(UroToday.com) The 2025 American Society of Clinical Oncology (ASCO) Annual Meeting held in Chicago, IL, was host to the Session State of the Art Lecture: Personalizing treatment for patients with metastatic castration resistant prostate cancer (mCRPC) in 2025. Dr. Wassim Abida delivered a lecture titled: Integrating PARP Inhibitors in the Treatment of Prostate Cancer: Timing, Combination Approaches, and Beyond BRCA1/2.
Dr. Abida began by highlighting that DNA damage repair (DDR) gene alterations are observed in approximately 20–25% of patients with metastatic castration-resistant prostate cancer (mCRPC). These alterations have important therapeutic implications, particularly in guiding the use of targeted agents such as PARP inhibitors.1

DNA repair is maintained through multiple specialized pathways that respond to distinct types of genomic damage. Base excision repair (BER) corrects small base lesions, commonly resulting from oxidative or alkylating stress. Mismatch repair (MMR) addresses base–base mismatches and insertion–deletion loops generated during DNA replication. Nucleotide excision repair (NER) eliminates bulky, helix-distorting lesions such as those caused by ultraviolet radiation. Homologous recombination repair (HRR), a high-fidelity mechanism that relies on genes including BRCA1, BRCA2, ATM, and RAD51, resolves double-strand breaks using a homologous template. In contrast, non-homologous end joining (NHEJ) directly ligates broken DNA ends without a template, making it more error prone. Importantly, PARP inhibitors exploit deficiencies in HRR, particularly in tumors with BRCA1/2 mutations, through synthetic lethality. These pathways and their therapeutic relevance are illustrated below.2

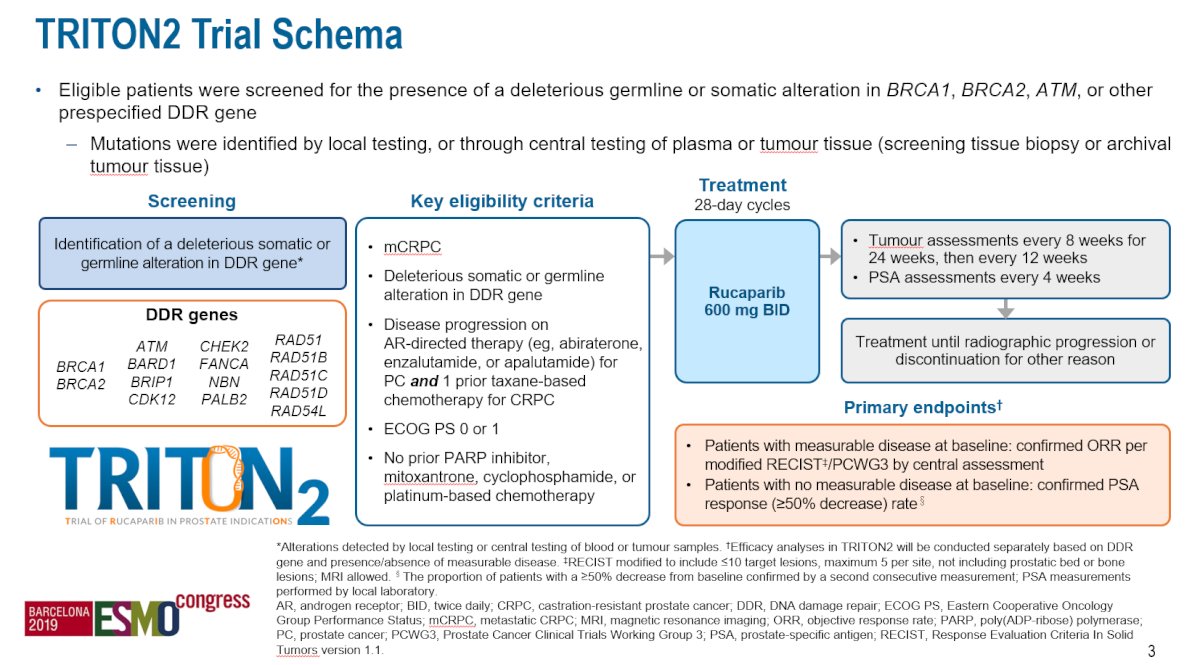
Dr Abida discussed the TRITON 2 trial, a phase 2, open-label study evaluating rucaparib (600 mg BID) in patients with mCRPC who harbor deleterious germline or somatic alterations in DNA damage repair (DDR) genes. Eligible patients had progressed on prior AR-directed therapy and at least one taxane-based chemotherapy, with ECOG PS 0–1. The primary endpoints were objective response rate (ORR) in patients with measurable disease and PSA response (≥50% decline) in those without measurable disease.3 The study design is shown below.
In the BRCA1/2 cohort of the TRITON2 trial, the confirmed objective response rate (ORR) was 51% among the investigator-evaluable population, with 44.6% of patients achieving partial responses. Additionally, the confirmed PSA response rate (defined as ≥50% decline from baseline) was 55%.

Moreover, when stratified by germline versus somatic mutation status. Among the investigator-assessed efficacy population, patients with somatic BRCA1/2 alterations had a similar ORR (43.9%; 95% CI: 28.5–60.3) compared to those with germline alterations (42.9%; 95% CI: 21.8–66.0). Similarly, PSA response rates were also slightly higher in patients with somatic mutations (61.7%; 95% CI: 45.5–75.6) versus germline mutations (50.7%; 95% CI: 38.6–62.8).


The PROfound trial was a phase III randomized study evaluating olaparib in patients with mCRPC who had progressed on prior novel hormonal agents and harbored HRR gene alterations. Patients were divided into two cohorts: Cohort A included those with BRCA1, BRCA2, or ATM alterations (n=245), and Cohort B included patients with other HRR gene alterations (n=142). Within each cohort, patients were randomized 2:1 to receive olaparib (300 mg BID) or physician’s choice of enzalutamide or abiraterone. The primary endpoint was radiographic progression-free survival (rPFS). Notably, Crossover to olaparib was permitted upon progression in the control arm.5

The PROfound study demonstrated a significant improvement in rPFS for patients in Cohort A (those with BRCA1, BRCA2, or ATM alterations) treated with Olaparib. The hazard ratio for rPFS was 0.34 (95% CI, 0.25–0.47; P < 0.001), indicating a 66% reduction in the risk of progression or death with olaparib in this biomarker-selected population.5

Similarly, treatment with olaparib was associated with a 31% reduction in the risk of death compared to physician’s choice of ARPI. The hazard ratio for overall survival was 0.69 (95% CI, 0.50–0.97; two-sided P = 0.02).

There was a significant improvement in rPFS in both Cohorts A and B for patients with HRR-mutated mCRPC treated with olaparib compared to the control arm. These results led to FDA approval of olaparib in May 2020 for this population.
However, when analyzing the PROFOUND data gene by gene, the median rPFS benefit was less pronounced for patients with non-BRCA mutations such as ATM and CHEK2, suggesting limited activity of olaparib in these subgroups, as shown below.5

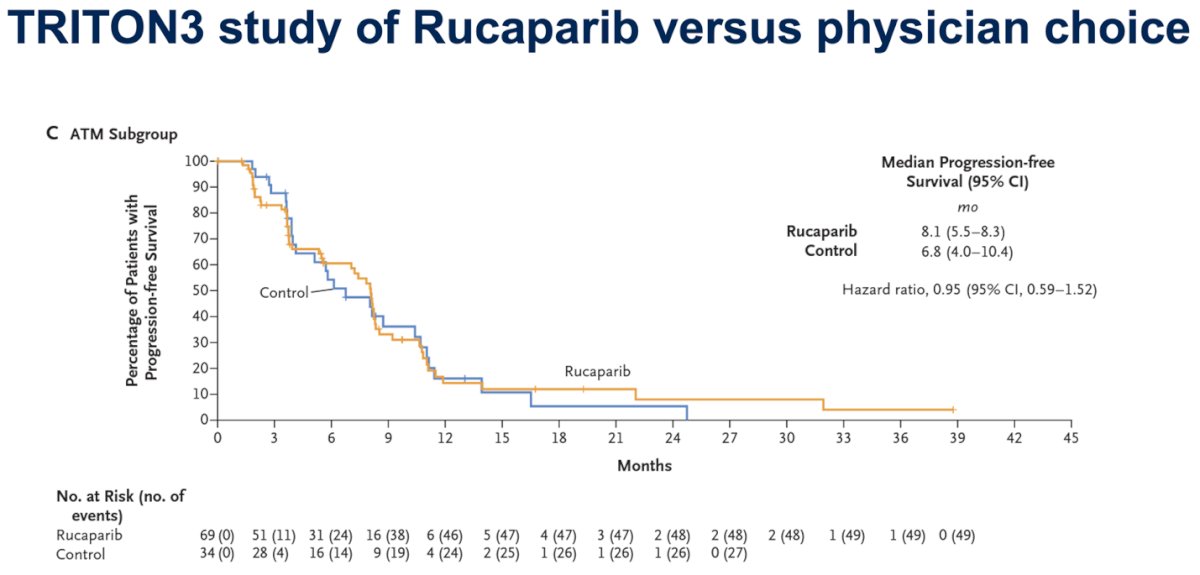
The TRITON3 trial compared rucaparib versus physician’s choice of therapy in men with mCRPC and DDR gene alterations. Notably, in the ATM-mutated subgroup, rucaparib did not demonstrate a clear benefit over control therapy, with a median rPFS of 8.1 months vs 6.8 months (HR 0.95; 95% CI, 0.59–1.52), indicating limited efficacy in this population.4
Dr. Abida emphasized that rucaparib and olaparib are appropriate treatment options for patients with HRR-mutated mCRPC who have progressed following at least one ARPI. The greatest clinical benefit is observed in patients with BRCA2 or BRCA-related gene mutations, such as PALB2. In contrast, there is no consistent evidence of benefit in patients with ATM mutations.
Combination of PARP inhibitors with ARPI in non-DDR-mutated mCRPC PROpelThe PROpel Phase 3 trial evaluated the combination of abiraterone plus olaparib versus abiraterone alone as first-line therapy in mCRPC. Patients were unselected for HRR mutation status, though exploratory testing was conducted via plasma or tumor NGS. Prior docetaxel for mHSPC was allowed, but prior ARPI was not, with about 25% of participants having received prior docetaxel.6
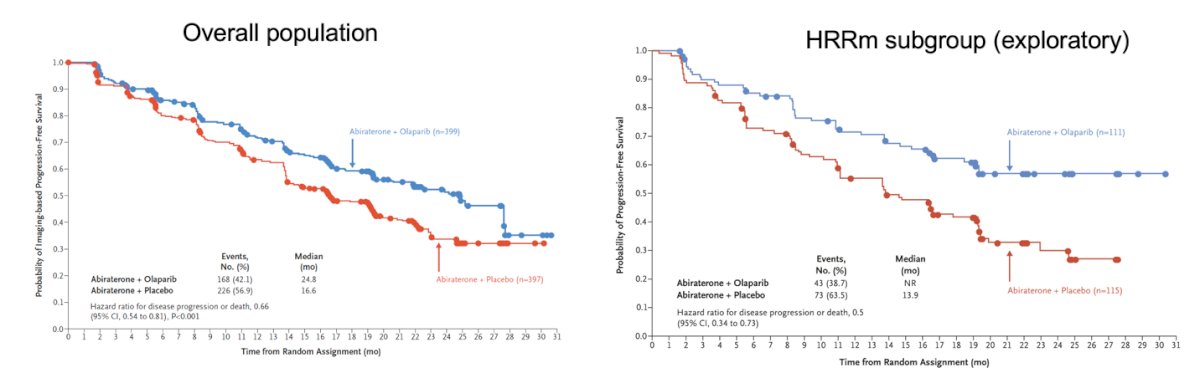
Dr. Abida highlighted that in the overall population of the PROpel trial, the combination of abiraterone and olaparib led to a significant improvement in rPFS compared to abiraterone plus placebo, with a hazard ratio for disease progression or death of 0.66 (95% CI, 0.54–0.81; p<0.001). This benefit was even more pronounced in the HRR-mutated subgroup, where an exploratory analysis showed a hazard ratio of 0.50 (95% CI, 0.34–0.73).
The MAGNITUDE phase 3 trial evaluated the combination of abiraterone plus niraparib versus abiraterone alone in the first-line treatment of patients with mCRPC. Prior exposure to docetaxel or ARPI was allowed but not required (~20% had prior docetaxel, ~3% had prior ARPI). Patients were prospectively stratified into HRR-mutated and non-HRR-mutated cohorts. There was a significant improvement in rPFS both in the BRCA1/2 subgroup and in the overall HRR+ Cohort.7

The TALAPRO-2 phase 3 trial evaluated enzalutamide alone versus enzalutamide combined with talazoparib in the first-line setting for mCRPC. Prior use of docetaxel (~25%) or ARPI (~5%) was allowed but not required. The trial prospectively stratified patients by HRR mutation status.8 This study also showed a significant improvement in rPFS in patients with any HRR gene alteration (HR for disease progression or death, 0.45 (95% CI, 0.33-0.61, P<0.0001).

Notably, the magnitude of rPFS improvement with PARP inhibitor combinations followed a clear hierarchy by gene subgroup: the greatest benefit was observed in patients with BRCA mutations, followed by those with PALB2 alterations. CDK12 and ATM clusters showed more modest effects, while the benefit was least pronounced or absent in patients with other non-BRCA HRR gene alterations.8

Dr Abida highlighted that combining PARP and ARPI is an appropriate strategy for patients with HRR-mutant first-line mCRPC. The greatest benefit is consistently seen in patients with BRCA2 and related gene mutations (PALB2), while the benefit in patients with ATM mutations remains unclear, despite regulatory approvals for agents like olaparib and enzalutamide plus talazoparib in this setting. Notably, the efficacy of this combination in ARPI-pretreated patients is uncertain, and few patients are truly ARPI-naïve by the time they develop castration resistance. There may also be potential PFS benefit in CDK12-mutated disease.
AR inhibition has been shown to modulate the expression of HRR genes in prostate cancer cell lines, providing a rationale for combining ARPI and PARPi even in HRR-proficient settings. Preclinical studies have demonstrated that this combination can exert a synergistic effect in some HRR-intact prostate cancer models. Building on this, several clinical trials are investigating ARPI and PARPi combinations in non-HRR-mutated mCRPC. However, results have been mixed so far, and this approach remains investigational.
Ongoing studies and future directionsDr. Abida highlighted the evolving landscape of PARP inhibitor strategies in prostate cancer, emphasizing efforts to move their use earlier in the disease course for DDR-mutant patients, including trials in metastatic castration-sensitive prostate cancer (mCSPC) such as TALAPRO-3, AMPLITUDE, and EVOPAR01, and in high-risk localized disease with the NEPTUNE study. He also noted ongoing investigations of PARPi combinations in non-DDR-mutated prostate cancer, including PARPi plus ARPI in mCSPC (TALAPRO-3 and EVOPAR01), PARPi combined with radioligand therapy, and early-phase studies exploring PARPi with other DNA repair inhibitors.
Dr Abida concluded the presentation with the following key takeaway points:
- PARP inhibitors are standard of care, effective therapy for a subset of patients with genomic alterations in DDR genes
- All patients with metastatic prostate cancer should have DNA testing
- Benefit is greatest in patients with homologous recombination repair (HRR) gene alterations including BRCA2 and PALB2
- The combination of PARP inhibitors with ARPI in patients without DDR gene mutations remains investigational
Presented by: Wassim Abida, MD, PhD, Genitourinary Oncologist at The Memorial Sloan Kettering Cancer Center, New York, NY.
Written by: Julian Chavarriaga, MD – Urologic Oncologist at Cancer Treatment and Research Center (CTIC) via Society of Urologic Oncology (SUO) Fellow at The University of Toronto. @chavarriagaj on Twitter during the American Society of Clinical Oncology (ASCO) 2025 Annual Meeting, Chicago, IL, Fri, May 30 – Tues, Jun 3, 2025.
Reference:
- Robinson D, Van Allen EM, Wu YM, Schultz N, Lonigro RJ, Mosquera JM, et al. Integrative clinical genomics of advanced prostate cancer. Cell. 2015;161(5):1215–28.
- Jalal S, Earley JN, Turchi JJ. DNA repair: from genome maintenance to biomarker and therapeutic target. Clin Cancer Res. 2011;17(22):6973–84.
- Abida W, Campbell D, Patnaik A, Shapiro J, Sautois B, Vogelzang NJ, et al. Rucaparib in men with metastatic castration-resistant prostate cancer harboring a BRCA1 or BRCA2 gene alteration. J Clin Oncol. 2020;38(32):3763–72.
- Sandhu S, Mateo J, Heidenreich A, Nishiyama H, Li J, Oya M, et al. Rucaparib for patients with metastatic castration-resistant prostate cancer associated with homologous recombination deficiency: primary analysis of the phase 3 TRITON3 study. Lancet. 2023;401(10374):213–23.
- de Bono J, Mateo J, Fizazi K, Saad F, Shore N, Sandhu S, et al. Olaparib for metastatic castration-resistant prostate cancer. N Engl J Med. 2020;382(22):2091–102.
- Clarke N, Wiechno P, Alekseev B, Sala N, Jones R, Kocak I, et al. Olaparib combined with abiraterone in metastatic castration-resistant prostate cancer: a randomized, double-blind, placebo-controlled, phase 3 trial. Lancet Oncol. 2023;24(3):347–57.
- Smith MR, Scher HI, Sandhu S, Efstathiou E, Lara PN Jr, Yu EY, et al. Niraparib in combination with abiraterone acetate and prednisone for metastatic castration-resistant prostate cancer in men with or without homologous recombination repair gene alterations: a randomized, placebo-controlled phase 3 trial. Lancet Oncol. 2022;23(9):1290–300.
- Agarwal N, Loriot Y, McGregor BA, Dreicer R, Drake CG, Dorff TB, et al. TALAPRO-2: Talazoparib plus enzalutamide versus placebo plus enzalutamide in patients with metastatic castration-resistant prostate cancer—A phase 3 trial. Lancet. 2023;401(10374):205–12.
- Li L, Karanika S, Yang G, Wang J, Park S, Broom BM, Manyam GC, Wu W, Luo Y, Basourakos S, Song JH, Gallick GE, Karantanos T, Korentzelos D, Azad AK, Kim J, Corn PG, Aparicio AM, Logothetis CJ, Troncoso P, Heffernan T, Toniatti C, Lee HS, Lee JS, Zuo X, Chang W, Yin J, Thompson TC. Androgen receptor inhibitor-induced "BRCAness" and PARP inhibition are synthetically lethal for castration-resistant prostate cancer. Sci Signal. 2017 May 23;10(480):eaam7479. doi: 10.1126/scisignal.aam7479. PMID: 28536297; PMCID: PMC5855082.