(UroToday.com) The 2026 American Society of Clinical Oncology Genitourinary (ASCO) Annual Meeting, held in Chicago, IL, will host the Kidney and Bladder Cancer - Posters. Dr. Yunkai Qie presented Abstract 4593: Urinary tumor DNA-guided de-escalation of systemic immunotherapy in extensive very high-risk non-muscle invasive bladder cancer (NMIBC).
With the emergence of systemic immunotherapy for NMIBC, several large randomized trials, including CREST, POTOMAC, and ALBAN, have evaluated prolonged treatment strategies in patients with high-risk disease. However, the benefit of extended systemic therapy remains heterogeneous and may come at the expense of cumulative toxicity. In this context, investigators evaluated whether urinary tumor DNA (utDNA) negativity after complete response (CR) could support safe treatment de-escalation in patients with extensive very-high-risk NMIBC (VHR-NMIBC).
This study included patients from a prospective cohort with extensive VHR-NMIBC who achieved CR following treatment with the PD-1 inhibitor tislelizumab combined with low-dose paclitaxel. After CR assessment, selected patients underwent low-coverage utDNA testing as part of routine clinical decision-making. Patients with negative utDNA status completed three additional treatment cycles followed by planned discontinuation of systemic therapy and were categorized into the utDNA-guided de-escalation group. Patients who continued treatment beyond this point comprised the longer treatment-exposure cohort.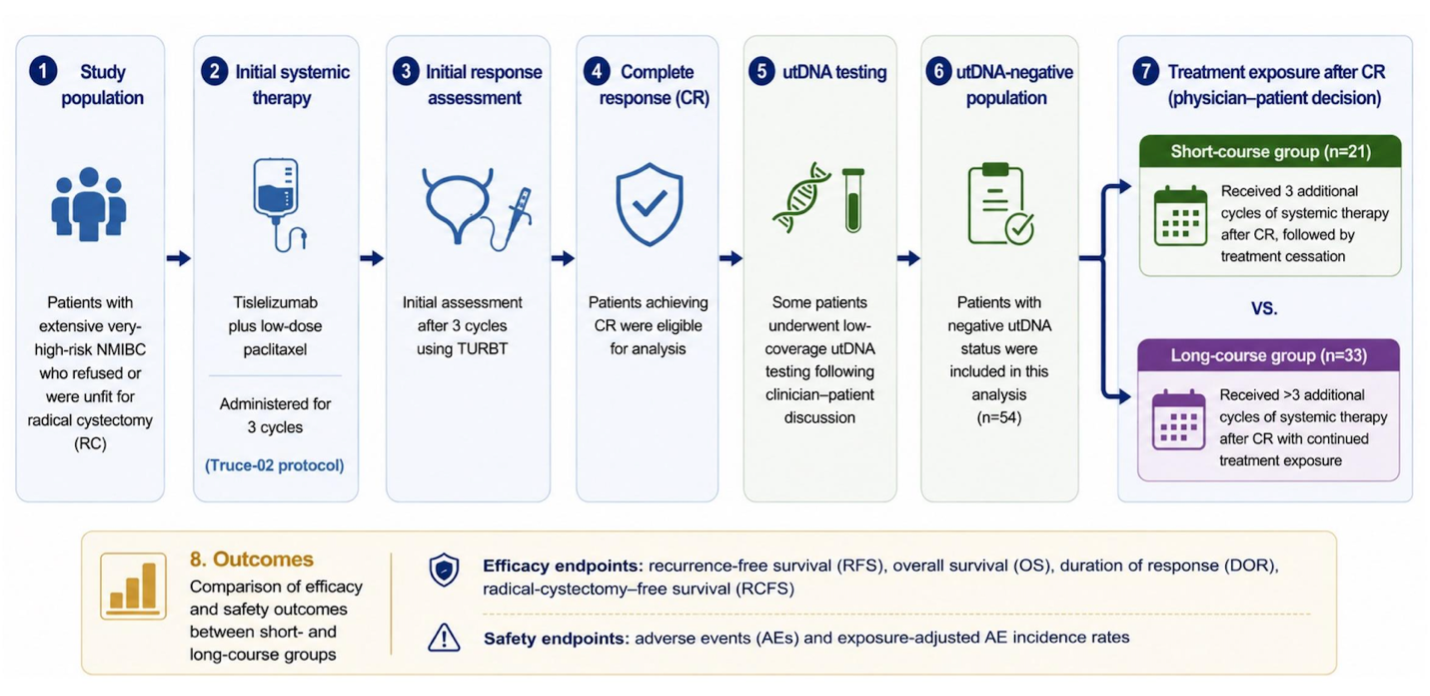
At a median follow-up of 42.8 months, 54 patients achieving CR were evaluable. Among them, 21 patients with negative utDNA completed three additional cycles and subsequently discontinued treatment, whereas 33 patients continued longer-duration systemic therapy.
Across major efficacy endpoints, outcomes appeared comparable between the two groups. No statistically significant differences were observed in:
- Recurrence-free survival (HR 1.37, 95% CI 0.21–8.87; P=0.73)
- Overall survival (HR 2.48, 95% CI 0.12–53.7; P=0.51)
- Duration of response (HR 1.33, 95% CI 0.21–8.50; P=0.76)
However, a difference was observed in radical cystectomy-free survival, favoring the longer treatment-exposure group (HR 4.97, 95% CI 1.03–23.9; P=0.03).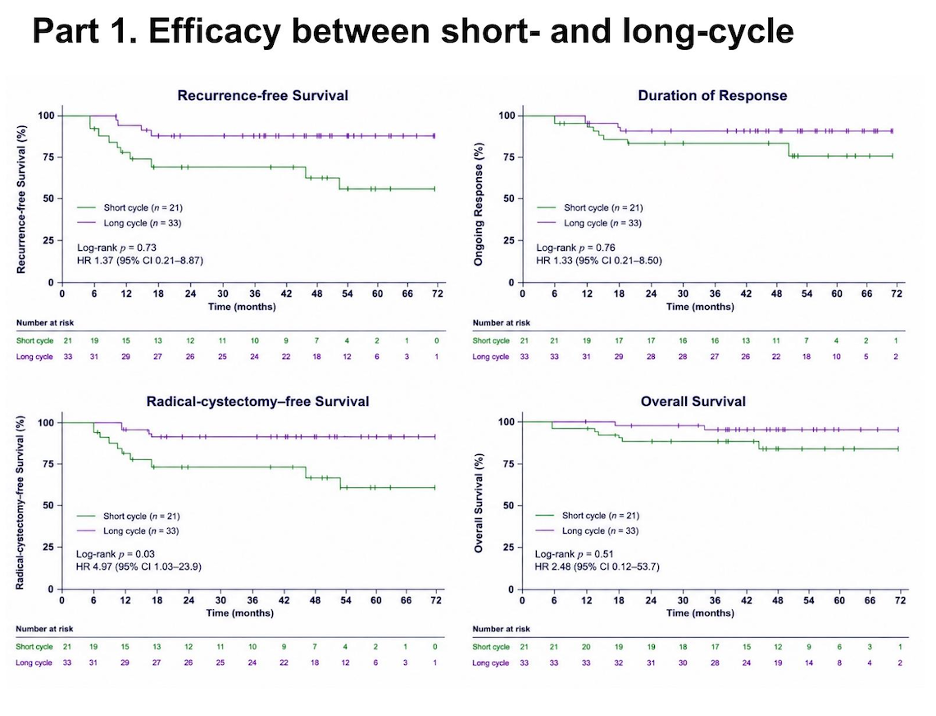
Investigators also highlighted the toxicity implications of prolonged treatment exposure. Patients receiving longer-duration systemic therapy experienced a higher cumulative incidence of any-grade adverse events compared with the de-escalation cohort (88.1% vs 72.5%) and developed a greater number of adverse event types overall (median 5 vs 2; P<0.001). Grade ≥3 adverse events occurred in 2.9% of patients in the de-escalation group versus 9.5% in the prolonged-treatment group, with most higher-grade toxicities occurring during later phases of treatment.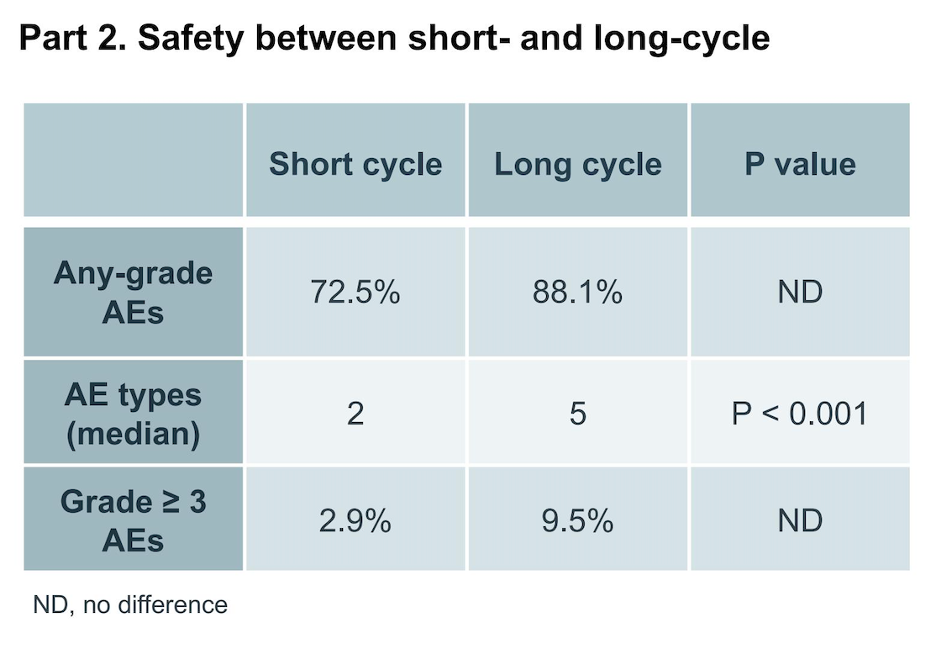
Key Takeaways:
- utDNA negativity following complete response may provide a molecular basis for individualized treatment duration in patients with VHR-NMIBC.
- Early treatment discontinuation guided by utDNA negativity demonstrated comparable recurrence-free survival, overall survival, and duration of response relative to prolonged systemic therapy.
- Longer treatment exposure was associated with greater cumulative toxicity and a higher incidence of grade ≥3 adverse events.
- These findings support the potential role of liquid biopsy–guided treatment tailoring in NMIBC.
- Prospective validation in larger biomarker-driven studies is warranted before implementation into routine clinical practice.
Presented by: Yunkai Qie, MD, The Second Hospital of Tianjin Medical University, Tianjin, China
Written by: Julian Chavarriaga, MD, Clinical Assistant Professor, Urologic Oncologist, Department of Urology at Penn State Health @chavarriagaj on X during the American Society of Clinical Oncology Genitourinary (ASCO) Annual Meeting held in Chicago, IL between May 29th and June 1st, 2026