(UroToday.com) The 2025 American Society of Clinical Oncology (ASCO) Annual Meeting held in Chicago, IL between May 30th and June 3rd, 2025, was host to a New Frontiers in Prostate-Specific Membrane Antigen (PSMA) Radioligand Therapy. Dr. Jorge Garcia discussed ‘hits, misses, and next steps’ in prostate cancer radioligand therapies.
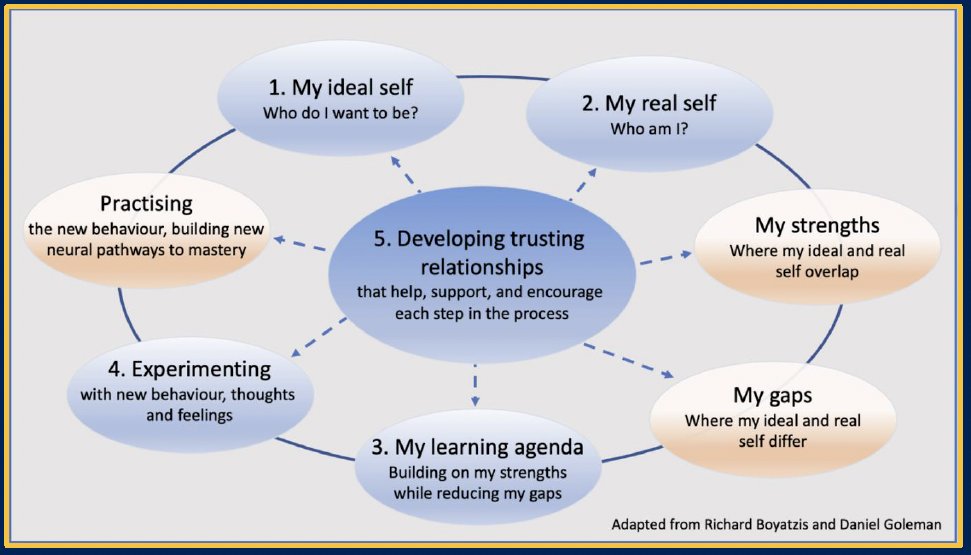
There is a clear intersection between the progress of radioligand therapy in prostate cancer and the intentional change theory, and this can be exemplified as follows
- Ideal self/vision – Who do I want to be?
- Leveraging PSMA to precisely target cancer cells with radioactive payloads
- Real self – Who am I?
- Realities of clinical trials and patient outcomes – celebrating successes and recognizing shortcomings include variability in outcomes
- Learning agenda
- Address challenges by understanding biologic mechanisms of sensitivity and resistance and selecting the ideal patients
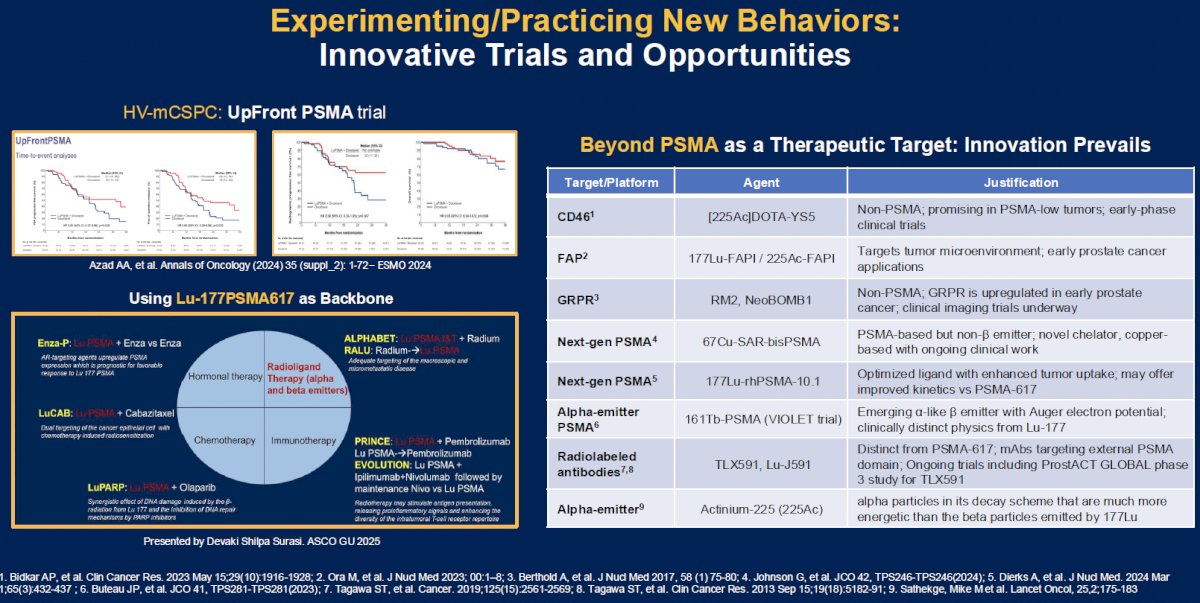
- Experimenting
- Next-generation therapies and innovative trial strategies
- Collaborative relationship
- Across disciplines and continents to drive knowledge into action
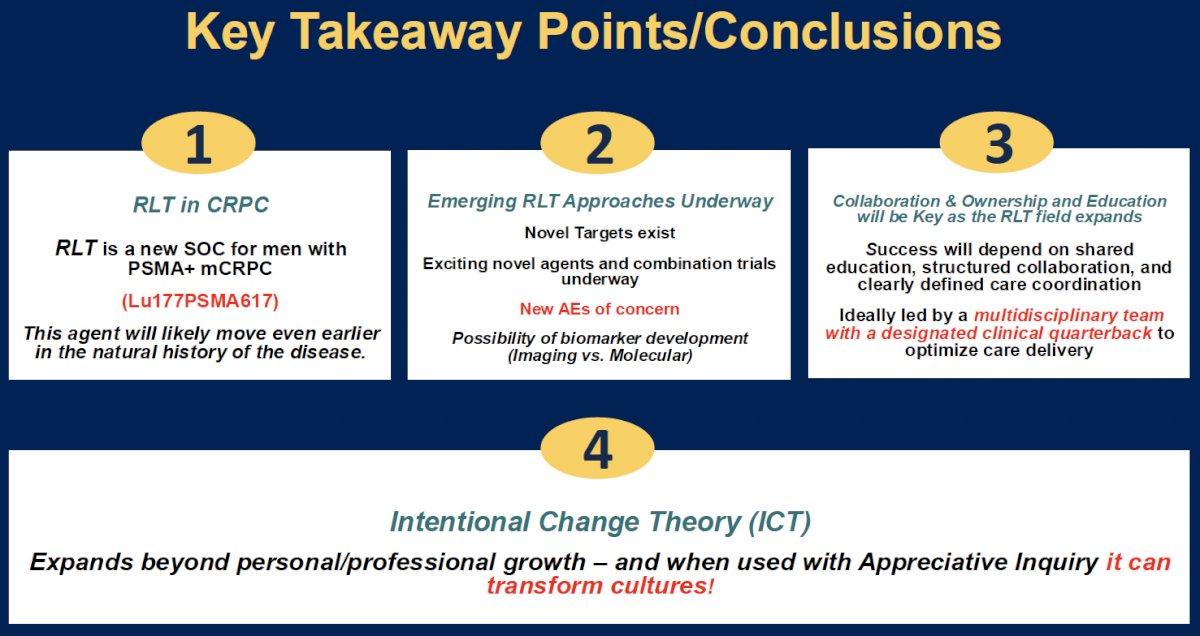
What are the key takeaways from this presentation?
- Radioligand therapy works – it has been validated in phase II/III trials with consistent efficacy across endpoints
- Radioligand therapy is not perfect – biologic and imaging limitations, patient heterogeneity, and access remain major hurdles. Emerging adverse events that could impact the early use of radioligand therapy require further evaluation
- We are learning fast – innovation and collaboration will be key. Ongoing trials are shifting the paradigm by:
- Evaluating radioligand therapy combinations and in earlier settings
- Standardization of imaging
- Evolution in the types of radioligand therapy, SUV criteria requirements, response definitions, and trial eligibility
Dr. Garcia argued that radioligand therapy, in the ‘ideal self’ discovery phase, can achieve outcomes previously thought unattainable by:
- Achieving curative-intent outcomes with minimal therapy exposure and toxicity
- Delivering biologically individualized therapy – treating only those most likely to benefit
- Deploying radioligand therapy early to preempt resistance and tumor transformation
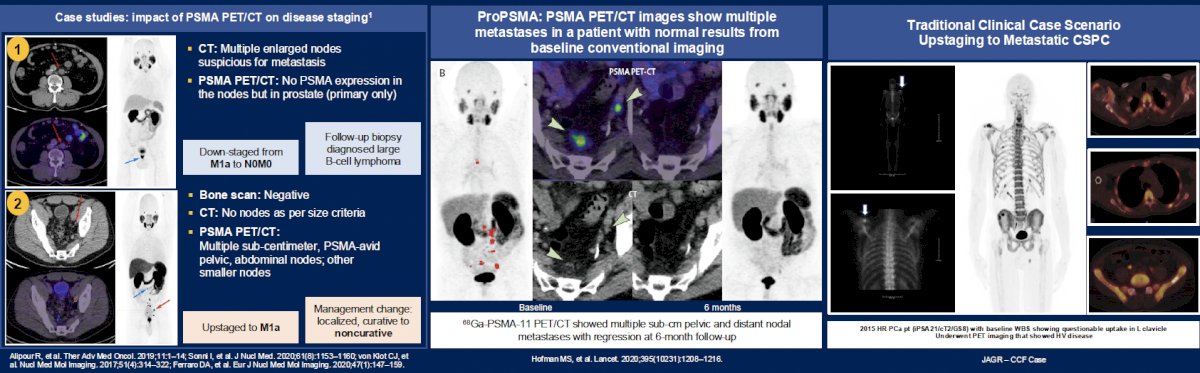
But what about the ‘real self’ discovery phase we find ourselves in? He argued that notable challenges remain. Imaging success has been transformational, but challenges in interpretation and applicability for some remain.
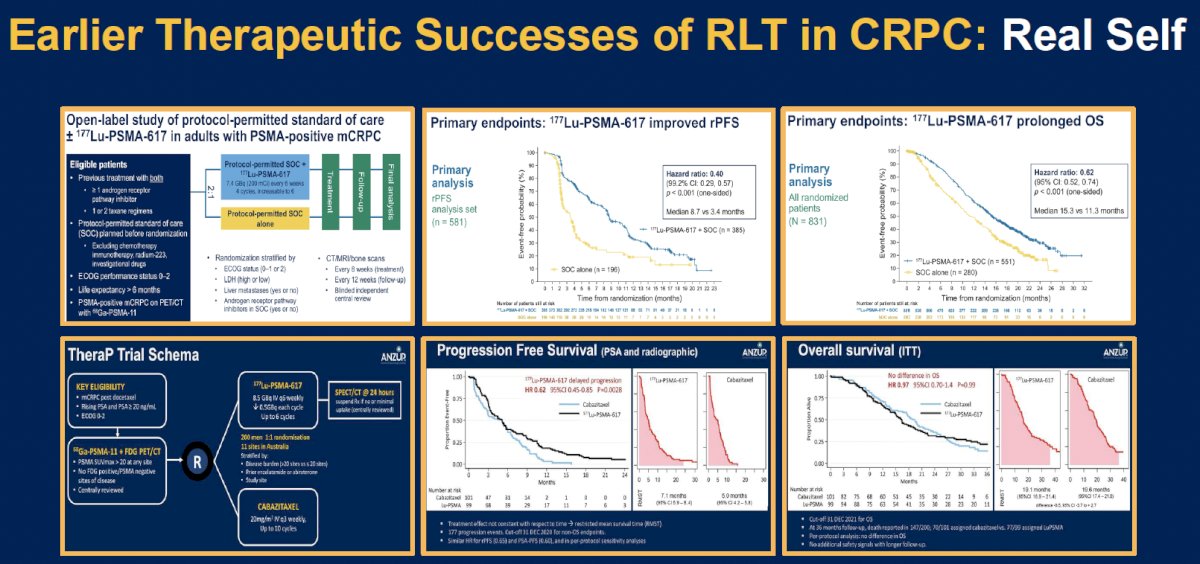
There have been numerous therapeutic successes for radioligand therapy in CRPC:
- 177Lu-PSMA-617 in the post-androgen receptor pathway inhibitor (APR) and taxane setting: VISION and TheraP1,2
- 177Lu-PSMA-617 in the post-ARPI setting: PSMAfore3
- 177Lu-PSMA-617 + enzalutamide in the pre-taxane setting: ENZA-p4
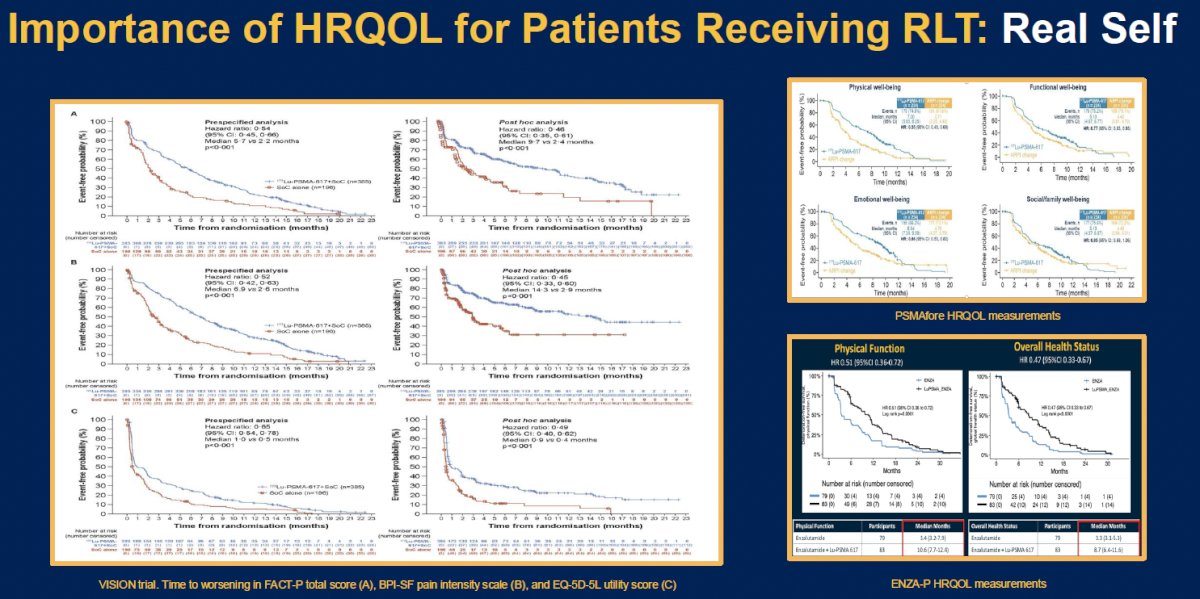
In addition to proven efficacy, PSA and patient-related endpoints have also been met, as highlighted below:
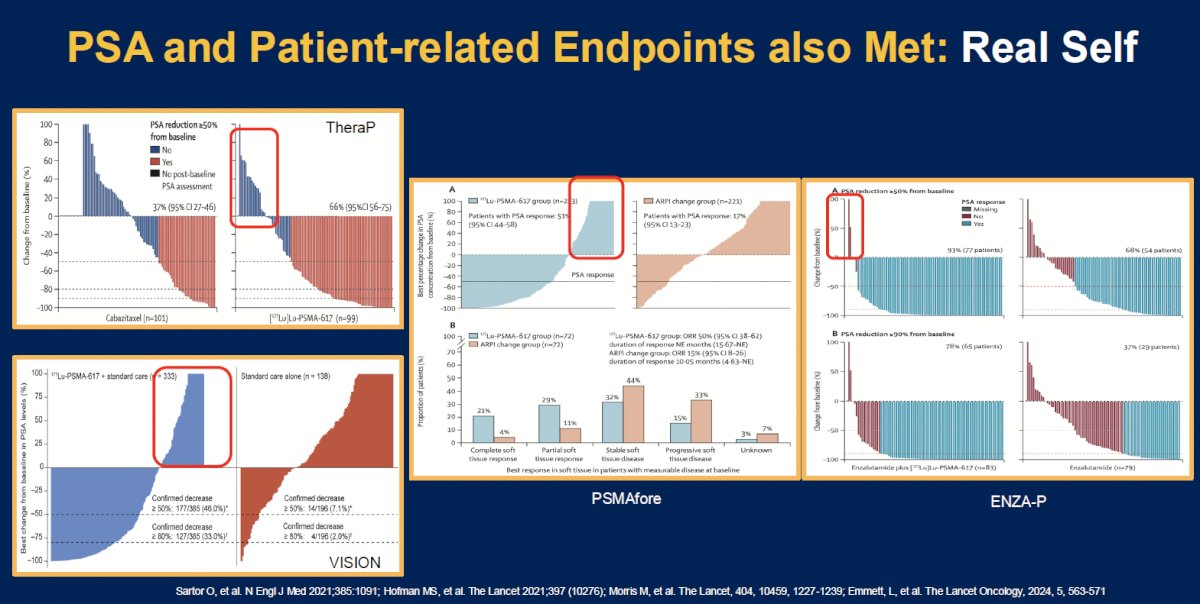
The importance of health-related quality of life for patients receiving radioligand therapy cannot be overstated. mCRPC patients commonly experience significant treatment-related toxicities and, thus, quality of life outcomes become of utmost importance. Encouragingly adding radioligand therapy with 177Lu-PSMA-617 in later line settings appear to improve these quality-of-life outcomes, which may reflect underlying treatment efficacy and reduced disease burden.
How do we ‘bridge’ the vision and reality? We need to recognize current challenges in real self:
- Not every patient benefits from radioligand therapy, with reasons including:
- Heterogeneity of PSMA expression and tumor plasticity
- Biologic mechanisms of resistance
- Challenges in imaging interpretation and biomarker development
Discussing heterogeneity of PSMA expression and tumor plasticity, Dr. Garcia highlighted the following key points:
- The tumor phenotype shifts over time: PSMA expression often decreases as aggressiveness increases
- Patients with tumors that demonstrate high PSMA expression are ideal radioligand therapy candidates
- Low or discordant uptake limited efficacy
- FDG PET complements PSMA PET – it identifies biologically aggressive, PSMA-negative subclones
- Therapy selection must match biology – imaging + molecular biomarkers are needed for treatment precision

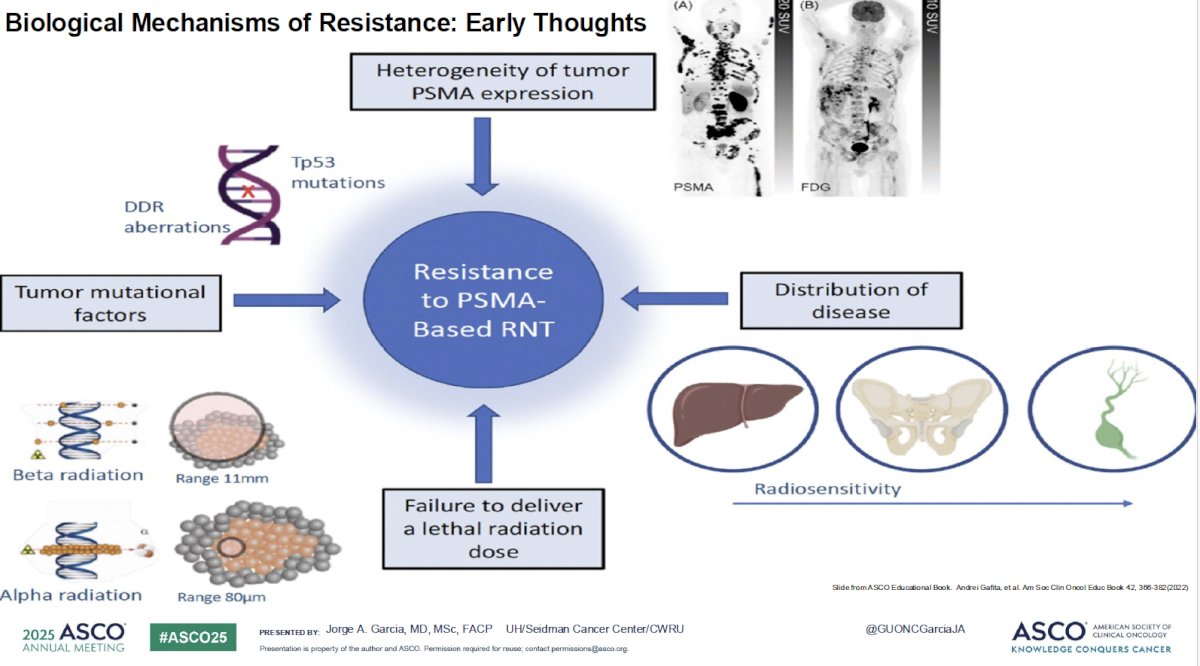
What about biologic mechanisms of resistance? Numerous factors have been correlated with resistance to PSMA-based radioligand therapy:
- Heterogeneity of tumor PSMA expression
- Disease distribution
- Failure to deliver a lethal radiation dose
- Tumor mutational factors
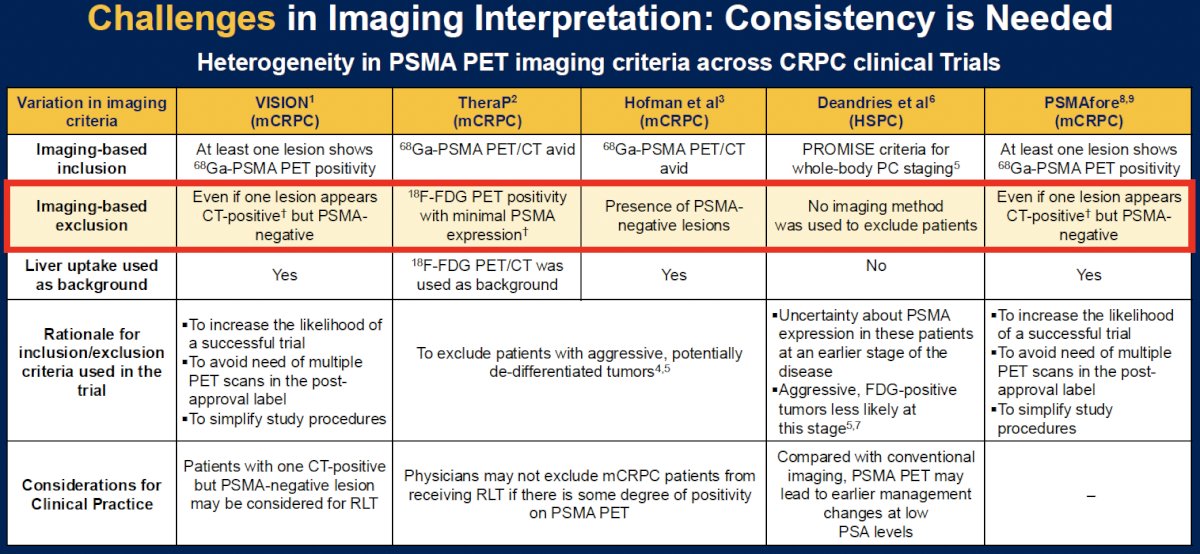
Trials of radioligand therapy have preemptively attempted to exclude patients with heterogenous tumor PSMA expression to maximize the probability of treatment success. As summarized in the table below, VISION excluded patients if they had ≥1 lesions that was CT-positive, but PSMA-negative, and TheraP excluded patients with lesions demonstrating 18F-FDG PET positivity with minimal PSMA expression.
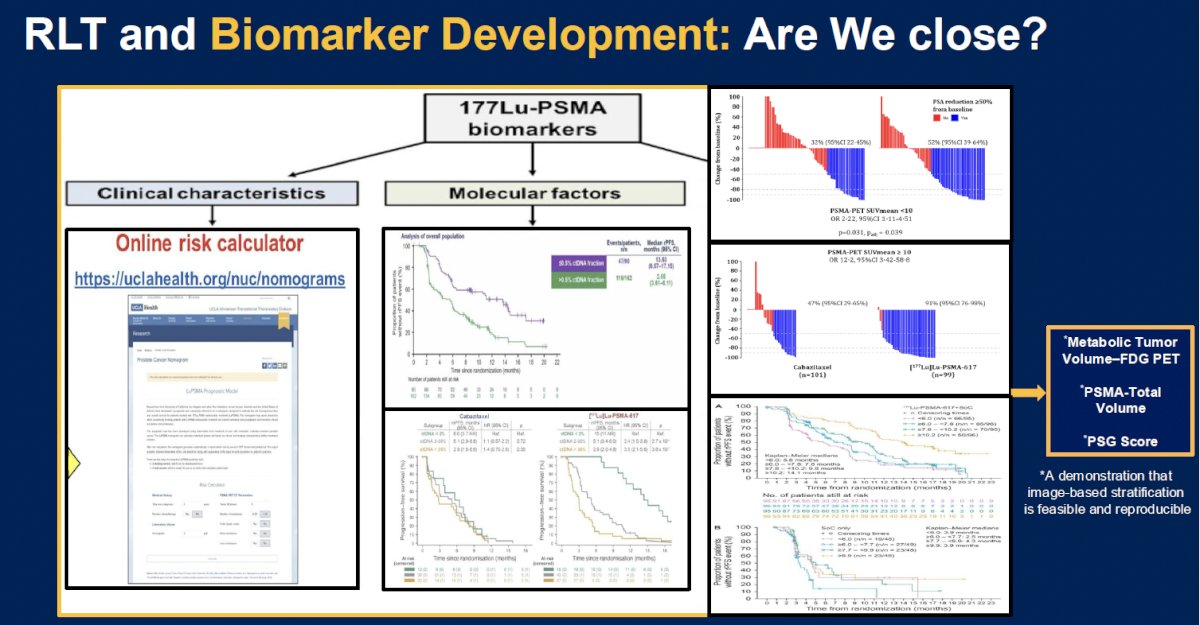
Are we close to biomarker development in radioligand therapy? There are currently online risk calculators of treatment benefit, based on clinical characteristics. Serum molecular factors, such as ctDNA, are being increasingly employed, with patients having low ctDNA fractions demonstrating superior survival outcomes with 177Lu-PSMA-617 therapy. Radiologic imaging variables, including metabolic tumor volume on FDG PET and PSMA total volume are also being employed for treatment selection.
What is currently on the learning agenda for radioligand therapy? We need to ‘reduce gaps and capitalize on our strengths’ by:
- Employing multiparametric models that fuse PET SUV data with genomic, metabolic, and serologic markers that could potentially greatly refine patient selection and early response prediction in radioligand therapy.
- Moving beyond conventional SUV measurements – radiomics and AI-driven analysis techniques promise to extract more predictive information from PSMA PET scans.
- Response-adaptive dosing and therapeutic strategies aimed at escalating treatment in those thought to have stable disease or partial responses (to maximize tumor dose), while sparing those who achieve complete metabolic responses from unnecessary radiation.
- Employing PSMA PET tumor volume (PSMA-TV) and total lesion PSMA uptake (PSMA-TV × SUV_mean) as integrated biomarkers
Dr. Garcia highlighted ongoing, exciting trials of radioligand therapy in this space:
Dr. Garcia concluded his presentation with the following take-home messages:
Presented by: Jorge A. Garcia, MD, FACP, Division Chief, Solid Tumor Oncology, Seidman Cancer Center University Hospitals, Cleveland, OH
Written by: Rashid K. Sayyid, MD, MSc – Robotic Urologic Oncology Fellow at The University of Southern California, @rksayyid on Twitter during the American Society of Clinical Oncology (ASCO) 2025 Annual Meeting, Chicago, IL, Fri, May 30 – Tues, Jun 3, 2025.
References:- Hofman MS, Emmett L, Sandhu S, et al. [(177)Lu]Lu-PSMA-617 versus cabazitaxel in patients with metastatic castration-resistant prostate cancer (TheraP): A randomized, open-label, phase 2 trial. Lancet. 2021; 397(10276): 797-804.
- Sartor O, de Bono J, Chi KN et al. Lutetium-177-PSMA-617 for Metastatic Castration-Resistant Prostate Cancer. N Engl J Med. 2021; 385(12):1091-1103.
- Sartor O, Morris MJ, Chi KN, et al. 177Lu-PSMA-617 versus a change of androgen receptor pathway inhibitor therapy for taxane-naïve patients with progressive metastatic castration-resistant prostate cancer (PSMAfore): a phase 3, randomised, controlled trial. Lancet. 2024 ;403(10328): 112–123.
- Emmett L, Subramaniam S, Joshua AM, et al. ENZA-p: A randomized phase II trial using PSMA as a therapeutic agent and prognostic indicator in men with metastatic castration-resistant prostate cancer treated with enzalutamide (ANZUP 1901). BJU Int. 2021; 128(5):642–651.