Dr. Petrylak began by noting that currently available antibody-drug conjugates containing monomethyl auristatin E payloads have demonstrated significant efficacy in locally advanced and metastatic urothelial carcinoma, but are frequently associated with adverse events including peripheral neuropathy, dermatologic toxicities, and ocular toxicity. He emphasized that these toxicities can negatively impact tolerability and lead to treatment discontinuation, highlighting the ongoing need for more tolerable therapeutic strategies in this disease space.
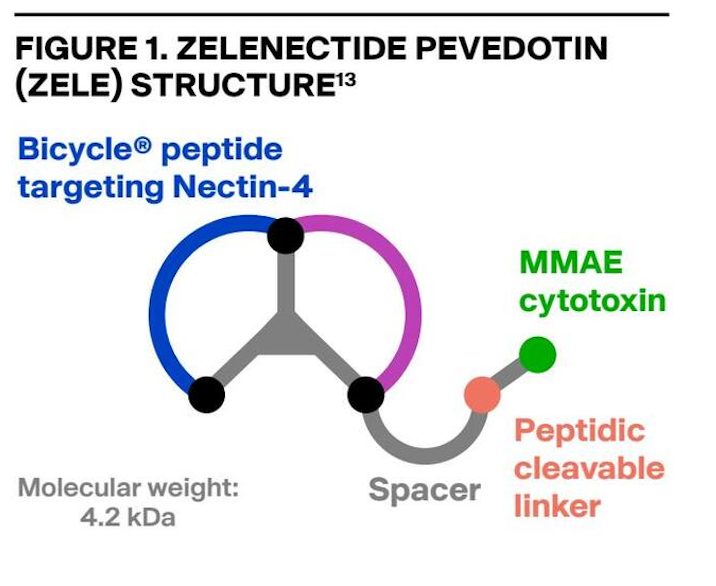
He further discussed Bicycle molecules as a novel therapeutic platform designed to combine the pharmacokinetic and manufacturing advantages of small molecules with the high target specificity typically associated with biologics. Within this context, he introduced zelenectide pevedotin, formerly BT8009, a first-in-class Nectin-4-targeted Bicycle Drug Conjugate linked to MMAE through a cleavable linker. Dr. Petrylak noted that Nectin-4 is highly overexpressed in locally advanced and metastatic urothelial carcinoma, making it an attractive target for selective cytotoxic payload delivery.
The phase 1/2 Duravelo-1 (NCT04561362) dose-escalation and expansion study previously demonstrated encouraging antitumor activity of zelenectide pevedotin in 45 patients with previously treated locally advanced or metastatic urothelial carcinoma.(1)
Duravelo-2 (NCT06225596) includes two cohorts: Cohort 1 evaluating zele plus pembrolizumab in previously untreated platinum-eligible patients, and Cohort 2 evaluating zele monotherapy in patients who had received at least one prior systemic therapy. The current interim analysis focused on Cohort 2 and aimed to optimize zele dosing based on efficacy, safety, pharmacokinetic, and benefit-risk analyses.
Patients in Cohort 2 were randomized 1:1 to receive either:
- Zele 5 mg/m² on Days 1, 8, and 15 of a 21-day cycle
- Zele 6 mg/m² on Days 1 and 8 of a 21-day cycle (Study design presented below)
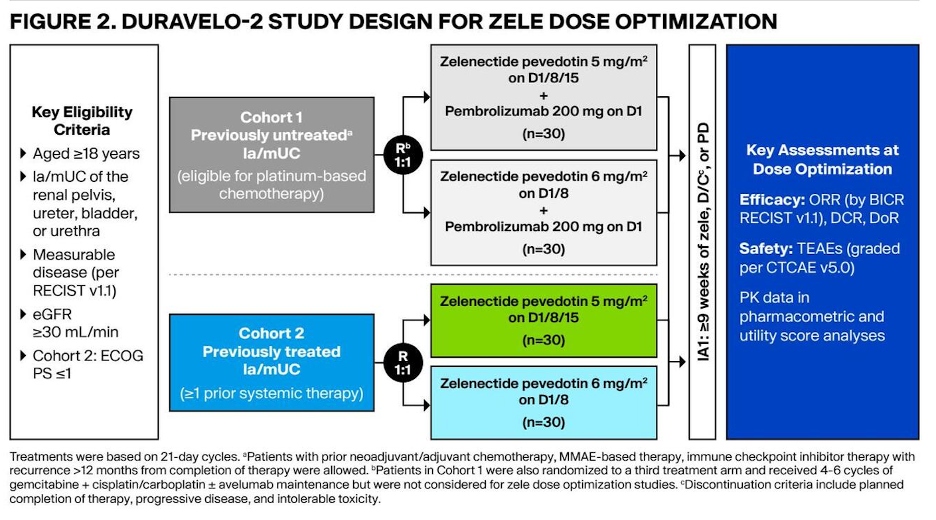
Dose optimization was determined using an integrated benefit-risk assessment incorporating efficacy, safety, utility scoring, and pharmacokinetic exposure-response modeling. Key efficacy endpoints included objective response rate, disease control rate, and duration of response per RECIST v1.1 by blinded independent central review, while safety analyses evaluated treatment-emergent and treatment-related adverse events, including serious adverse events. The efficacy-evaluable population included patients who received at least one dose of study treatment and had measurable disease at baseline.
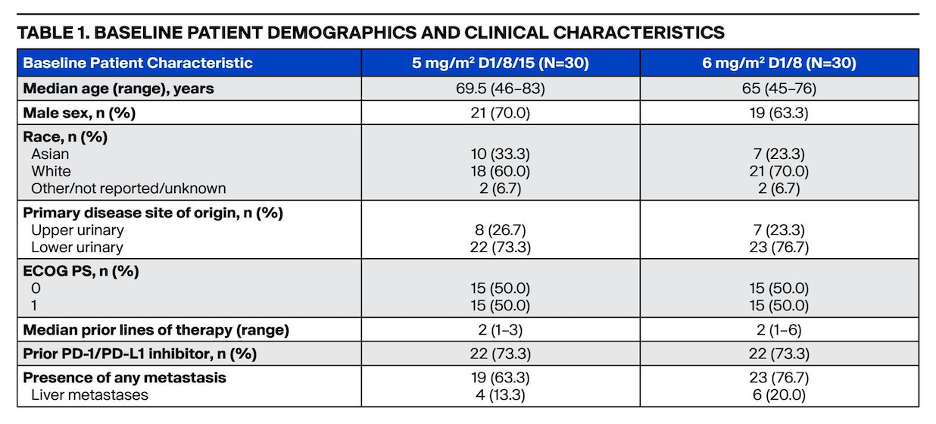
At the time of the interim analysis, patients in the IA1 population had either completed 27 weeks of treatment, experienced disease progression, or discontinued study therapy. As of June 14, 2025, a total of 60 previously treated patients with locally advanced or metastatic urothelial carcinoma had been enrolled, with baseline demographic and clinical characteristics summarized in the table below. Median relative dose intensity was 92.9% in the 5 mg/m² day 1/8/15 cohort and 85.6% in the 6 mg/m² day 1/8 cohort.
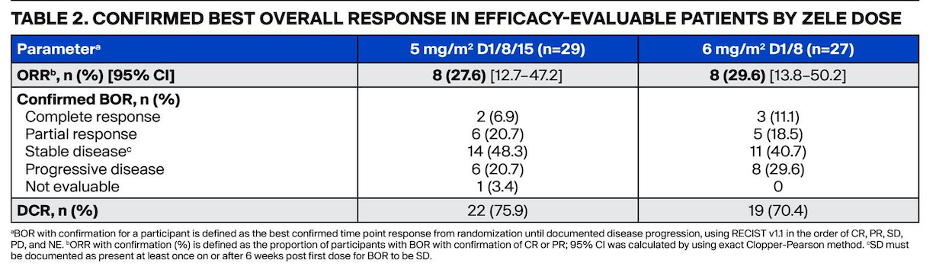
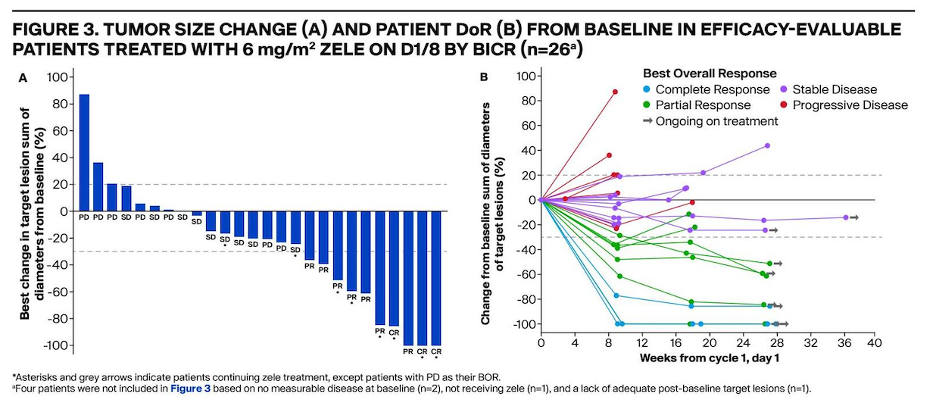
Among randomized and treated patients with measurable disease at baseline, confirmed objective response rates (ORR) by blinded independent central review (BICR) were:
- 27.6% with zele 5 mg/m² (2 complete responses and 6 partial responses; 95% CI 12.7–47.2)
- 29.6% with zele 6 mg/m² (3 complete responses and 5 partial responses; 95% CI 13.8–50.2)
At 27 weeks, eight patients in the 6 mg/m² cohort remained on treatment, including two with stable disease. Additionally, six patients achieved unconfirmed responses, including four in the 5 mg/m² day 1/8/15 cohort and two in the 6 mg/m² day 1/8 cohort. Median time on treatment was 4.8 months in the 6 mg/m² cohort, while median follow-up duration was 6.7 and 6.2 months for the 5 mg/m² and 6 mg/m² cohorts, respectively.
Treatment-related adverse events were reported in 93% of patients in both dose groups, with grade ≥3 adverse events occurring in 47% and 52% of patients treated with the 5 mg/m² and 6 mg/m² regimens, respectively. For the 6 mg/m² schedule, the most common grade ≥3 treatment-related adverse events included decreased neutrophil count and neutropenia (10% each), as well as anemia, asthenia, and ALT elevation (7% each). Importantly, no grade 5 treatment-related adverse events were reported with either regimen.
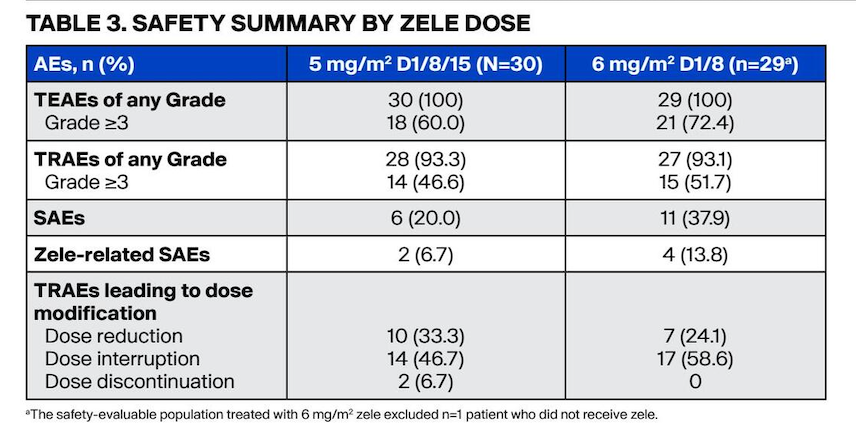
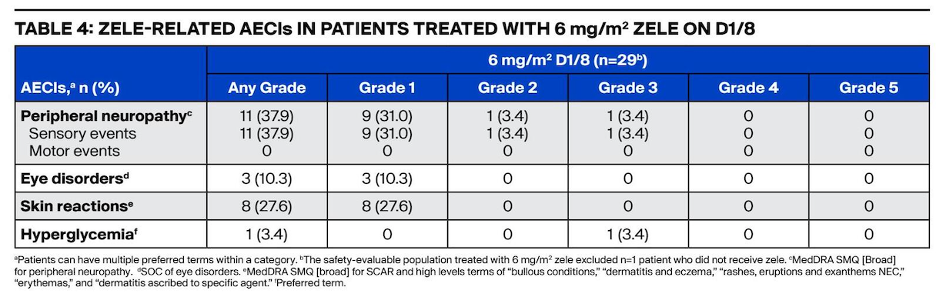
Dr. Petrylak highlighted the favorable tolerability profile of zele, particularly with respect to adverse events commonly associated with Nectin-4–directed ADCs. Notably, no severe treatment-related skin reactions of any grade were observed in either treatment arm. As seen previously peripheral neuropathy of any grade was present in 38% of patientsin the 6 mg/m² schedule. Furthermore, dose reductions and treatment discontinuations related to adverse events occurred in 24% and 0% of patients receiving the 6 mg/m² regimen, respectively. At week 27, approximately one-third of patients remained on therapy.
Dr. Petrylak concluded his presentation with the following key messages:
- The 6 mg/m² dose administered on days 1 and 8 of a 21-day cycle was identified as the optimized zelenectide pevedotin monotherapy regimen based on the overall benefit-risk profile
- Zelenectide pevedotin at 6 mg/m² demonstrated encouraging antitumor activity, with eight patients remaining on treatment at the time of the interim analysis
- Based on the observed safety profile, the 6 mg/m² regimen may offer a safer and more tolerable treatment option with improved combinability and convenience, potentially leading to fewer treatment discontinuations
- Skin toxicities were generally low grade and manageable
- As of June 18, 2025, no cases of Stevens-Johnson syndrome or toxic epidermal necrolysis had been reported among 595 patients treated with zelenectide pevedotin, supporting a differentiated safety profile compared with currently available MMAE-based ADC regimens
Presented by: Daniel Petrylak, MD, Professor of Medicine (Medical Oncology) and of Urology, Yale School of Medicine, Smilow Cancer Hospital, New Haven, CT
Written by: Julian Chavarriaga, MD, Clinical Assistant Professor, Urologic Oncologist, Department of Urology at Penn State Health @chavarriagaj on X during the American Society of Clinical Oncology Genitourinary (ASCO) Annual Meeting held in Chicago, IL between May 29th and June 1st, 2026