(UroToday.com) The 2026 American Society of Clinical Oncology (ASCO) Annual Meeting was host to a kidney and bladder cancer oral abstract session. Dr. Ronald Chen presented health-related quality of life (HRQOL) data from the AMBASSADOR (Alliance A031501) trial of pembrolizumab versus observation for high-risk muscle-invasive urothelial carcinoma (MIUC) after surgery.
Muscle-invasive urothelial carcinoma remains an aggressive disease. Patients with “high-risk” disease harbor a 60–70% chance of recurrence following radical surgery, with “high-risk” status defined as follows:
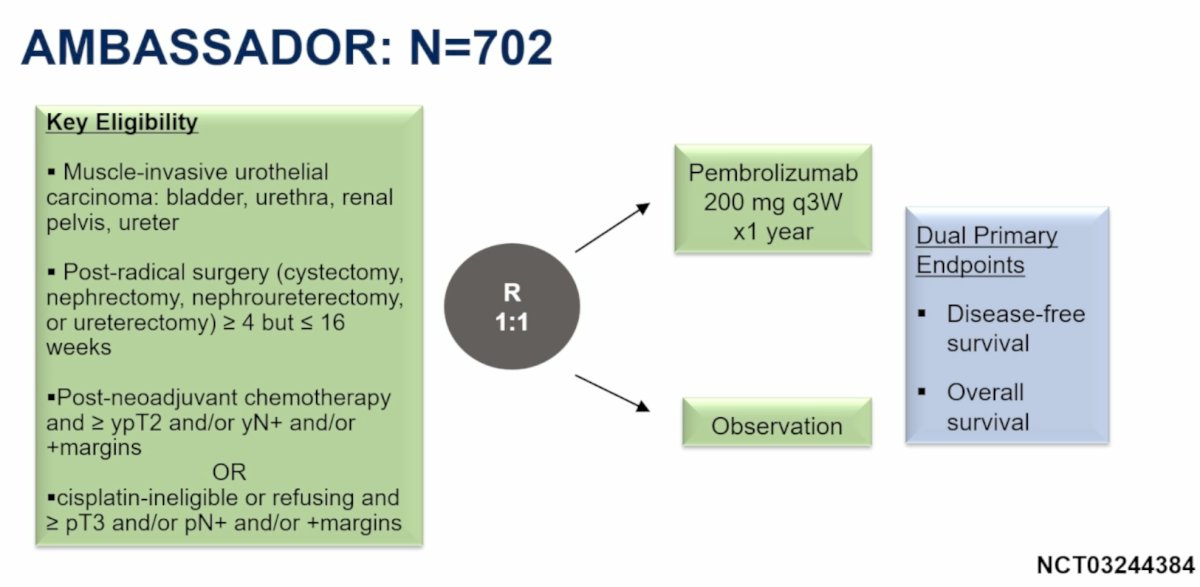
- In patients without prior neoadjuvant cisplatin-based chemotherapy: pT3+, pN+, or positive margins
- Prior neoadjuvant cisplatin-based chemotherapy: ypT2+, or ypN+, or positive margins
Given this substantial risk of recurrence, there remains an unmet need for adjuvant therapy to improve patient outcomes. Pembrolizumab, a programmed death-1 (PD-1) checkpoint inhibitor, has previously demonstrated efficacy in urothelial carcinoma.
The AMBASSADOR trial enrolled 702 patients with muscle-invasive urothelial carcinoma of the bladder, urethra, renal pelvis, or ureter. Eligible patients had undergone radical surgery (cystectomy, nephrectomy, nephroureterectomy, or ureterectomy) within 4–16 weeks prior to enrollment. Patients were randomized 1:1 to receive pembrolizumab 200 mg every 3 weeks for one year or observation. The dual primary endpoints were disease-free survival (DFS) and overall survival.
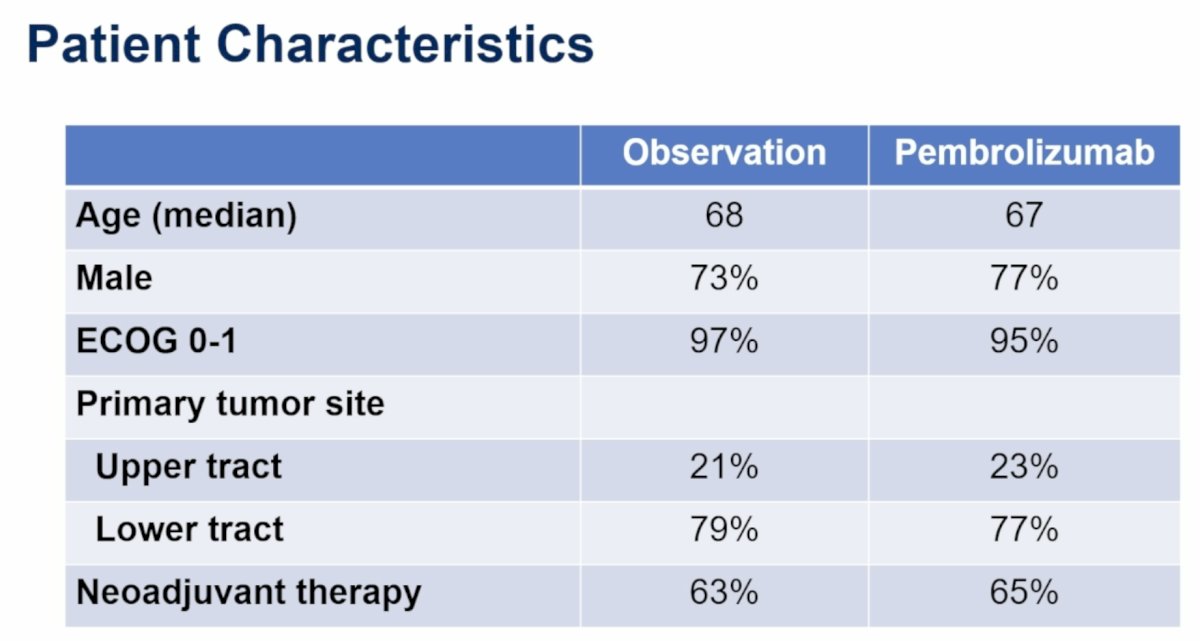
Baseline characteristics were well-balanced between treatment arms. The median age was 68 years in the observation arm and 67 years in the pembrolizumab arm. Male patients comprised 73% and 77% of the cohorts, respectively, while ECOG performance status 0–1 was present in 97% and 95%, respectively. Upper tract primary tumors accounted for 21% and 23% of patients, with lower tract tumors accounting for 79% and 77%, respectively. Prior neoadjuvant therapy had been administered in 63% of patients assigned to observation and 65% of those receiving pembrolizumab.
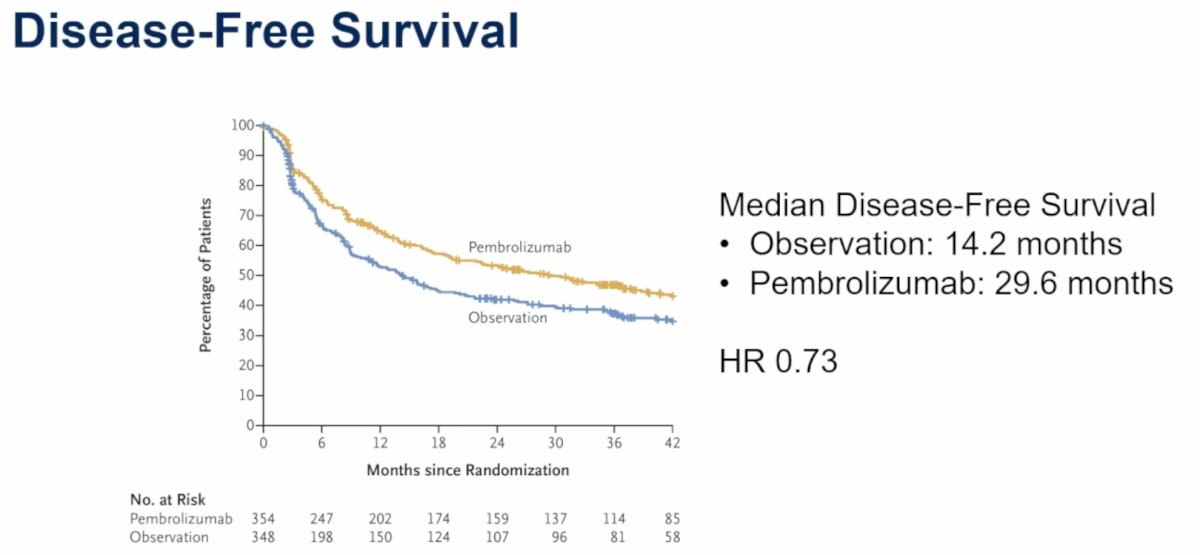
As previously reported,1 adjuvant pembrolizumab significantly improved DFS. Median DFS increased from 14.2 months with observation to 29.6 months with pembrolizumab (HR 0.73).
Since adjuvant therapy improves disease control, Dr. Chen noted that patients and physicians also need to understand the impact of intensified treatment on HRQOL. HRQOL assessments included:
- EORTC QLQ-C30 and BLM30 questionnaires
- Symptom domains including fatigue, dyspnea, and nausea/vomiting
- Functional domains, including physical functioning and role functioning
- Global health and overall HRQOL assessments
- Bladder cancer-specific domains, including urinary symptoms and sexual function
- EQ5D-5L overall HRQOL/health status assessments, which will be used for quality-adjusted survival analyses
The primary HRQOL analyses focused on changes from baseline at 6, 12, and 24 months, interpreted according to established minimally important difference (MID), with higher scores indicating worse outcomes.
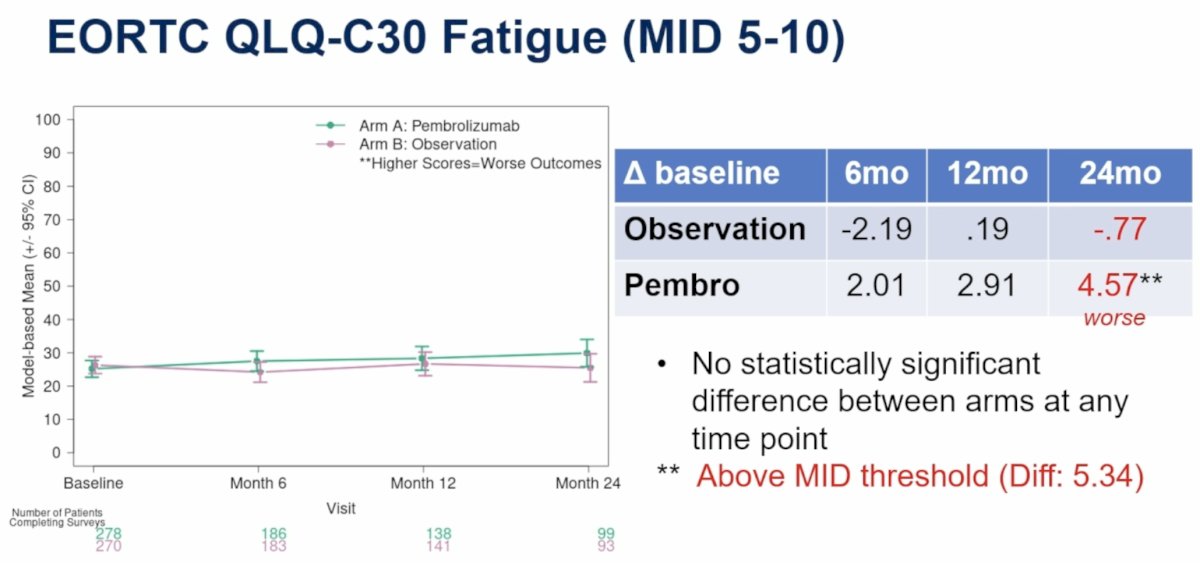
Fatigue (MID 5–10)For fatigue, no statistically significant difference between treatment arms was observed at any time point. At 24 months, fatigue scores increased by 4.57 points from baseline in the pembrolizumab arm compared with a decrease of 0.77 points in the observation arm, producing an inter-arm difference of 5.34 points that exceeded the MID threshold.
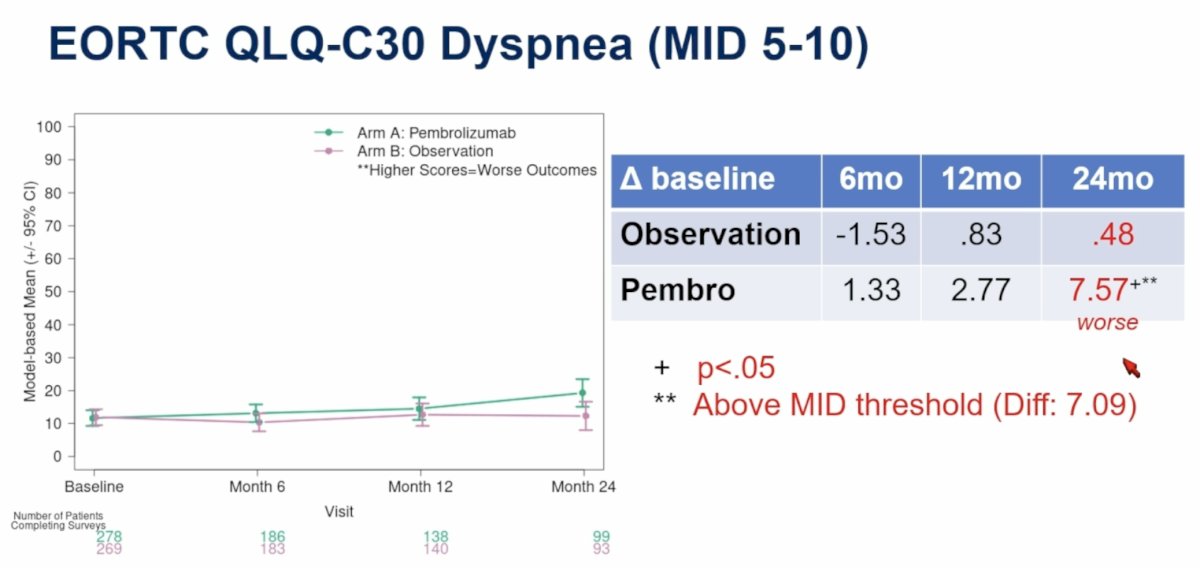
For dyspnea, patients receiving pembrolizumab experienced greater worsening over time. At 24 months:
- Observation: 0.48-point increase from baseline
- Pembrolizumab: 7.57-point increase from baseline
- This represented a statistically significant difference (p<0.05) and exceeded the MID threshold, with an inter-arm difference of 7.09 points. Earlier time points demonstrated smaller differences.
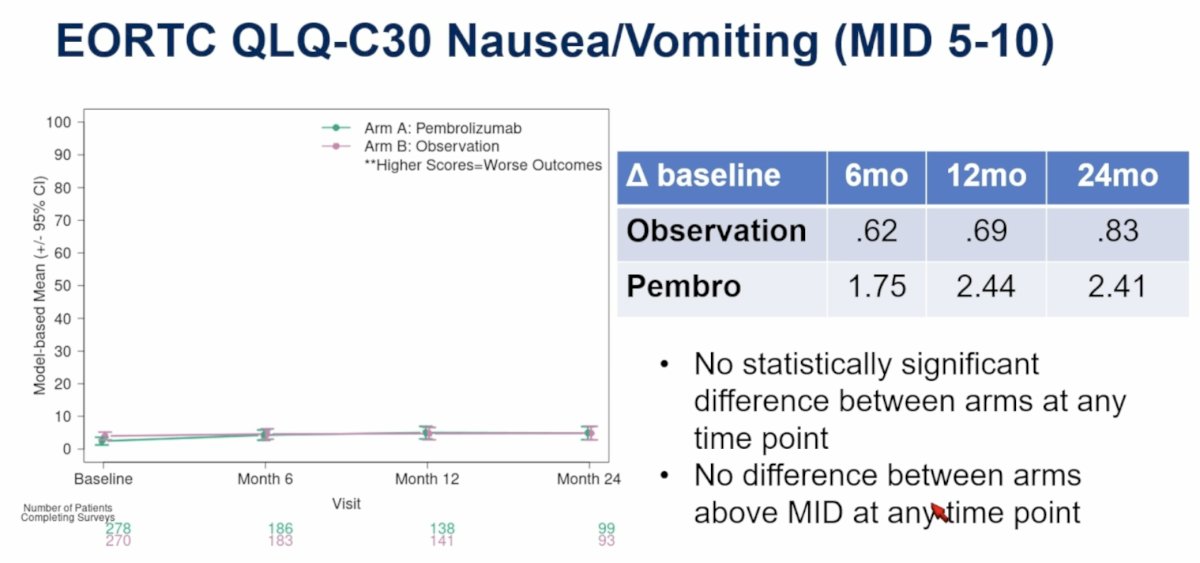
For nausea/vomiting, no statistically significant difference between arms was observed at any time point, and no difference exceeded the MID threshold.
Physical functioning assessed activities of daily living, walking, and strenuous activities. In this domain, higher scores indicate better outcomes.
At 24 months:
- Observation: -0.81 change from baseline
- Pembrolizumab: -5.97 change from baseline
- Although there was no statistically significant difference between treatment arms, the 5.16-point inter-arm difference exceeded the MID threshold.

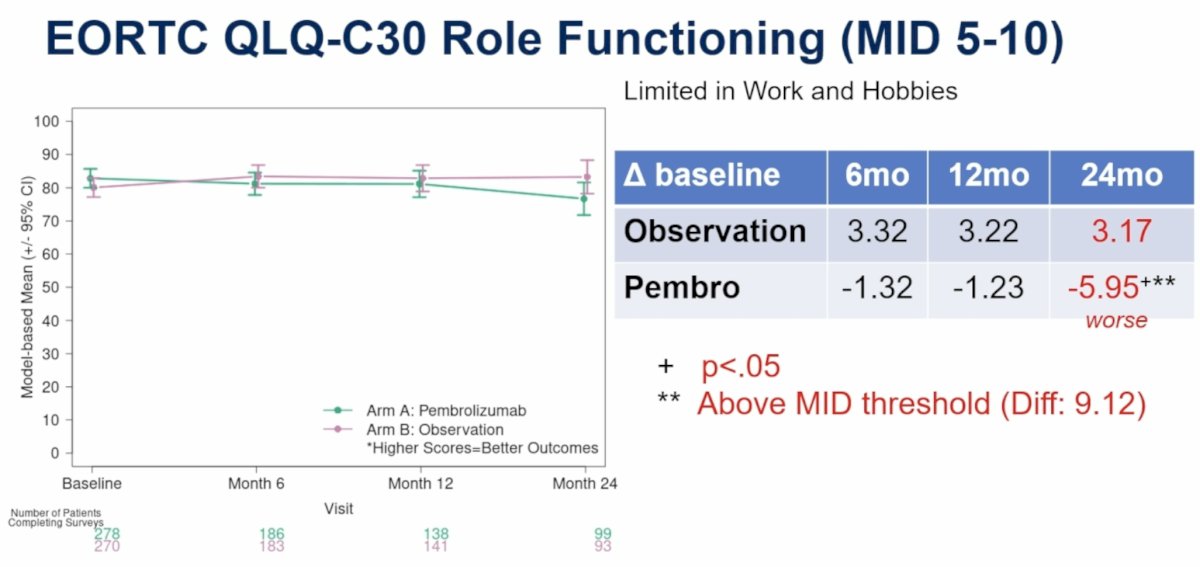
Role functioning evaluated limitations in work and hobbies. Higher scores indicate better outcomes here.
At 24 months:
- Observation: 3.17-point improvement from baseline
- Pembrolizumab: -5.95-point decline from baseline
- This represented a statistically significant difference (p<0.05) and exceeded the MID threshold, with a clinically meaningful inter-arm difference of 9.12 points.
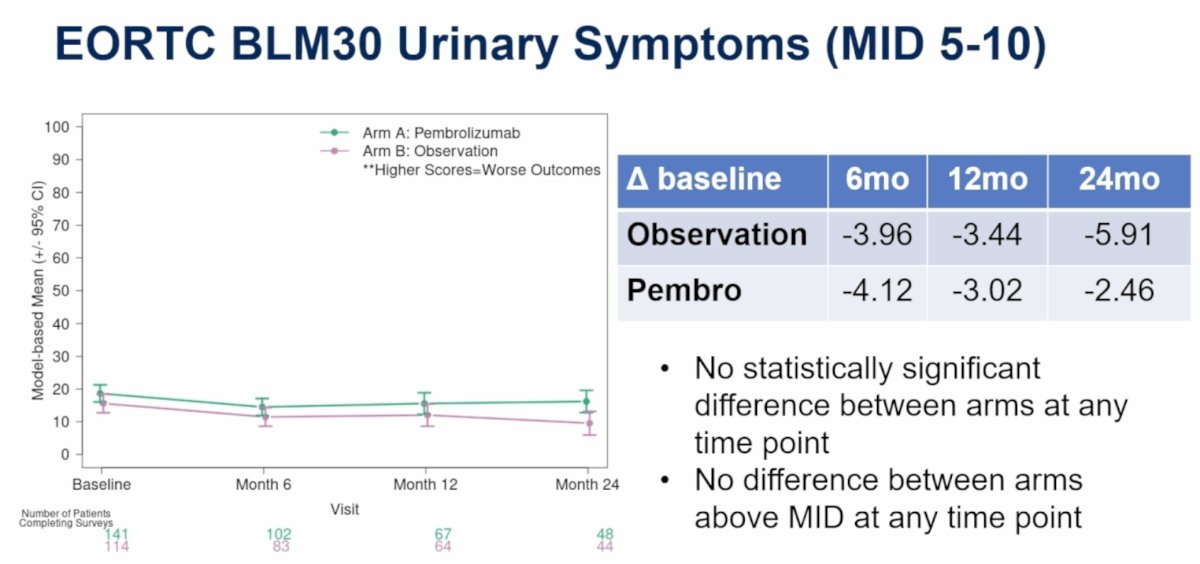
For EORTC BLM30 urinary symptoms (higher scores indicate worse outcomes), no statistically significant differences between treatment arms were observed at any time point, and no differences exceeded MID thresholds.
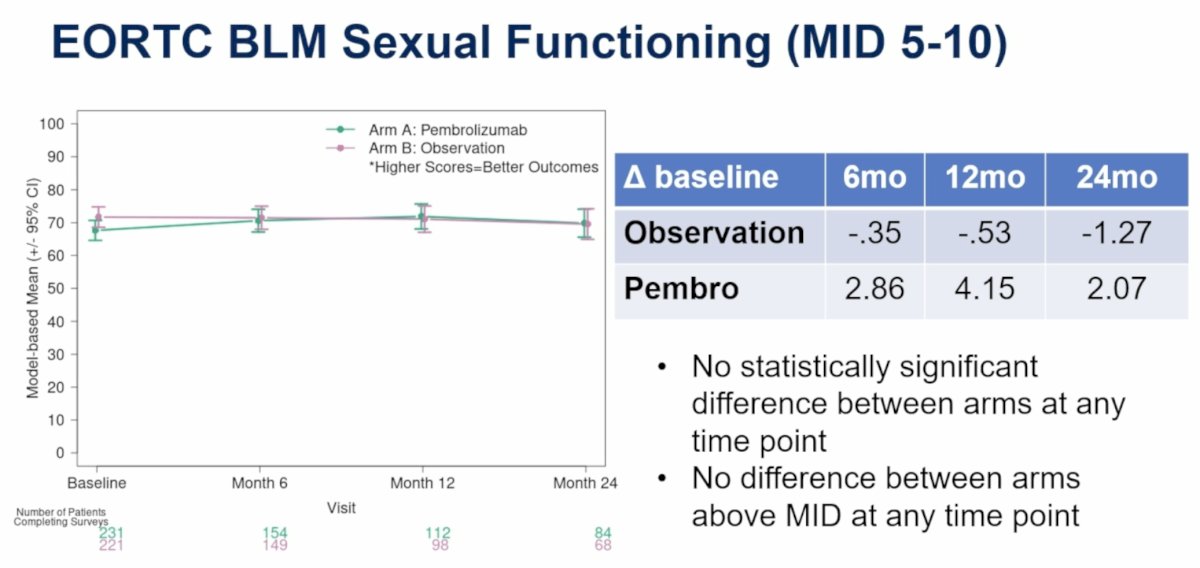
For sexual functioning (higher scores indicate better outcomes), no statistically significant differences between treatment arms were observed, and no differences exceeded MID thresholds.
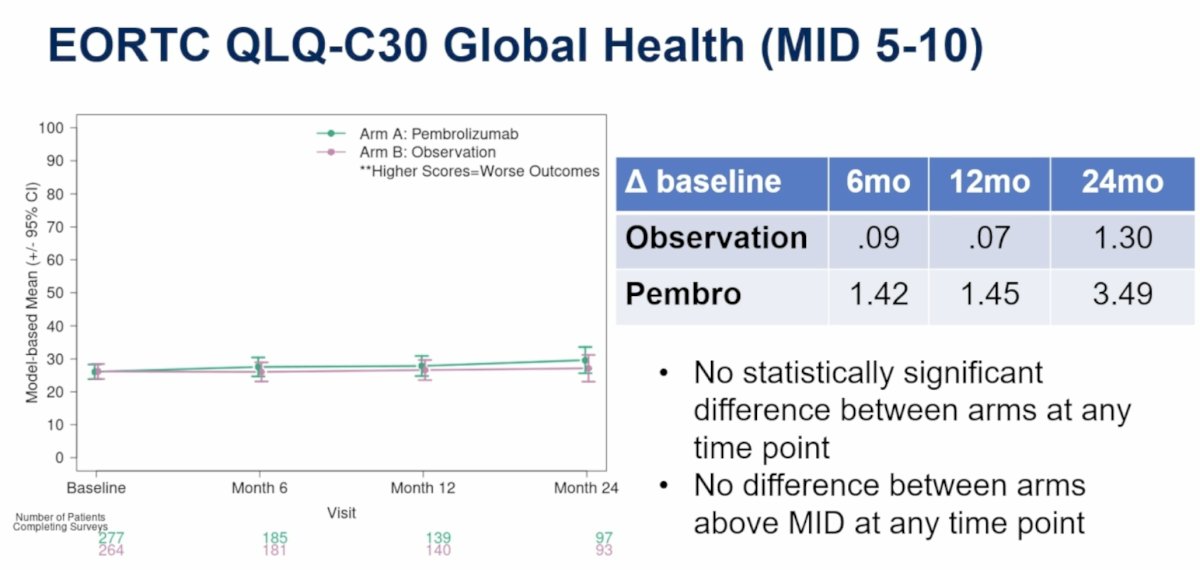
For EORTC QLQ-C30 Global Health, there were no statistically significant differences between treatment arms at any time point, and no differences exceeded MID thresholds.
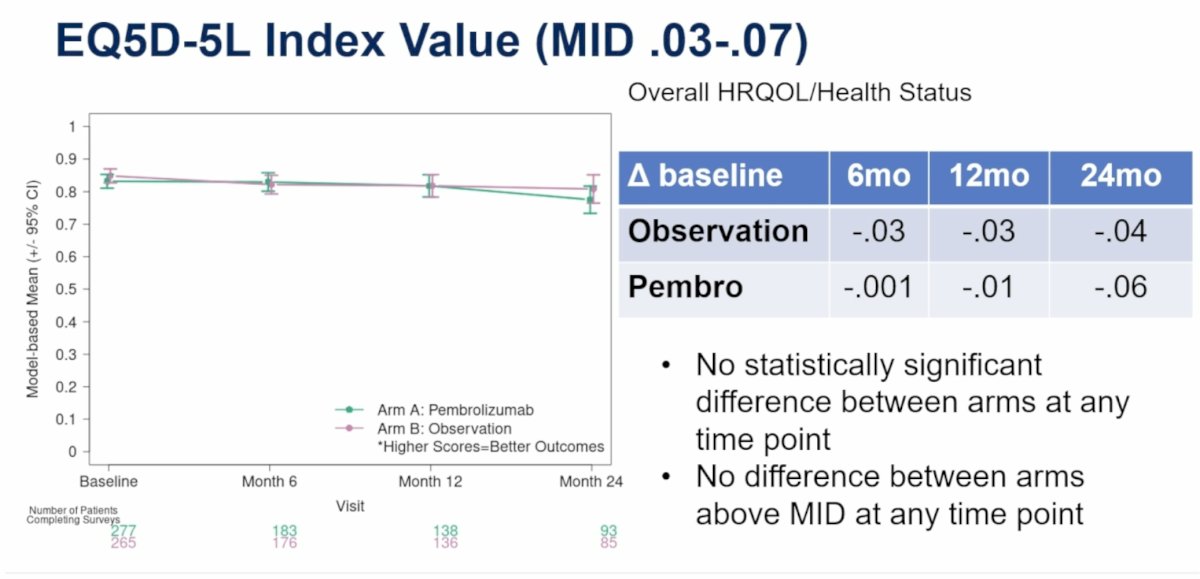
Similarly, EQ5D-5L Index Value (MID 0.03–0.07), which assesses overall HRQOL/health status, showed no statistically significant differences between arms and no differences above MID thresholds.
Dr. Chen summarized the key findings as follows:
- Adjuvant pembrolizumab versus observation after radical surgery for patients with high-risk muscle-invasive urothelial carcinoma was associated with increased fatigue and dyspnea
- These symptoms modestly affected physical function and the ability to perform roles (work, hobbies)
- However, there was no difference in patient assessment of global health or overall HRQOL
The primary limitation of the analysis was that smaller sample sizes at later time points reduced statistical power to detect differences between treatment arms, potentially due to disease progression.
In his concluding remarks, Dr. Chen emphasized that for patients with high-risk urothelial carcinoma after radical surgery, adjuvant pembrolizumab versus observation:
- Increases median disease-free survival from 14.2 to 29.6 months
- Causes well-known side effects (fatigue, dyspnea), which modestly impact physical function and the ability to perform certain roles
- Has no impact on overall HRQOL
- These data help inform patient decision-making and the possible need for supportive services
8Presented by: Ronald C. Chen, MD, MPH, Professor, Chair, Radiation Oncology, University of Kansas Medical Center, Kansas City, Kansas
Written by: Rashid K. Sayyid, MD, MSc, Assistant Professor, Urologic Oncologist, Department of Urology at The University of Arizona and Banner University Medical Center, Tucson, AZ – @rksayyid on X during the American Society of Clinical Oncology Genitourinary (ASCO) Annual Meeting held in Chicago, IL between May 29th and June 1st, 2026
Related content: Quality of Life Results from the AMBASSADOR Adjuvant Pembrolizumab Trial - Ronald Chen
Reference:
- Apolo AB, Ballman KV, Sonpavde G, et al. Adjuvant Pembrolizumab versus Observation in Muscle-Invasive Urothelial Carcinoma. N Engl J Med. 2024;391:1217-1228. doi:10.1056/NEJMoa2401726.