr. Reimer noted that these results place SAKK 06/19 among the most active perioperative regimens reported to date and raise important questions regarding the specific contribution of intravesical rBCG to these outcomes.
A major focus of Dr. Reimer’s discussion centered on the clinical implications of achieving higher pCR rates. She reviewed updated NIAGARA analyses demonstrating that patients achieving pCR experienced substantially superior event-free and overall survival compared with patients harboring residual disease. These observations reinforce the concept that pCR is not merely a surrogate endpoint but may identify patients with exceptionally favorable long-term outcomes. Consequently, increasing pCR rates may create opportunities for bladder-preservation strategies in selected patients.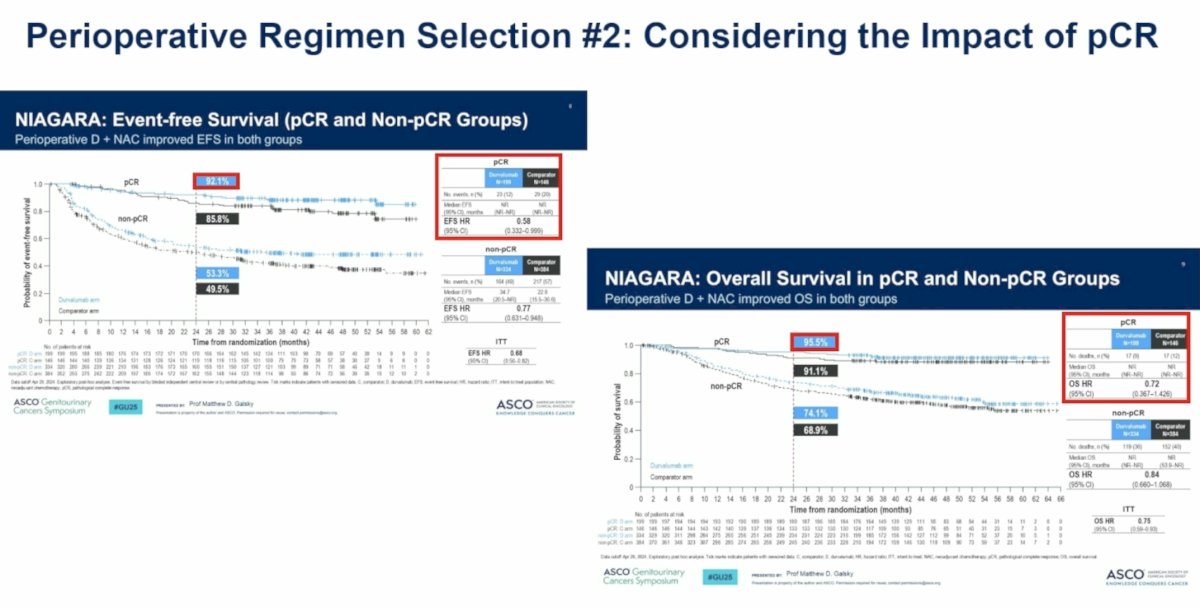
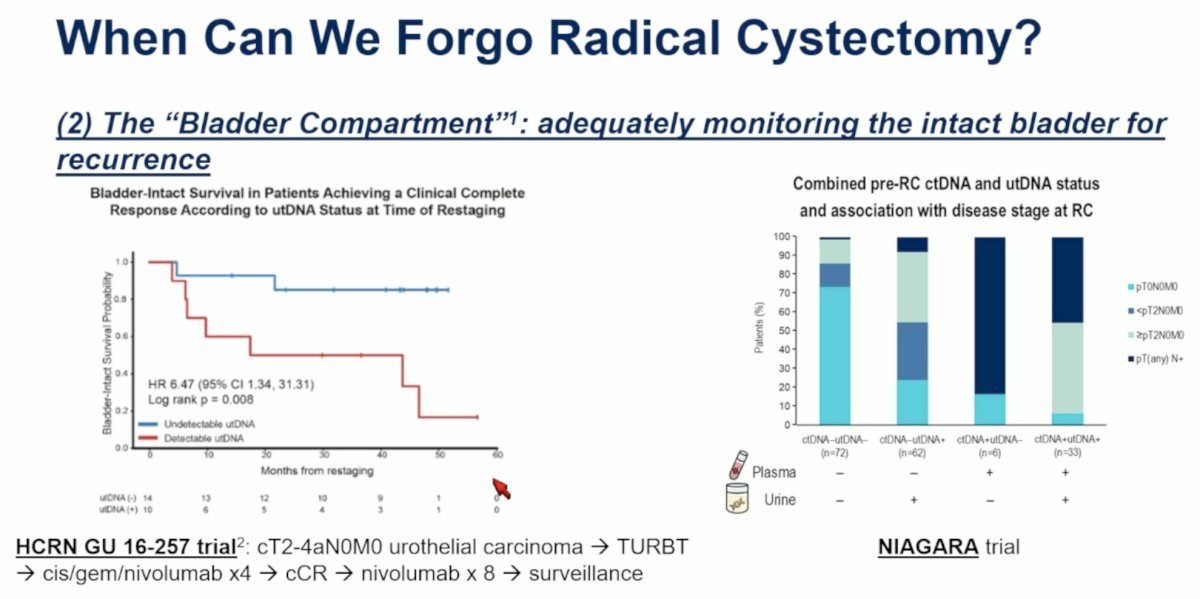
This naturally led to one of the central questions of her presentation: “When can we forgo radical cystectomy?”
Dr. Reimer emphasized that the first prerequisite is the establishment of a robust and reproducible definition of clinical complete response (cCR). In SAKK 06/19, among 25 evaluable patients, cCR demonstrated an impressive positive predictive value of 92% for predicting pCR using a multimodal assessment consisting of CT chest/abdomen/pelvis imaging, dedicated bladder MRI, cystoscopy, and urine cytology. She highlighted recently proposed International Bladder Cancer Group and Global Society of Rare Genitourinary Tumors consensus recommendations, which define cCR using negative cross-sectional imaging with an MRI bladder protocol, negative urine cytology, and negative post-chemotherapy bladder biopsies with systematic bladder mapping. Recommendations regarding the incorporation of circulating tumor DNA (ctDNA) and urinary tumor DNA (utDNA) remain under development.
However, Dr. Reimer cautioned that accurately assessing systemic disease clearance does not necessarily address the challenge of monitoring the intact bladder. She referred to this as the “bladder compartment” problem. She highlighted findings from RETAIN-2, in which patients received neoadjuvant dose-dense MVAC plus nivolumab followed by active surveillance. Among 40 monitored patients, 37 remained ctDNA-negative; nevertheless, 21 patients (52.5%) experienced local recurrence, and only 2 of these 21 recurrent cases (9.5%) were ctDNA-positive.6 These findings suggest that ctDNA monitoring alone appears insufficient to assess local bladder recurrence and underscore the continued importance of intensive local surveillance strategies.
Dr. Reimer further illustrated this challenge using emerging bladder-preservation data from HCRN GU14-257 and exploratory analyses from NIAGARA evaluating the relationship between combined pCR and ctDNA status. Together, these studies suggest that systemic molecular remission and local bladder control may represent distinct biological phenomena requiring separate monitoring strategies.
Importantly, Dr. Reimer proposed that intravesical rBCG may ultimately have a role beyond improving pCR rates. She questioned whether additional local therapy delivered directly to the intact bladder could decrease the risk of local relapse and thereby facilitate bladder-preservation approaches. While speculative, this concept represents a potentially important future direction for investigation and may ultimately define the clinical niche for intravesical rBCG in MIBC.
Another important issue raised during the discussion concerned treatment de-escalation following favorable pathological responses. Dr. Reimer highlighted that 31 patients in SAKK 06/19 achieved ≤ypT1N0 disease and therefore did not receive adjuvant atezolizumab according to protocol. She questioned whether these patients derive meaningful benefit from additional immunotherapy and suggested that future analyses examining event-free survival, overall survival, and ctDNA status could help identify patients who can safely avoid adjuvant treatment. Such an approach could substantially reduce treatment burden and healthcare expenditures. She noted that one year of adjuvant atezolizumab, administered every three weeks, costs approximately $88,088, emphasizing the potential financial implications of improved patient selection.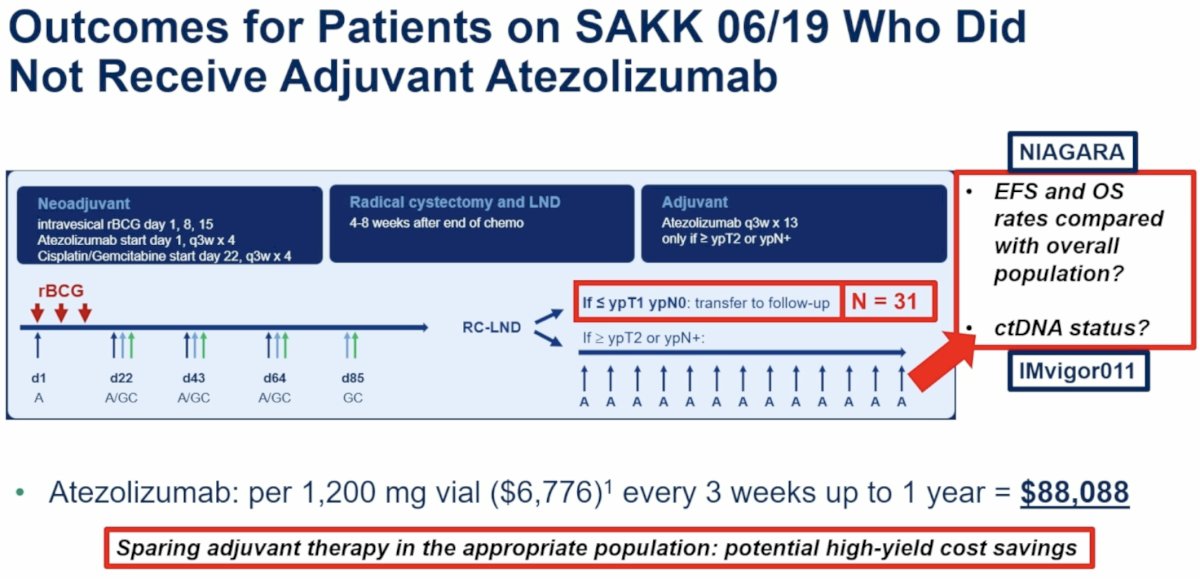
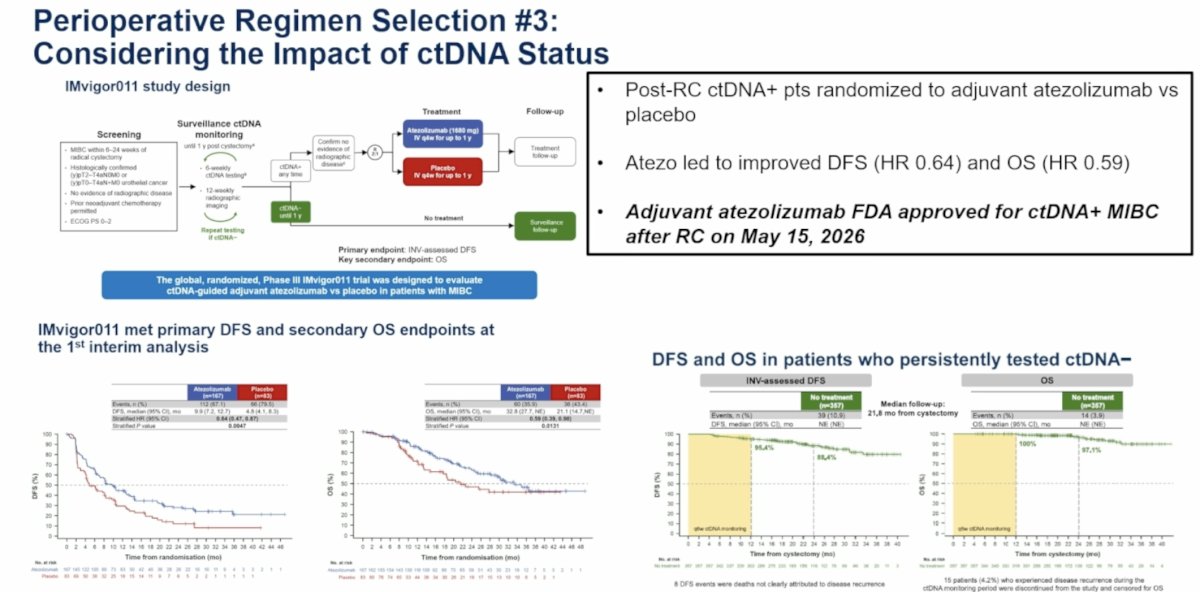
The discussion then expanded to the emerging role of ctDNA-guided treatment selection. Dr. Reimer reviewed IMvigor011, in which post-cystectomy ctDNA-positive patients were randomized to adjuvant atezolizumab or placebo.7 Atezolizumab significantly improved disease-free survival (HR 0.64) and overall survival (HR 0.59), leading to FDA approval of adjuvant atezolizumab for ctDNA-positive MIBC following radical cystectomy on May 15, 2026. She suggested that future treatment paradigms will increasingly integrate clinical response assessment, ctDNA, utDNA, urine cytology, and imaging biomarkers to individualize decisions regarding radical cystectomy, adjuvant therapy, and bladder preservation.
To illustrate this concept, Dr. Reimer presented a proposed future MIBC treatment algorithm. Patients would receive intensified neoadjuvant therapy, such as enfortumab vedotin plus pembrolizumab with or without intravesical rBCG, followed by a comprehensive assessment incorporating bladder MRI, repeat TURBT, urine cytology, ctDNA, and utDNA. Patients achieving cCR with negative molecular biomarkers could potentially enter bladder-preservation pathways with intensive surveillance, whereas those with persistent disease or positive biomarkers would proceed to radical cystectomy followed by risk-adapted systemic therapy. This framework reflects the growing movement toward biologically individualized treatment strategies rather than uniform management for all patients.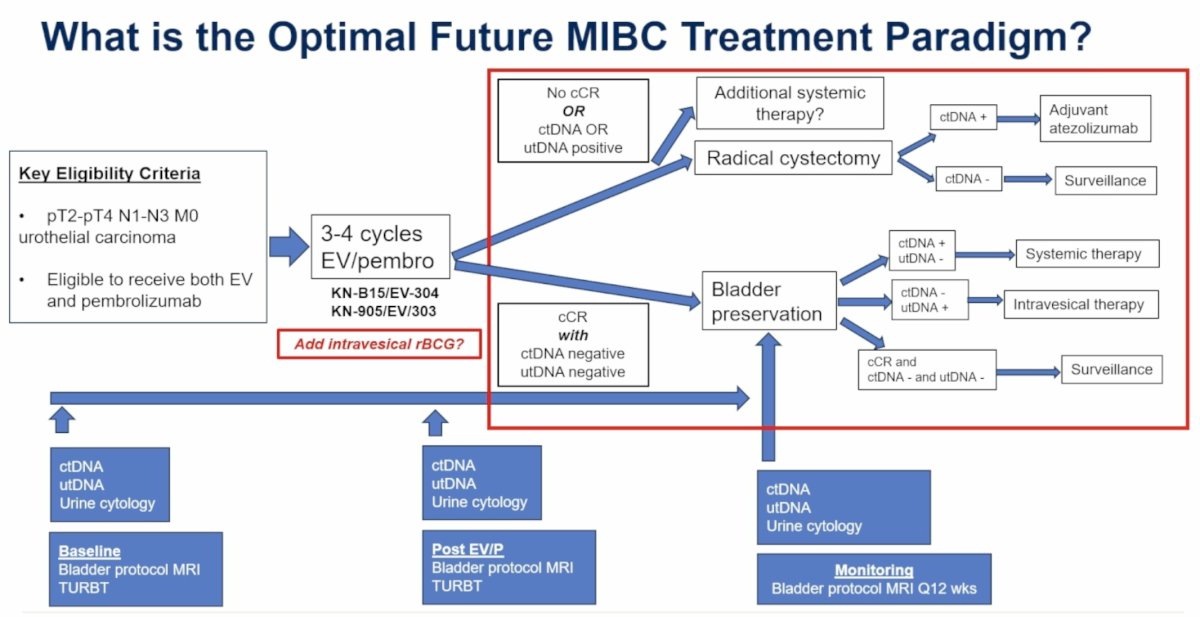
Discussion of Abstract #4513: AMBASSADOR HRQoL Analysis
Dr. Reimer then turned her attention to the AMBASSADOR HRQoL analysis presented by Dr. Ronald Chen. She emphasized that HRQoL outcomes remain a critical component of modern clinical trial infrastructure and should be considered alongside traditional efficacy endpoints when evaluating adjuvant therapies.
As previously reported, AMBASSADOR demonstrated a significant disease-free survival benefit with adjuvant pembrolizumab, improving median DFS from 14.2 months to 29.6 months (HR 0.73).8 The HRQoL analysis subsequently showed that pembrolizumab was associated with increased fatigue and dyspnea, with modest downstream effects on physical and role functioning. However, despite these treatment-related toxicities, there was no meaningful deterioration in global health status or overall HRQoL.
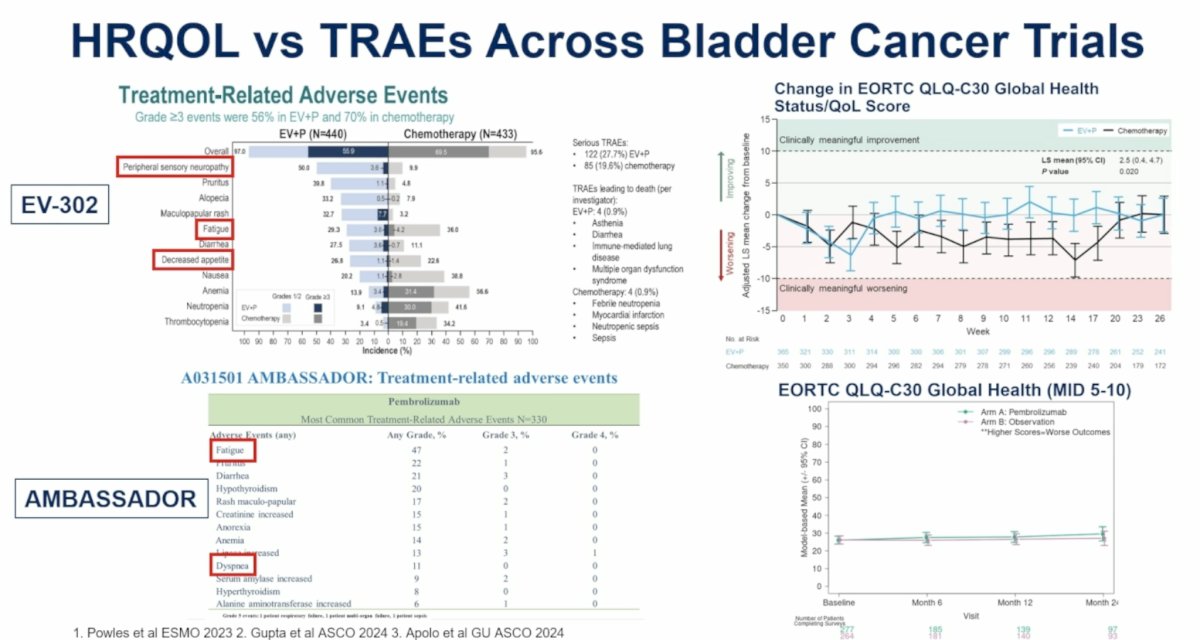
Dr. Reimer highlighted what she viewed as one of the most important observations from the AMBASSADOR analysis. Comparing AMBASSADOR with other contemporary studies, such as EV-302, she demonstrated that substantial treatment-related adverse events can occur without corresponding declines in global HRQoL metrics. The figure above contrasts the frequency and severity of treatment-related adverse events with relatively stable EORTC QLQ-C30 global health scores, illustrating a potential disconnect between toxicity burden and traditional HRQoL assessments. These observations suggest that conventional HRQoL instruments may not fully capture the day-to-day impact of treatment-related toxicities experienced by patients receiving modern systemic therapies.
Accordingly, Dr. Reimer argued that future studies should focus not only on measuring HRQoL but also on improving how treatment-related toxicities are captured from the patient perspective. She emphasized that HRQoL and patient-reported outcomes remain critical components of clinical trial design but may not adequately characterize the true burden of treatment-emergent adverse events. This led to the question: “How can we further optimize PRO and HRQoL tools to adequately capture TRAE impacts?”
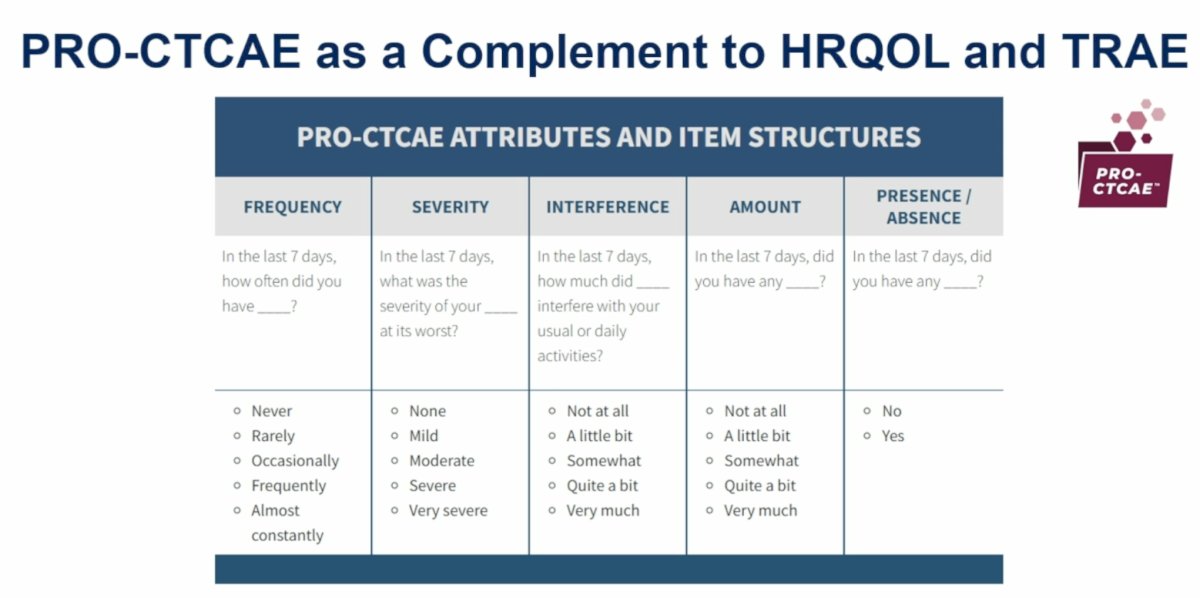
To address this challenge, Dr. Reimer highlighted the Patient-Reported Outcomes version of the Common Terminology Criteria for Adverse Events (PRO-CTCAE) as a complementary assessment tool. Unlike traditional HRQoL instruments, PRO-CTCAE captures multiple symptom dimensions, including frequency, severity, interference with daily activities, amount, and symptom presence or absence. By providing a more granular evaluation of symptomatic toxicity, PRO-CTCAE may offer a more comprehensive understanding of treatment burden and better reflect the patient experience.
Finally, Dr. Reimer broadened the discussion to the increasingly complex process of adjuvant therapy selection in MIBC. She highlighted several factors that should inform treatment decisions moving forward, including pathological response status, ctDNA status, patient-reported outcomes, treatment-related toxicities, HRQoL measures, financial toxicity, and drug accessibility. She specifically noted the substantial costs associated with contemporary therapies, including estimated annual pembrolizumab costs ranging from $144,736 to $288,753 and enfortumab vedotin costs approaching $227,529 for nine treatment cycles. She also emphasized disparities in drug access across low- and middle-income countries, reinforcing the importance of considering resource utilization alongside efficacy when developing future treatment paradigms.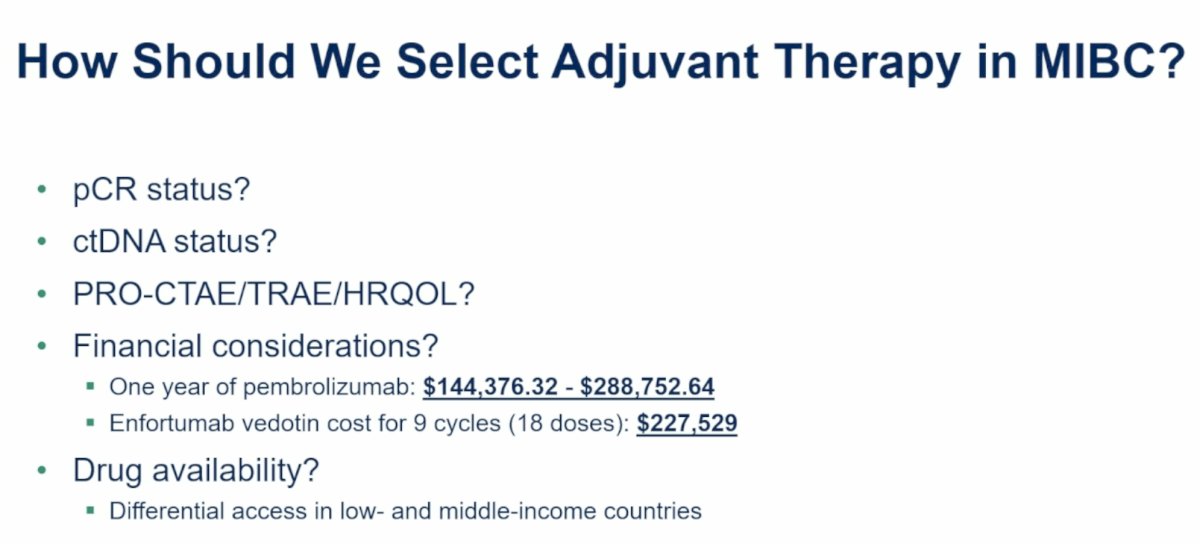
In her concluding remarks, Dr. Reimer summarized several overarching themes.
- First, combination systemic and intravesical approaches represent a promising multidisciplinary strategy for improving outcomes in MIBC, although the precise role of intravesical therapy remains unconfirmed and requires further study.
- Second, determining whether some patients can safely avoid radical cystectomy following exceptional responses has become a high-priority research question. Third, ctDNA-guided treatment strategies are poised to play an increasingly important role in perioperative management.
- Third, maximizing HRQoL while minimizing both treatment-emergent and financial toxicities should remain a central focus of future clinical investigation.
The key takeaway points from Dr. Reimer’s discussant presentation were as follows:
- Combination systemic and intravesical therapies represent a promising multidisciplinary strategy for MIBC, but the independent contribution of intravesical rBCG remains uncertain.
- SAKK 06/19 achieved a centrally reviewed pCR rate of 68%, comparing favorably with outcomes reported in VESPER, NIAGARA, and KEYNOTE-B15/EV-304.
- Higher pCR rates may create opportunities for bladder-preservation approaches, although standardized cCR definitions and improved surveillance strategies are needed before radical cystectomy can be safely omitted.
- ctDNA monitoring alone appears insufficient for detecting local bladder recurrence, highlighting the continued importance of imaging, cystoscopy, and tissue-based assessment.
- ctDNA and urinary biomarkers are likely to become central components of future perioperative treatment selection and bladder-preservation algorithms.
- AMBASSADOR demonstrated that adjuvant pembrolizumab improves disease-free survival while producing only modest effects on selected symptom and functional domains without compromising overall HRQoL.
- Traditional HRQoL instruments may incompletely capture treatment burden, supporting the incorporation of complementary measures such as PRO-CTCAE.
- Future treatment paradigms must balance efficacy, toxicity, quality of life, cost, biomarker status, and patient preferences to optimize individualized care for patients with localized bladder cancer.
Presented by Melissa A. Reimers, MD, Associate Professor, Department of Medicine, Division of Medical Oncology, St. Louis, MO, USA
Written by: Rashid K. Sayyid, MD, MSc, Assistant Professor, Urologic Oncologist, Department of Urology at The University of Arizona and Banner University Medical Center, Tucson, AZ – @rksayyid on X during the American Society of Clinical Oncology Genitourinary (ASCO) Annual Meeting held in Chicago, IL between May 29th and June 1st, 2026
References:- Roupret M, Bensalah K, Pfister C, et al. ALBAN (GETUG-AFU 37): a phase III, randomized, open-label international trial of intravenous atezolizumab and intravesical Bacillus Calmette-Guérin (BCG) versus BCG alone in BCG-naive high-risk, non-muscle-invasive bladder cancer (NMIBC). Ann Oncol. 2026;37(1):12-23.
- Shore ND, Powles TB, Bedke J, et al. Sasanlimab plus BCG in BCG-naive, high-risk non-muscle invasive bladder cancer: the randomized phase 3 CREST trial. Nat Med. 2025;31(8):2815.
- De Santis M, Palou Redorta J, Nishiyama N, et al. Durvalumab in combination with BCG for BCG-naive, high-risk, non-muscle-invasive bladder cancer (POTOMAC): final analysis of a randomised, open-label, phase 3 trial. Lancet. 2025;406(10516):2221-2234.
- Pfister C, Gravis G, Fléchon A, et al. Perioperative Dose-Dense Methotrexate, Vinblastine, Doxorubicin, and Cisplatin in Muscle-Invasive Bladder Cancer (VESPER): Survival Endpoints at 5 Years in an Open-Label, Randomised, Phase 3 Study. Lancet Oncol. 2025;26(4):494-506.
- Powles T, Catto JWF, Galsky MD, et al. Perioperative Durvalumab With Neoadjuvant Chemotherapy in Operable Bladder Cancer. N Engl J Med. 2024;391:1773-1786.
- Ghatalia P, Ross EA, Zibelman MR, et al. A Phase 2 Trial of Risk-Enabled Therapy After Neoadjuvant Chemo-Immunotherapy for Muscle-Invasive Bladder Cancer (RETAIN-2). J Clin Oncol. 2025;43(5 Suppl):815.3
- Powles T, Kann AG, Castellano D, et al. ctDNA-Guided Adjuvant Atezolizumab in Muscle-Invasive Bladder Cancer. N Engl J Med. 2025;393:2395-2408.
- Apolo AB, Ballman KV, Sonpavde G, et al. Adjuvant Pembrolizumab versus Observation in Muscle-Invasive Urothelial Carcinoma. N Engl J Med. 2024;391:1217-1228. doi:10.1056/NEJMoa2401726.